
Change of bilateral difference in radial artery pulse morphology with one-side arm movement
- DOI
- 10.1016/j.artres.2017.04.008How to use a DOI?
- Keywords
- Arterial volume compliance; Artery pulse; Radial artery pulse
- Abstract
Previous studies have demonstrated that the compliance of peripheral artery changes with arm movement. This study aimed to quantify the bilateral difference in radial artery pulse morphology with one-side arm movement. Twenty-four healthy subjects were recruited. Radial artery pulses were synchronously recorded from both arms, with one arm (left or right) at five different positions (90°, 45°, 0°, −45° and −90°) and the other arm at horizontal level (0°) as reference. Two types of indices of arterial pulse morphology were derived from the normalized arterial pulse signals: the waveform width corresponding to the 50%, 60% and 70% pulse amplitude (W50, W60, W70) and the total area of normalized pulse waveform (Apulse). No matter whether the moving arm was left or right arm, when compared with the other side reference arm, all the waveform widths decreased with arm moving from 90°, 45°, 0°, −45°, and −90°. The bilateral difference of W50, W60 and W70 with the moving arm (either left or right) at 90°, 45° were significantly positive (both p < 0.01) and significantly negative at −90° (both p < 0.05). Meanwhile, no matter whether the moving arm is left or right, Apulse decreased with arm moving from 90°, 45°, 0°, −45°, and −90°. The bilateral difference of Apulse with the left moving arm were significantly positive at 45°, 90° (both p < 0.05). Meanwhile, the bilateral difference of Apulse from the moving right arm was significantly positive at 90° and significantly negative at −45° and −90° (all p < 0.05). In summary, this study quantified the bilateral arterial pulse morphology between arteries with different compliances induced by a simple arm positioning procedure.
- Copyright
- © 2017 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Arteries play an important role in cardiovascular physiology and pathophysiology. Arterial properties can change with different physiological and clinical conditions,1–4 including aging,5,6 hypertension,3 diabetes,4 heart failure1,7 drug treatment,8 smoking,9 alcohol10 and emotion states.11 It is clinically important to characterize and quantify the elastic properties of arteries. Various non-invasive techniques have been used to indirectly quantify the properties of arteries. The most commonly used technique measures pulse wave velocity (PWV) or pulse transit time (PTT).12–14 Analysis of pulse waveform shape characteristics has also been accepted as another non-invasive technique. The difference in finger pulse amplitude changes with changing pressure have been explored in patients with cardiovascular diseases.15 The carotid waveform morphology has also been used to investigate the difference between the peripheral and central arterial pressure pulses.16
Recently, Zheng and Murray12,17 reported a simple technique through arm moving to induce the change of peripheral arterial volume distensibility and concluded that the peripheral arteries are more compliant with the arm positioned above horizontal level in comparison with the arm at the horizontal level.18 To the best of our knowledge, the arterial pulse morphology change with arm moving has not been quantified. Therefore, the first aim of this study was to quantify the radial pulse morphology changes for arteries with different compliances induced by positioning the arm at different positions. For healthy subjects, the bilateral radial pulse morphology should be almost the same if both arms are positioned at the same height levels. By positioning one arm at horizontal level as reference and the other arm at a different height, a bilateral pulse morphology difference could be introduced, and its changes with arm positions could be quantified. Thus, the bilateral pulse morphology difference from the synchronously recorded bilateral radial pulses, i.e., between the moving arm (at five different positions 90°, 45°, 0°, −45°, and −90° to the horizontal level) and the reference arm (at horizontal position 0°), would be quantified.
Methods
Subjects
Twenty-four healthy subjects (14 male and 10 female) aged between 21 and 50 were enrolled in this study. Their basic clinical information is presented in Table 1. The study received ethical permission from the local Ethical Committee of Shandong University in China, and all subjects gave their written informed consent to participate in this study.
| Variables | Value | Range (min–max) |
|---|---|---|
| Number (M/F) | 24 (14/10) | – |
| Age (year) | 29 ± 8 | 21–50 |
| Height19 | 169 ± 8 | 151–183 |
| Weight (kg) | 63 ± 11 | 41–87 |
| BMI (kg/m2) | 22 ± 3 | 15–27 |
| SBP (mmHg) | 115 ± 12 | 93–137 |
| DBP (mmHg) | 70 ± 10 | 57–95 |
| MAP (mmHg) | 85 ± 10 | 69–107 |
Value is expressed as number (male/female) or mean ± standard deviation (SD). BMI: body mass index, SBP: systolic blood pressure, DBP: diastolic blood pressure, MAP: mean arterial pressure.
