
The effects of antihypertensive drugs on arterial stiffness☆
This article was presented as lecture in the symposium on “Arterial stiffness: a translational approach” at the ARTERY 14 Congress in Maastricht, The Netherlands (October 9–11, 2014).
- DOI
- 10.1016/j.artres.2016.02.001How to use a DOI?
- Keywords
- Pulse wave velocity; Arterial stiffness; Augmentation index; Target organ damage; Hypertension guidelines; Angiotensin-converting enzyme inhibitor; Calcium channel blocker
- Abstract
Ageing and cardiovascular risk factors, particularly uncontrolled hypertension, adversely impact arterial stiffness and wave reflection leading to increased central systolic blood pressure. Carotid-femoral pulse wave velocity is the “gold standard” method for the assessment of aortic stiffness. Increased pulse wave velocity has been independently associated with adverse cardiovascular outcomes. Thus, current European hypertension guidelines acknowledge the reproducibility, predictive value, and cost-effectiveness of pulse wave velocity.
Augmentation index, a marker of arterial stiffness and wave reflection has been also associated with poor cardiovascular outcome.
Current evidence suggests that increased arterial stiffness and wave reflection contribute to target organ damage. Thus, early intervention is fundamental for cardiovascular prevention. Elevated pulse wave velocity and augmentation index can be reduced by normalizing blood pressure and by using specific treatments for reducing arterial stiffness.
This article will review the available evidence on the effect of the different antihypertensive drug classes on arterial stiffness. Angiotensin-converting enzyme inhibitors, angiotensin receptor blockers can reduce pulse wave velocity beyond the blood pressure lowering effect. Although blood pressure normalization is the most effective therapeutic tool for reducing parameters of wave reflections, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers and calcium channel blockers have beneficial effects on augmentation index.
- Copyright
- © 2016 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Ageing and cardiovascular (CV) risk factors, particularly hypertension, cause functional and structural alterations in the macro- and microcirculation, representing common pathologic mechanism for target organ damage and CV events.1–3
Arterial stiffness of the large arteries and increased media/lumen ratio or capillary rarefaction in the microcirculation can occur prematurely in susceptible patients as those with hypertension, characterizing the so called early vascular ageing2,3
Aortic stiffness is responsible for most of the pathophysiologic effects of central blood pressure (BP) and arterial stiffness on the left ventricle, brain, and kidney.1–3 The assessment of carotid to femoral pulse wave velocity (PWV) is considered the “ gold standard” for measurement of aortic stiffness, since it is a simple, non-invasive and reproducible method.1 Furthermore, PWV has a large amount of clinical evidence for the predictive value of aortic stiffness for CV events.4,5 Therefore, it has been included among the established measures of hypertensive target organ damage by previous and current European guidelines.6,7
Functional and structural changes in the microcirculation cause altered wave reflection, which contributes to the increase in central BP associated to arterial stiffness. An index of arterial stiffness and wave reflection, such as central BP augmentation, has been also shown to have independent prognostic relevance.8,9
According to their pathophysiological role, arterial stiffness and wave reflections have become a therapeutic target in patients with elevated CV risk. The normalization of elevated BP is one of the key approaches for reducing elevated PWV and wave reflections.1–3 The earlier intervention takes place, the better, as arterial wall damage can never be fully reversed and pharmacological intervention helps normalize the increased rate at which arterial wall damage occurs.2,3
The aim of this article is to review how different antihypertensive drug classes may reduce arterial stiffness.
Strategies for reducing PWV
BP normalisation
Increases in distending BP caused by hypertension lead to changes in the composition (elastin/collagen ratio) and structure of arteries (e.g. increased arterial wall thickness and smooth muscle hypertrophy) that accelerate arterial stiffening.4
In the short term, arterial stiffness can be reduced without modifying properties of the arterial wall by BP reduction per se, which shifts wall stress to the elastin component, while with arterial stiffening, the haemodynamic load in arteries increases leading to impairment of the natural repair process and damage of the macro- and the microcirculation.1–3
Thus, early pharmacological intervention can make a substantial difference in limiting endothelial and arterial wall damage and long-term treatment with antihypertensive medication may reduce arterial stiffness further via the complementary mechanism of arterial remodelling2,3 (Fig. 1).
