
Cardioliths in 19th century medical literature
- DOI
- 10.1016/j.artres.2018.05.005How to use a DOI?
- Keywords
- Heart; Thrombus; Cardilith; Auguste Sheridan Delépine
- Abstract
During 19th century the term “cardiolith” was widely used to describe a cluster of cardiac entities that could cause sudden death. Blood clots, polypoid growths, microorganisms and inflammation were implicated. Scientists of the era described formations that could enter any heart chamber after having been formed in any portion of the cardiac substance and could provoke a deadly thrombus or embolus. While pathologist and bacteriologist Auguste Sheridan Delépine (1855–1921), was the first who used the term “cardiolith” in his treatise “Description of a cardiolith” in 1890, a series of researchers noted the phenomenon, forming the “School of Cardiolithists”.
- Copyright
- © 2018 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
The term “cardiolith”, deriving from the two ancient Greek words for heart “cardia” (Greek: καρδιά) and stone “lithos” (Greek: λίθος), was widely used in 19th century medical literature to describe solid (concrete) formations inside the heart.1 Cardiologists, anatomists, surgeons and pathologists of the 19th century with their research, based mostly on necropsy, confirmed the existence of a series of factors, capable to form concrete formations in the heart (Fig. 1) such as blood clots, polypoid growths, microorganisms, or tumours which could penetrate the heart myocardium, or enter any of its chambers.2,3
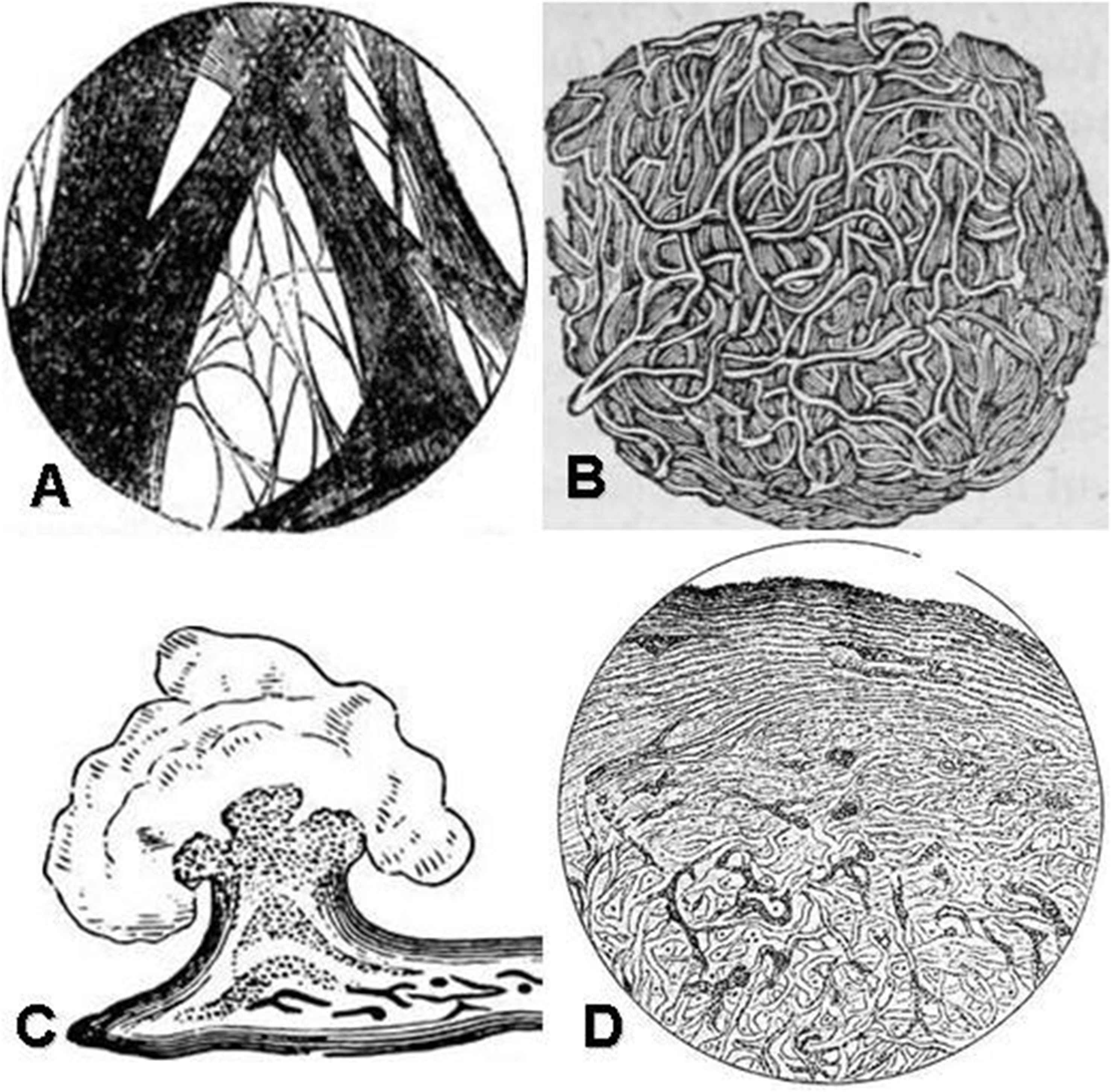
(A) A portion of fibrin, showing its fibrous structure, by Charles Alfred Lee, in Human Physiology for the Use of Elementary Schools, 1854. (B) Fibrinous throbi, vintage engraving. (C) A cardiolith due to acute endocarditis of the mitral valve, vintage engraving. (D) Section of organizing cardiac thrombus. At hte surface laminates blood clot with columns of cell between the laminae; the deeper part of the clot not laminated, transvered by embryonic vessels. Voelcker AF in Transactions of the Pathological Society of London, 1893.
Although the medical phenomenon of body fluids’ coagulation leading eventually to the formation of a “thrombus” (Greek: θρόμβος, clot), preoccupied ancient Greek, Greco-Roman and Byzantine medico-philosophers and physicians,4,5 the old term was neglected and the medical terms “heart lithiasis”, “cardiac concretion” and “cardiolith” became in vogue during 19th century.2 The enthusiastic supporters of the new lucrative, descriptive and more accurate term “cardiolith” formed a school in cardiology which may named “the Cardiolithists school”, introducing a novel pathological entity in 19th century cardiology even though blood clots were already an existent cluster on cardiac pathology.
The School of Cardiolithists