Basic clinical information for the 24 subjects studied.
Arterial pulse recording procedure
All the measurements were undertaken in a quiet room at Shandong University. Each subject was asked to lie down on a measurement bed for 5 min before the formal arterial pulse recording to allow cardiovascular stabilization. All the measurements were operated by the same operator.
For each subject, there were two repeat measurement sessions with an interval of 20 min. Within each measurement session, two series of five separate recordings were performed with one arm at five different positions (90°, 45°, 0°, −45°, and −90° to the horizontal level) and the other arm at horizontal position (0°) as the reference arm, and then vice versa, i.e., firstly, the right arm was regarded as the ‘moving arm’ by positioning at five positions and the left arm as the ‘reference arm’; then the left arm was regarded as the ‘moving arm’ with recordings at five positions and the right arm as the ‘reference arm’. Figure 1(A) shows the schematic diagram of the measurement procedure and a picture of the set-up. In total, 20 arterial pulse recordings were obtained from each subject (from 2 repeat session, 5 recordings with the left arm as moving arm and 5 recordings with the right arm as the moving arm).
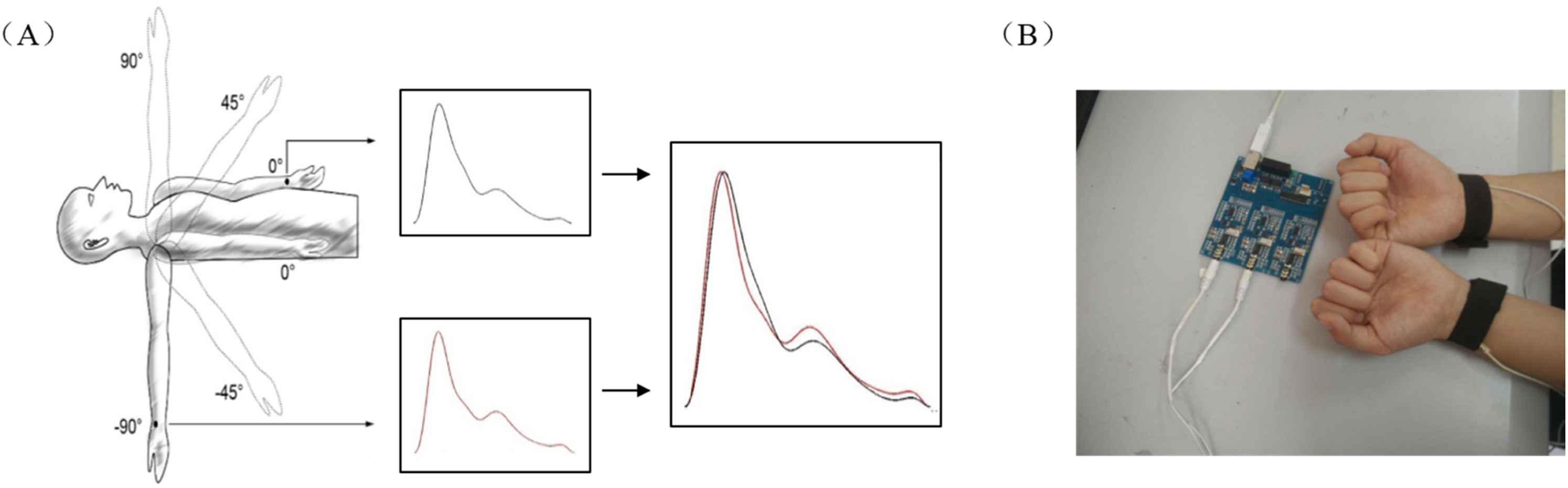
(A) The schematic diagram of the measurement procedure with the right arm (moving arm) at different positions and the left arm was regarded as ‘reference arm’. (B) the Piezoelectric sensors were placed in the radial arteries of both arms and were fixed using two same size bandages.