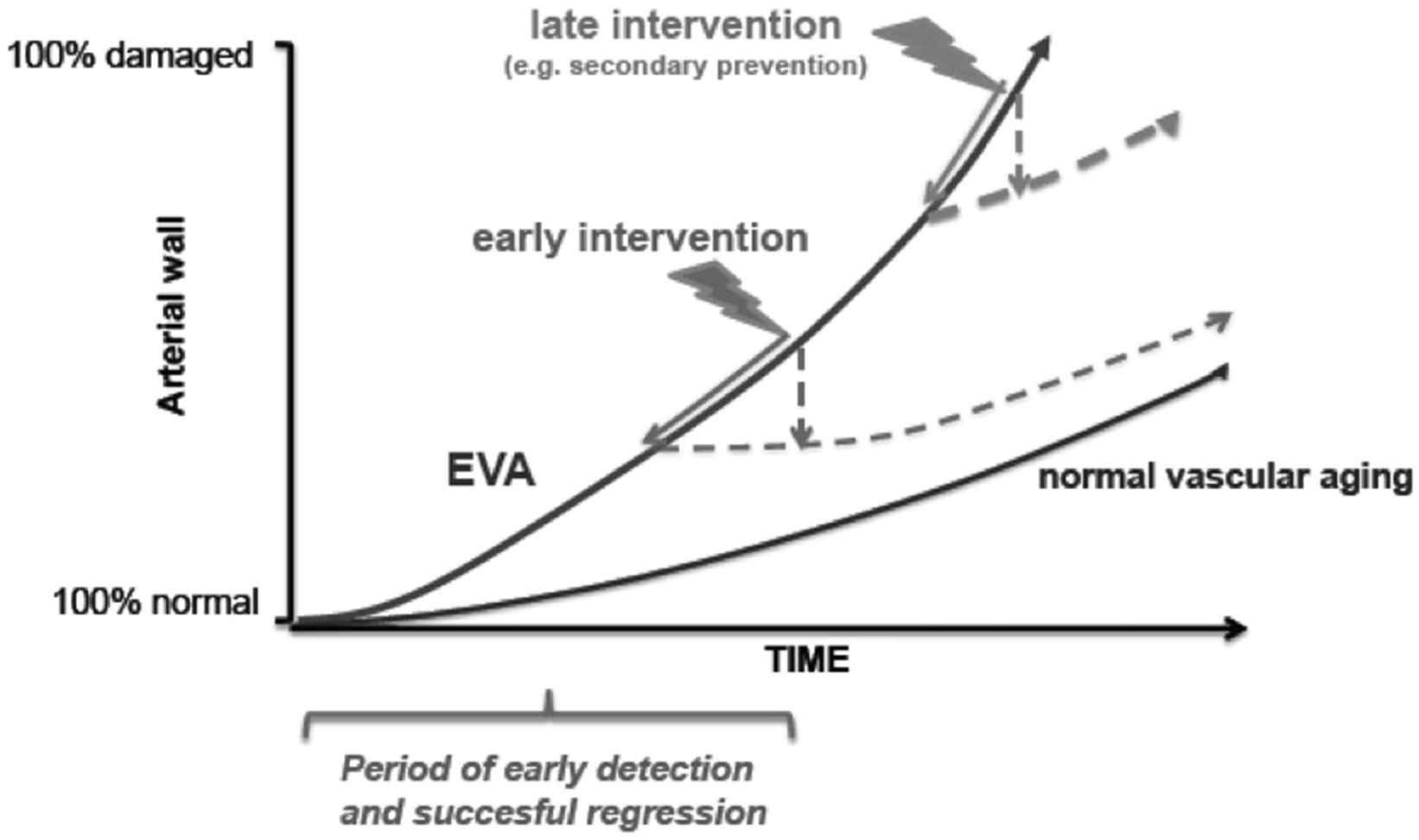
The effect of early and late intervention on preventing arterial wall damage in early vascular ageing (EVA). Modified from Ref [2].
In a 5.3-year study of PWV in routine clinical practice in 97 patients with essential hypertension (63 ± 11 years), long-term treatment with antihypertensive therapy decreased aortic PWV by 3.17 m/s (p < 0.0001) from 14.2 ± 4.2 m/s at baseline.10 Nearly two thirds (65%) had BP < 140/90 mm Hg. The rate of change of PWV was −0.64 ± 0.06 m/s per year after adjustment for age, sex, heart rate and mean BP. The reduction in PWV was found to account for most of the decrease in central pulse pressure from 59 ± 22 mm Hg to 54 ± 14 mm Hg (p < 0.001). Brachial systolic BP also decreased by −0.9 ± 0.3 mm Hg per year (p < 0.05), but not enough to explain the reduction in PWV. Indeed the decrease in PWV was only slightly modified (rate of change of from −0.70 to −0.64 m/s per year) when adjusted for the reduction of mean BP in the multivariate analysis.