It all started when the physician William J. Goodwin mentioned in 1700 a case of polyform concretion of the heart and at the same time he reported several cases of heart stones (lithiasis).6,7 Although the term “stone” was not previously in use, “cardiac polyps” (Latin: polypo cordis) was first referred half a century earlier by Dutch surgeon Nicolaas Tulp (1593–1674) in 1640’s, while Italian physician Fabrizio Bartoletti (1576–1630) may have preceded him in the use of the term, proposing polyps to result from compacted humours solidifying due to the “heat” of the heart. Italian physician and biologist Marcello Malpighi (1628–1694) published his treatise “De Polypo Cordis” in 1966, using the exact term which was introduced by Tulp recognized fibrinogen.8 Since the dawn of the 18th century, a plethora of medical scientists described formations that could enter any heart chamber after having been formed in any position of the cardiac anatomic area and could provoke, in most cases a fatal embolus.2
In 1826, the British surgeon Henry Vernon provided a lengthy report of a case of obstruction to the passage of blood through the right auriclo-ventricular opening of the heart from a fibrous concretion, which was entangled under the tendinous cords of the tricuspid valve. He had observed that the ossification of the heart, as he had named the phenomenon, had been appearing in patients from sixty years old and upward, who had been previously in robust active health. This morbid condition had been presenting with mental agony and distress, insomnia, attacks resembling syncope, and inability to feed. The symptoms were lasting from two to eight weeks before death. The only method to unveil the concrete formations was, according to him, the post-mortem examination.9 In his turn, Isidore Bricheteau (1789–1861), physician in Necker’s Hospital in Paris, reported in 1834 a similar concretion of a fibrous character. Two years later, in 1836, Aubrey observed first that fibrous concretions in vessels could cause obstruction to the circulation. He believed that they were coagulations formed due to an infection.2
In 1838, H.M. Hughes reported first eleven cases, while Hardy, the same year, attributed their formation to a vegetable ferment.10 The following year, the French physician Jean-Baptiste Bouillaud (1796–1881) mentioned that the concretions found in his patient were formed by blood alone.9 In 1848, the physician G. Sprague in Chicago, noted that he had discovered fibrinous concretions in the heart, extending into the pulmonary artery and aorta with extensive hepatization of both lungs. In 1852, the Italian physician Barbieri published in Gazzetta Medica Italiana, a case, in which a fibrous polyp was extended from the ventricle through the aortic orifice. In 1858, J. Hausley reported a death from a fibrous concretion in the right heart, declaring that the presence of such solid formations in the right, was less frequent than in the left heart.2 Finally, the British physician John William Ogle (1842–1905) reported in 1862 the largest known cardiolith, as a globular formation, one inch in diameter, lying loose within the left auricle of the heart, fibrous in character, while the patient presented an induration of the suprarenal capsules.11,12