During each recording, all subjects remained supine position on a measurement bed. Piezoelectric sensors (manufactured by Hefei-Huake Electronic Technology Research Institute, China) were placed in the radial arteries of both arms and were fixed using two same size bandages (as shown in Fig. 1(B)). When arterial pulse signals were stalely and clearly shown on the display screen, the moving arm was positioned at the measurement height by a mechanical support to avoid the movement and the reference arm was constantly kept at horizontal position. The radial artery pulses from both two side arms were simultaneously recorded for 40 s with a sampling rate of 500 Hz.
At the beginning and end of each study, systolic and diastolic blood pressures (SBP and DBP) were measured using a clinically validated BP monitor (102, Dongyue healthcare, Shandong, China) with both arms at the horizontal level. Mean arterial pressure (MAP) was calculated used the equation: MAP = DBP + 0.4(SBP − DBP).20
Arterial pulse processing
For each recording, the feet of the recorded radial artery pulses were detected by an open-source algorithm21,22 and then manually verified. 11 consecutive stable and high quality beats were chosen by manual. Then 11 separate beats were extracted respectively between two adjacent pulse feet. In order to eliminate the effects of changes in applanation pressure, the pulse waveform is normalized. Each beat was then normalized with the length of 1000 points and amplitude of 1 (i.e., pulse foot had amplitude of 0 and pulse peak