These findings suggest that mechanisms other than BP lowering also play a role in the beneficial effect of antihypertensive treatment on aortic stiffness.
Antihypertensive drugs and PWV
Although BP reduction per se is useful for reducing PWV, different classes of antihypertensive drugs have particular properties, making them more or less suited for reducing arterial stiffness.11–13
The inhibition of the renin-angiotensin system (RAS) reduces peripheral resistances and mean BP, leading to a passive reduction of arterial stiffness. Furthermore, RAS inhibitors can inhibit numerous deleterious effects caused by the binding of angiotensin II to AT1 receptors, including vasoconstriction and endothelial dysfunction, which increase oxidative stress, vascular remodelling and fibrosis14,15 (Fig. 2).
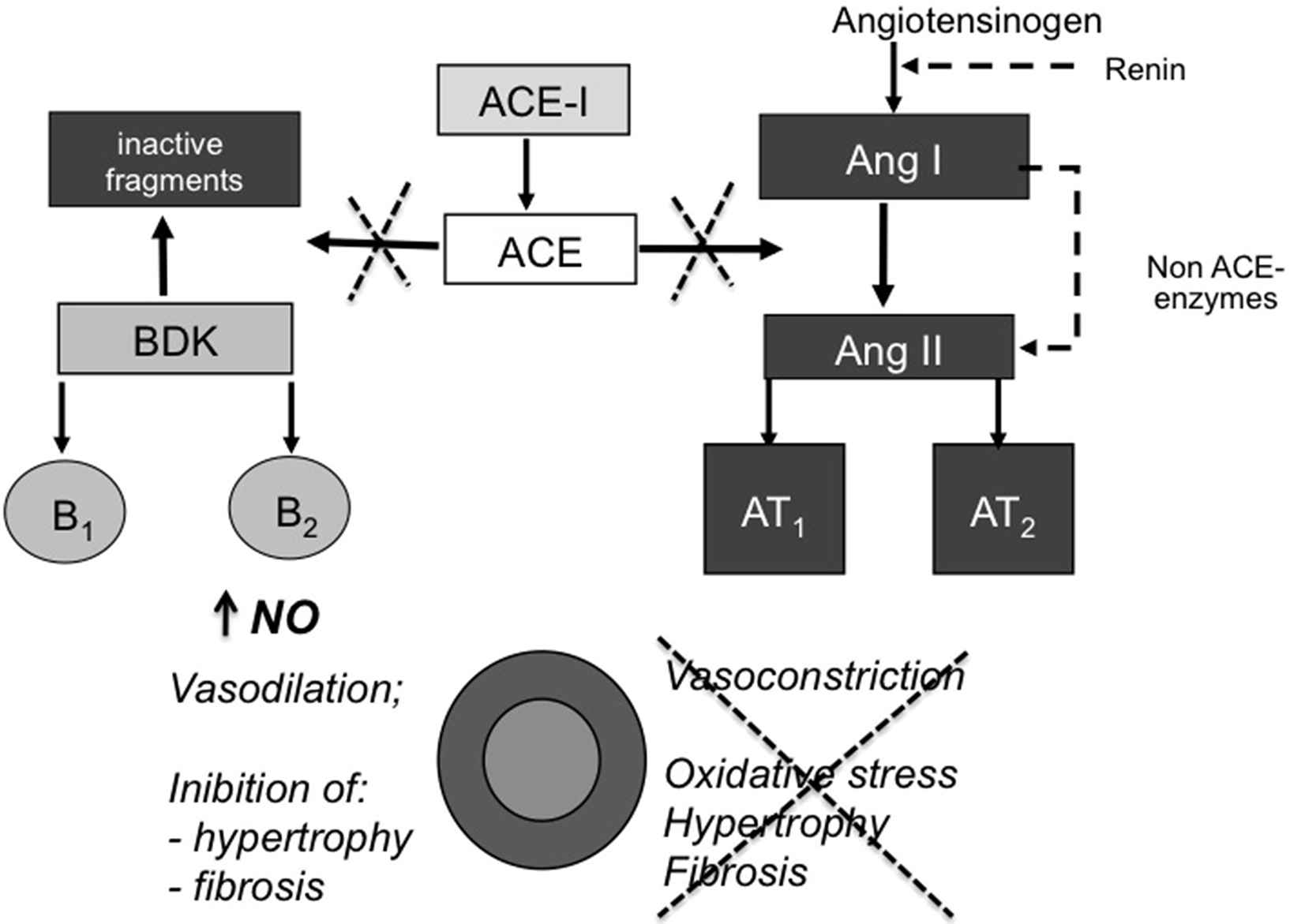
Protective effects of ACE inhibition on vascular function and structure. Abbreviations: ACE, angiotensin-converting enzyme; ACE-I: ACE-inhibitors; NO, nitric oxide.