Furthermore, 19th century researchers connected somehow the presence of cardioliths with an infectious agent. Thus, in 1869, Barbancy in Paris was the first to report fibrous concretions as due to pneumonia. In 1870, Joseph Fayrer (1824–1907), professor of midwifery in Calcutta, described a case of a patient, whose death was due to fibrinous concretions in the right side of the heart, while the patient was suffering from “urethral fever”. Five years later, the French physician Henri-Jules Rendu (1844–1902) observed also concretions in patients suffering from tuberculosis. In 1887, W.C. Chaffey in London was the first to connect fibrous deposits of the heart with diphtheria.2
Faure in 1864 undertook an experimental research concerning fibrinous clots and the products of inflammation. In the following years several physicians published their work concerning cardiac lithiasis. Garstang in 1852, Richardson in 1855, Blondet in 1857, Monard in 1867, Lawson in 1873, Baker in 1874, Hattute in 1875, and Maycock in 1888, wrote voluminously upon the subject.2
However, the distinguished pathologist and bacteriologist Auguste Sheridan Delépine (1855–1921) (Fig. 2), was the first to coin the term “cardiolith” in his treatise “Description of a cardiolith” in 1890.13,14 Delépine tried to save a cyanotic five year old girl, with rapid respiration and weak pulse. After her death, during her autopsy he had discovered a cardiac stone. An unusual thickness of the myocardium in the neighbourhood of the calculus was noted, a great number of columnae carneae and tendinous bands, encroaching upon the ventricular cavity. The anterior part extended beyond the anterior papillary muscle, whereas the posterior was nearly in contact with the posterior papillary muscles. The cardiolith occupied the space existing between the tricuspid valve and the ventricular wall externally. Delépine had also drawn some descriptive plates to demonstrate the cardiolith, and forged the idea of such a schematization (Fig. 3).13
Auguste Sheridan Delépine. Photogravure after Lafayette Ltd.

The two Delépine’s plates presenting the cardiolith, painted by Delépine himself in 1890.
Discussion
The classification of the fibrous concretions in the heart, a quite common pathology in 19th century medical literature, included blood clots, polypoid growths, microorganisms and inflammation. Nucleus meant in this era that a hard central formation was present, it meant that any foreign body (extra cardiac) may have entered the substance of the heart, or any of its chambers.