of 1). Normalized mean pulse template (NMPT) was then constructed by averaging 11 normalized pulses from each recording. Figure 2 shows the examples of five NMPTs with the left arm at 90°, 45°, 0°, −45° to −90° to the horizontal level. For each subject, a total of 40 NMPTs are obtained, with 20 NMPTs from the moving arm (left or right) at the five different positions (2 repeat sessions, 2 moving arms, 5 positions), as well as 20 NMPTs from the reference arm.
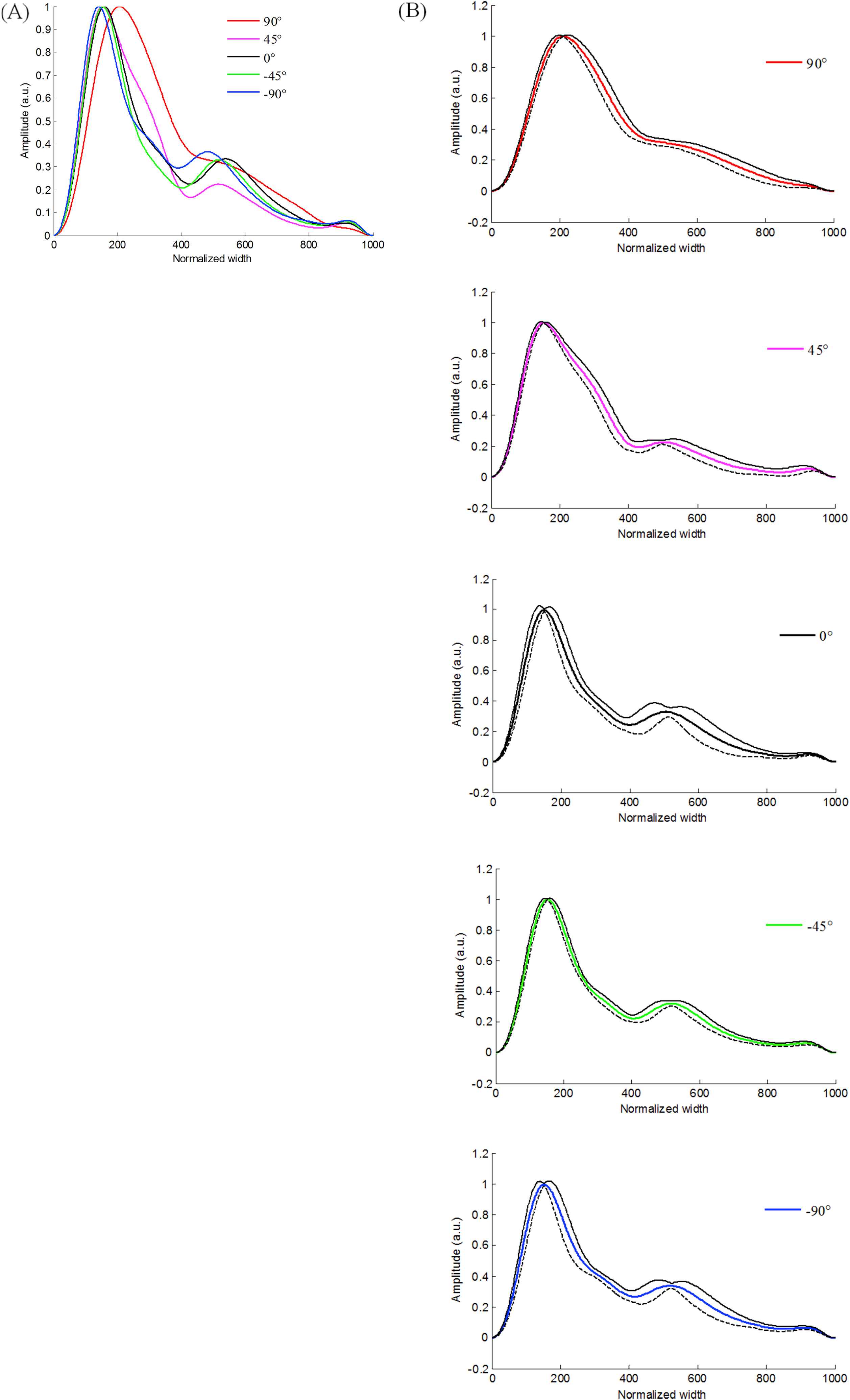
Examples of five NMPTs from one subject with the left arm at five different positions (90°, 45°, 0°, −45°, and −90° to the horizontal level). (A) show the five mean NMPTs and (B) shows the detailed three curves (average curve (thick solid line) and the mean ± 2 SDs curves (thin solid and dotted lines respectively)) for each position.
Pulse morphology indices and their bilateral differences
To quantify the pulse morphology changes with the arm at different positions, two types of indices were defined. One was the pulse waveform width index, which was defined as a pulse waveform width corresponding to a certain percentage of the pulse amplitude. In this study, three pulse waveform width indices (W50, W60 and W70) corresponding to 50%, 60% and 70% of pulse amplitude were considered. Another index was the total area of the NMPT signal (Apulse). Figure 3 demonstrates their definitions.
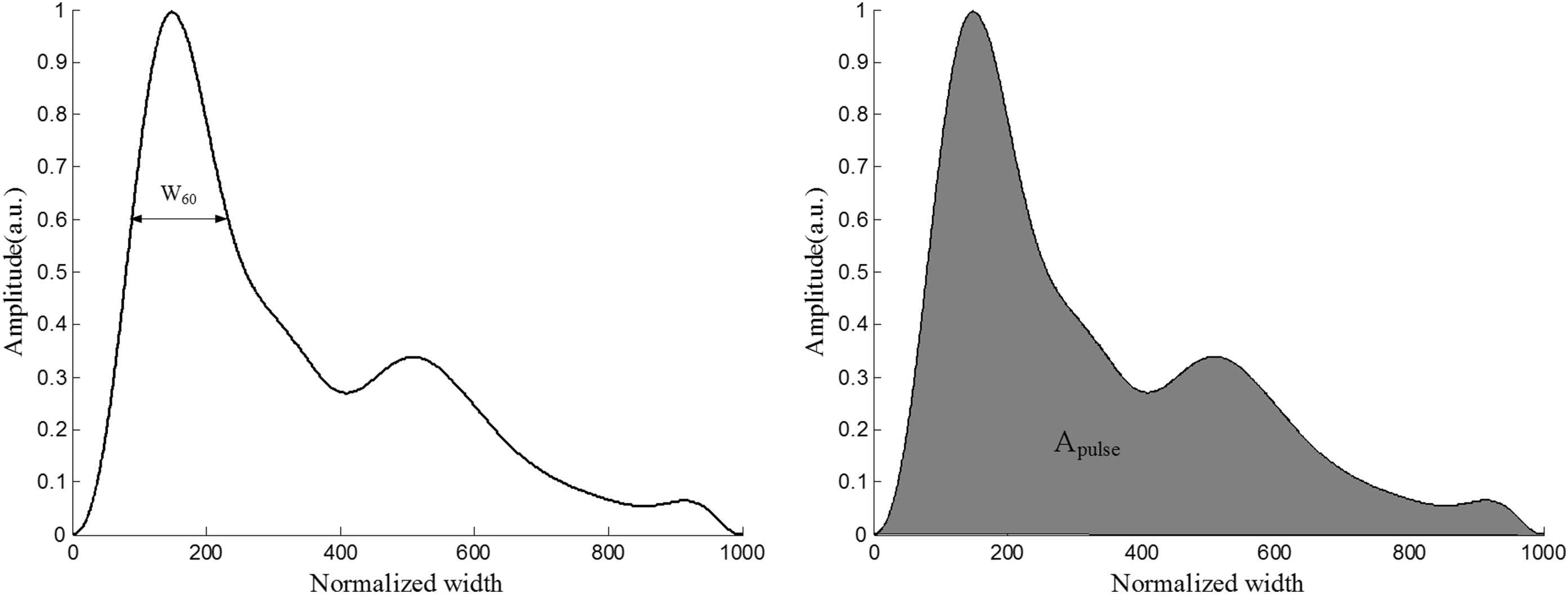
Definitions of the two indices: pulse waveform width (W60 as an example) and area of pulse waveform (Apulse).