RAS inhibition can decrease arterial stiffness also reducing the expression and activity of matrix metallo-proteinases, which damage collagen and elastin.1,15
Angiotensin converting enzyme inhibitors (ACEIs) also prevent the degradation of bradykinin increasing the production of nitric oxide, prostacyclin and endothelium-derived hyperpolarising factor, which leads to beneficial effects such as vasodilation, decreased proliferation of vascular smooth muscle cells, reduced platelet adhesion and restore fibrinolytic balance (Fig. 3).16 Clinical studies showed that ACEIs, but also Angiotensin II Receptors Blockers (ARBs), can improve endothelial function16 and reduce vascular remodelling.17 The effect of antihypertensive drugs on conduit endothelial function was tested in 168 hypertensive patients after 6-month with nifedipine GITS, amlodipine, atenolol, nebivolol, telmisartan and perindopril.18 The ACEI only restored flow-mediated dilation of the brachial artery.
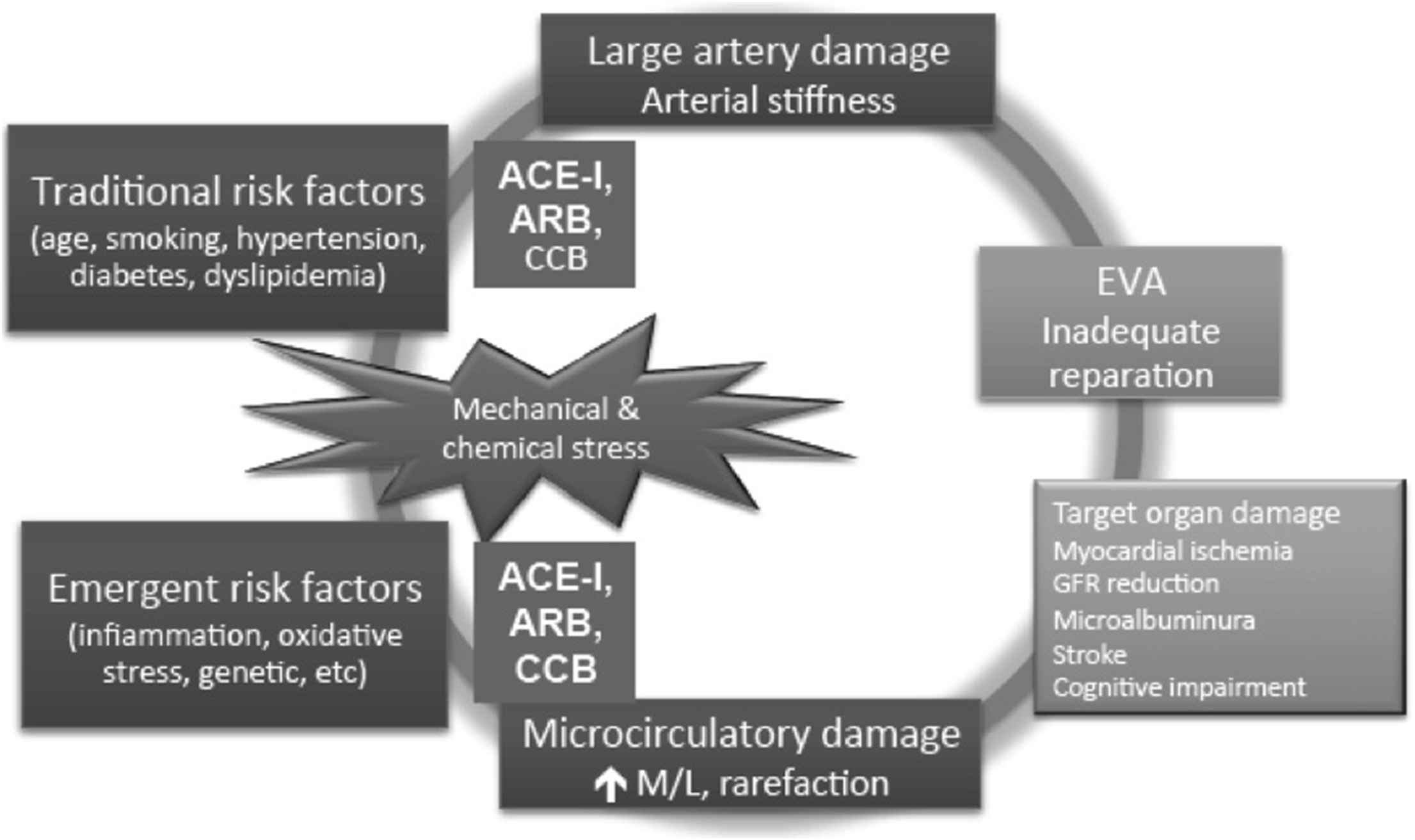
Effect of antihypertensive medication on the vicious circle of arterial damage. Modified from Ref. [3]: Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blockers; CCB, calcium channel blocker; GFR, glomerular filtration rate.