A nucleus (nucleus meant at the era a hard central formation) was present, meant that any foreign body (extra cardiac) may have entered the substance of the heart, or any of its chambers. Cardioliths could enter any heart chamber after having formed in any portion of the cardiac substance, and at once become foreign bodies to be classed. Apart from cardioliths’ schematization, their circulation inside the cardiovascular system had been also observed.2
The removal of cardioliths (intramyocardial or within the chambers) became possible in the early 20th century. Cardiologists should attempt to remove them when they cause serious trouble, while the x-ray was considered to greatly aid in determining their presence.15 Despite the fact that the “School of Cardiolithists” never really existed, its legacy still echoes in cardiology, as all those scientists have tried to unearth the secrets of cardiac concretions, to determine a classification among them, to introduce the idea of an extra cardiac body and to systematise a pathologic entity of a great importance.
Lithos in Greek is the term used for an earth’s stone. Ancient Greek and Byzantine scholars suggested the hypothesis of fluid coagulation, resulting to the formation of intra-circulatory stones, introducing the concept of blabber stones, urolithiasis, cardiolithiasis and lung embolism.5,16 “Cardiolithists” most probably desired to nominate this knowledge by adopting the ancient term. The term was still in use in 1920’s, gaining several other nominations. Thus when the concretions were found in veins, they were named “phleboliths”, in arteries “arterioliths”, and as mentioned, in heart “cardioliths”.17 Still, in the following years, the term was gradually abandoned, and other names were used, like “calcified thrombi”, soon returning to the oldest Greek term of thrombus.17 While the definition of a “lithos” was confined in antiquity to the coagulation of fluids, the term thrombus acquired a more complex character, containing the mixture of other substances too. Since the 14th century, when translations of ancient Greek medical treatises became available, Greek-derived medical terminology flowed into international nomenclature.18,19 The renaissance marked the rebirth of Greek terminology in medicine admixed with Latin. This incorporation of Greek terms is thought by some to have been one of the lasting contributions of romantic medicine.20 While it was used predominantly by those with a classical education, the passion of ancient Greeks for a perfect description when spoken terms were used, founded an indelible basis for nomenclature. Thrombus as a medical concept included elements of both the humoral and atomic theories as described by Leucippus (ca 5th century BC), Democritus (460–370 BC) and Asclepiades of Bithynia (ca 2nd AD). According to this view, a thrombus could be formed by circulating fluids and/or the concentration of solid materials to create a circulatory blockage. As a term with an expanded meaning, it gradually overshadowed older terms, such as cardiolith.5,21–23 Furthermore, since the early 19th century, under the influence of Rudolph Virchow (1821–1902 AD), the term embolus was applied to the small plugs that had detached from the heart valves, while thrombus was applied to those derived from the veins.14,24–25 Consequently, the use of the term “cardiolith” faded and the names of the physicians who studied this phenomenon in the late 18th and 19th century is now forgotten. ’The term “cardiolith” faded due to nomenclature’s progression and this team of physicians who thrived from late 18th century until late 19th is now forgotten.
Conclusion
Although a series of descriptions concerning heart stones appear in medical literature since 18th century it is unclear who introduced the term “cardiolith”. The first paper mentioning it was Delépine’s work in 1890. Surprisingly the ancient Greek word “thrombus” (clot) was not used at all, and instead a more descriptive term concerning local anatomy was chosen. Since the first part of the 20th century the term has been abandoned, and “cardiolith” as a medical diagnosis is currently very rarely used (calculus cardialis). Yet mostly due to its naming, cardiolith made an impact during 19th century in cardiology.
Conflicts of interest
The authors declare no conflicts of interest.
Appendix A
Supplementary data
Supplementary data related to this article can be found at
References
Cite this article
TY - JOUR AU - Gregory Tsoucalas AU - Theodoros G. Papaioannou AU - Charalampos Vlachopoulos AU - Marianna Karamanou PY - 2018 DA - 2018/05/23 TI - Cardioliths in 19th century medical literature JO - Artery Research SP - 9 EP - 13 VL - 23 IS - C SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2018.05.005 DO - 10.1016/j.artres.2018.05.005 ID - Tsoucalas2018 ER -