The bilateral waveform width difference and the bilateral total area difference were then calculated between the moving arm (at five different positions 90°, 45°, 0°, −45°, and −90° to the horizontal level) and the corresponding reference arm (at horizontal position 0°) to obtain the bilateral pulse morphology differences.
Data and statistical analysis
The mean and SD values of the obtained indices (Apulse, W50–W70, and their bilateral differences) were firstly calculated, separately for each arm at different positions. The effect of arm position on the bilateral pulse morphology differences was then tested. A p < 0.05 was considered statistically significant.
Results
Changes of bilateral difference of W60 with arm moving
Our results show that the changes of W50, W60 and W70 with arm moving were similar and there was no significant difference between these three indices at different arm positions. To simplify the results, W60 was used to describe the results in details.
Figure 4(A) and (B) shows overall means and their SDs of index W60 with the moving arm (left or right) at different positions (90°, 45°, 0°, −45°, and −90°) and the other arm at horizontal level as reference. Whether left arm or right arm, W60 decreased with arm moving from 90°, 45°, 0°, −45°, and −90°. When compared with the reference arm, W60 from the moving left arm were significantly larger at 90°, 45° (both p < 0.01) and significantly smaller at 0°, −90° (both p < 0.05), while not at −45°. Meanwhile, W60 from the moving right arm were significantly larger at 90°, 45° (both p < 0.01) and significantly smaller at −90° (p < 0.05), while not at 0° and −45°. As shown in Fig. 4(C) and (D), for left arm moving, the mean bilateral W60 differences were 54.9, 34.1, 8.6, −4.2 and −9.0 respectively for the five positions, and for right arm moving, their corresponding mean differences were 53.1, 35.4, 2.1, −5.9 and −11.2 respectively.
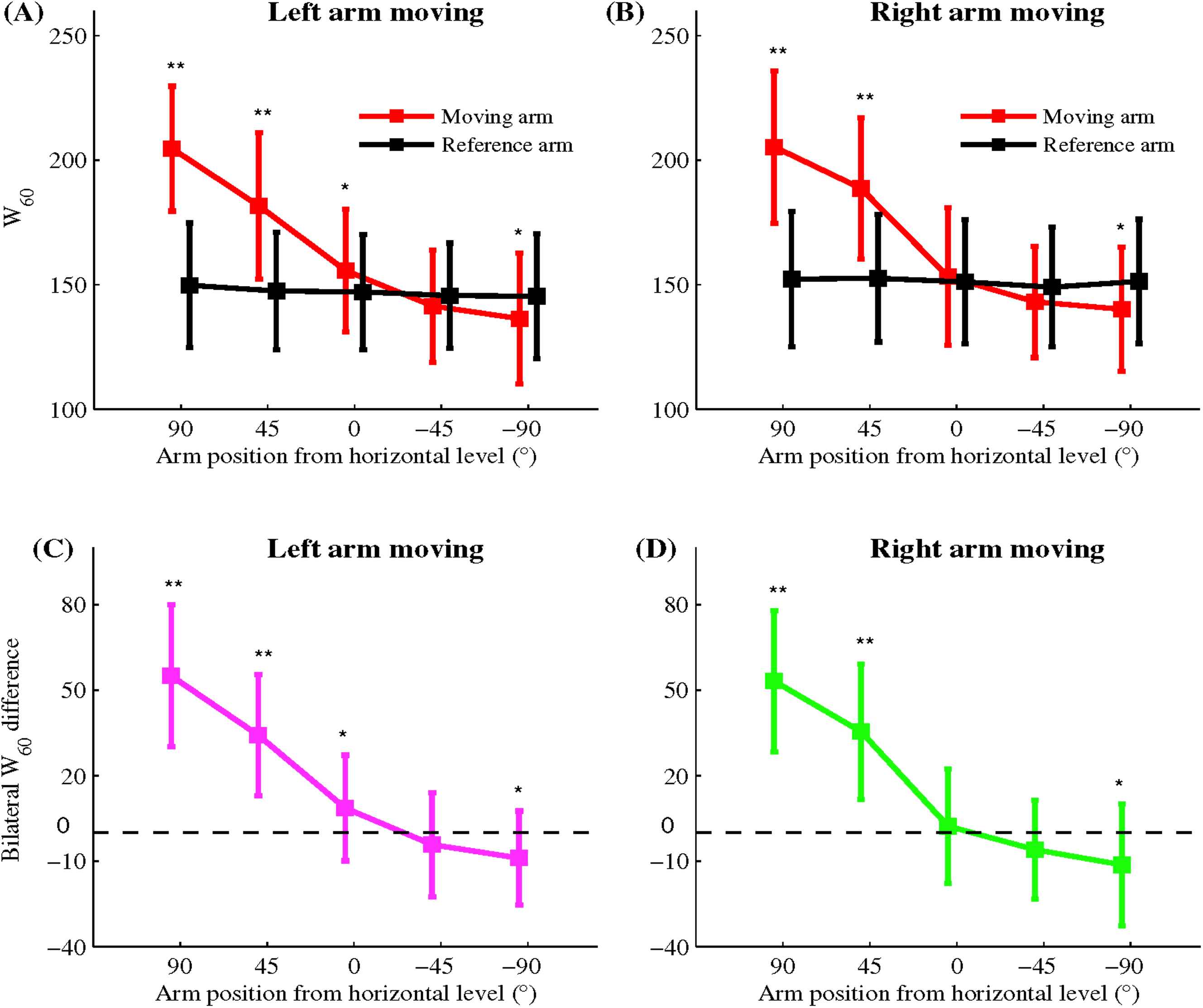
Results of index W60 with the moving arm (A and C for left arm, and B and D for right arm) at five different positions (90°, 45°, 0°, −45°, and −90° to the horizontal level) and the other side arm at horizontal level as reference: (A) and (B) show the means and standard deviations (SDs) for index W60 respectively, and (C) and (D) show the bilateral W60 difference between the moving arm and the reference arm, with the dotted zero line. * means significant statistical difference for p < 0.05 and ** means significant statistical difference for p < 0.01.
Changes of bilateral difference of Apulse with arm moving
Figure 5(A) and (B) shows overall means and their SDs of index Apulse with the moving arm (left or right) at different positions (90°, 45°, 0°, −45°, and −90°) and the other arm at horizontal level as reference. Whether left arm or right arm, Apulse decreased with arm moving from 90°, 45°, 0°, −45°, and −90°. When compared with the reference arm, Apulse from the moving left arm were significantly larger at 90° (p < 0.01) and 45° (p < 0.05), while not at 0°, −45° and −90°. Meanwhile, Apulse from the moving right arm was significantly larger at 90°, and significantly smaller −45° and −90° (both p < 0.05), while not at 45° and 0°. As shown in Fig. 5(C) and (D), for left arm moving, the mean bilateral Apulse differences were 30.3, 11.1, 6.3, −8.1 and −7.0 respectively for the five positions, and for right arm moving, the corresponding mean differences were 19, 4, −4, −14 and −13 respectively.
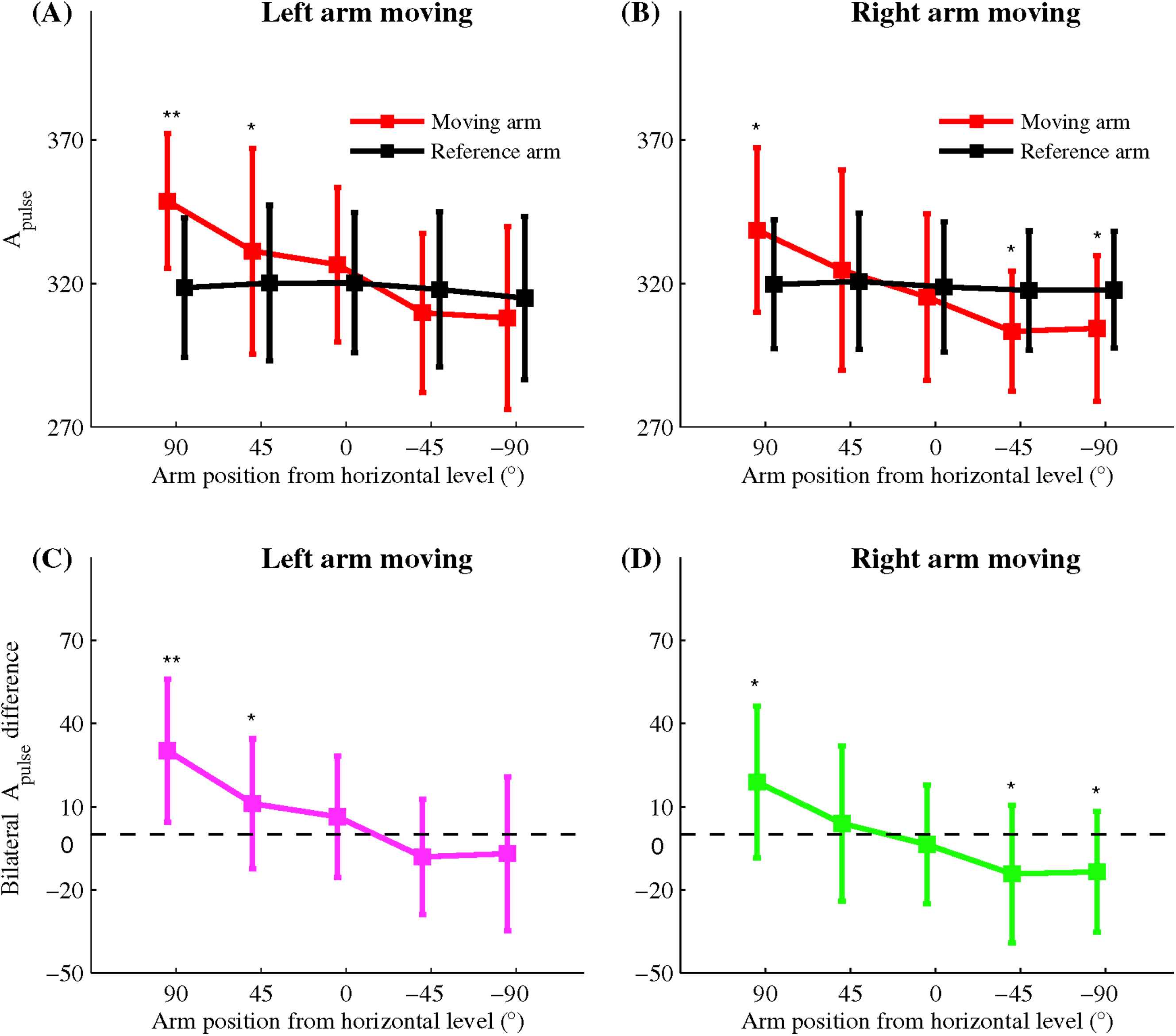
Results of index Apulse with the moving arm (A and C for left arm, and B and D for right arm) at five different positions (90°, 45°, 0°, −45°, and −90° to the horizontal level) and the other side arm at horizontal level as reference: (A) and (B) show the means and standard deviations (SDs) for index Apulse respectively, and (C) and (D) show the bilateral Apulse difference between the moving arm and the reference arm, with the dotted zero line. * means significant statistical difference for p < 0.05 and ** means significant statistical difference for p < 0.01.
Discussion
This study quantified the bilateral radial artery pulse shape difference between the moving arm (at five different positions 90°, 45°, 0°, −45°, and −90° to the horizontal level) and the reference arm (at horizontal position 0°). These changes were quantified by two indices (pulse waveform width and normalized pulse area). Specifically, bilateral W40, W50, W60 and Apulse difference were quantified, which decreased gradually and significantly with the arm moving from 90° to 45°, 0°, −45°, and −90° respectively.
The effect of arm position on heart rate has been counted in this paper. The means and SDs of heart rate with arm moving from 90°, 45°, 0°, −45°, and −90° were 66.6 ± 5.1, 66.9 ± 5.5, 66.8 ± 5.2, 66.9 ± 5.2 and 67.1 ± 5.0 beat/min respectively. Our results were consistent with results of previous research that the subject’s heart rate did not change if the subject kept quiet, whether supine or sitting, with the arm passively positioned in different positions by a support, in a way that the arm kept relaxed without muscle tension.23,24
The changes of elastic properties of arteries are associated with different physiological and clinical conditions induced by the change of BP. Previous studies have found important differences between indirect BP readings when the arm was placed in different positions.23,25,26 Both SBP and DBP values were significantly decrease when the arm were elevated above the level of the right atrium, while significantly increase when lowered below the level of the right atrium. Previous studies also studied the influence of body posture on the indirectly measured BP values when the arm was placed at the right atrium level and showed that both SBP and DBP were significantly higher in the supine than those in the sitting position.27 In our current study, all subjects were asked to keep a supine position and both arms were constantly kept at heart level at 0° measurement.
With elevating the arm, the effect of gravity induces a hydrostatic pressure difference. Mitchell et al.28 and Netea et al.26 reported that the change of BP values taken from the arm at different levels versus the reference level of the right atrium could almost completely be explained by the effect of hydrostatic forces. The change of BP affects the arterial compliance. Pucci et al. researched the relationship between the arterial compliance and BP with the arm movement, and reported that, relative to the heart level, radial augmentation index increased with the arm elevating and decreased with the arm reducing.23
Zheng and Murray18 reported that the peripheral arteries compliant with the arm positioned above horizontal level in comparison with the arm positioned below horizontal level by measuring PTT difference. However, this conclusion was from the unilateral finger/ear PPG measurements, not from the simultaneously recorded bilateral radial artery measurements as in this study. Different from the published study by Zheng et al., two pulse waveform morphology indices, i.e., W60 and Apulse, were used in the current study, and the effect of arm position on arterial pulse waveform was investigated from simultaneously recorded bilateral radial pulse waveforms, avoiding the potential physiological variations with time.
Previous studies assessed the change of elastic properties by measuring PWV, but produced different clinical conclusions, with no change,29 higher19,30 and lower31 of PWV results. These conflicting results may be partly due to the different segments of arteries used for investigation or/and the methodological difference. Further investigation on pulse morphology is therefore worthwhile.
If the peripheral arterial system had relatively higher compliance, a larger proportion of the ejected blood would expand the peripheral arteries and hence the radial artery pulse would be expected to have bigger pulse’s area and width of pulse waveform.5 In the current study, it has been observed both pulse waveform’s width and area indices increased with arm raising, where the arteries are more compliant. Therefore, our results agreed with the published expectation and demonstrated that the change of pulse waveform’s width and area indices could be used to quantify the change of arterial compliance with a simple arm positioning procedure.
As the comparison of the two indices W60 and Apulse, it is observed that W60 was better than Apulse in response to arterial compliance changes since the effect of arm position on W60 was larger as shown in Figs. 4 and 5. In addition, from Figs. 4 and 5, slight difference was observed between the left and right arms at 0° level. This result may be partly due to the physiological structure difference of the left and right arms.
In conclusion, this study quantified the bilateral difference of the two pulse morphology indices, i.e., W60 and Apulse, with the arm at different positions, which indicated that these indices could be potentially used for quantifying arterial compliance changes.
Conflict of interest statement
The authors declare no conflict of interest.
Acknowledgments
This research was sponsored by the
References
Cite this article
TY - JOUR AU - Xinge Jiang AU - Shoushui Wei AU - Dingchang Zheng AU - Feifei Liu AU - Shouqin Zhang AU - Zhimin Zhang AU - Chengyu Liu PY - 2017 DA - 2017/05/12 TI - Change of bilateral difference in radial artery pulse morphology with one-side arm movement JO - Artery Research SP - 1 EP - 8 VL - 19 IS - C SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2017.04.008 DO - 10.1016/j.artres.2017.04.008 ID - Jiang2017 ER -