The effect of different anti-hypertensive drug classes was specifically evaluated in a meta-analysis of individual data from 15 randomized, controlled, double-blind, parallel group trials evaluating the changes of PWV after treatment in 294 patients with untreated mild-to-moderate hypertensive patient from a single centre.19 This study showed that in the short-term and long-term trials, PWV decreased significantly by −0.75 and −1.3 m/s in the active treatment group compared with by −0.17 and −0.44 m/s in the placebo group, respectively.19 Active treatment was independently related to the changes in PWV explaining 5 and 4% of the variance in the short-term and long-term trials, respectively. In the short-term trials, ACEIs were more effective than calcium channel blockers (CCBs) and placebo on improving arterial stiffness, while in the long-term trials, ACEI, CCBs, beta-blockers, and diuretics reduced significantly PWV compared to placebo.
In a subsequent meta-analysis that compared the effect of treatment with ACEIs on arterial stiffness versus placebo in 5 trials including 469 patients, ACE inhibition reduced PWV (pooled mean change difference −1.69 m/s; 95% CI, −2.05 to −1.33 m/s; p < 0.00001) with insignificant heterogeneity.20 Compared with other antihypertensive therapies (9 trials including 378 patients), however, the pooled mean change difference in PWV of −0.19 m/s (95% CI, −0.59–0.21 m/s; p = 0.36; I2 = 0%) was non-significant. Interestingly, mean BP differences between baseline and end of treatment did not predict the ACEIs induced changes in PWV.
The effect of ACEIs on arterial stiffness is not only BP-independent but also it seems to be dose-dependent, as demonstrated by the effect of perindopril on carotid distensibility in hypertensive patients with diabetes mellitus.21
As already mentioned, CCBs reduce PWV significantly as compared to placebo,20 an effect which can be ascribed to BP reduction but also to the prevention smooth muscle cell contraction by blocking receptor- or voltage-operated channels.
Diuretics have a beneficial effect on PWV by reducing BP.11–13,20 However, a specific mechanism, related to the anti-fibrotic effect, is ascribed to the aldosterone antagonist, as suggested by results of a clinical trial, in which spironolactone added to RAAS inhibition in 56 patients with early chronic kidney disease resulted in an additional reduction in PWV (−0.8 ± 1.0 versus −0.1 ± 0.9 m/s) and in aortic distensibility (0.69 ± 0.86 × 10−3 versus 0.04 ± 1.04 × 10−3 mm Hg) compared with placebo (both p < 0.01).22 Indapamide reduced PWV when combined to the ACEI perindopril as compared to the beta-blocker atelolol.23
Beta-blockers can reduce PWV, although some that their effect, in particular for those that are non-vasodilating is either limited or negative.10–13,23
Reduction of PWV has been a target for specific therapeutic treatments, such the cross-linking breaker ALT-711, which significantly reduced PWV in elderly subjects with increased pulse pressure (>60 mmHg),24 but which are not yet available for clinical use.
Antihypertensive drugs and augmentation index
The augmentation index, a marker of the wave reflection, is reduced by most of the antihypertensive drugs’ classes, an effect which is mainly related to mean BP reduction.10–13
However, the meta-analysis of Shahin et al.13 showed that wave reflection, measured by augmentation index, was reduced significantly with ACE inhibitors compared with other anti-hypertensive drugs (7 trials including 323 patients; pooled mean change difference −1.84 m/s; 95% CI, −3.00 to −0.68 m/s: p = 0.002; I2 = 32%; p for heterogeneity = 0.11) as well as when compared with placebo (7 trials including 614 patients; pooled mean change difference −3.79 m/s; 95% CI, −5.96 to −1.63 m/s; p = 0.0006; I2 = 87%; p for heterogeneity <0.00001).
CCBs, in particular amlodipine, have been evaluated in studies with the ACEI perindopril in a large clinical trial, such as in the CAFE study,25 showing a significant reduction in central augmentation index, which might be responsible for the better cardiovascular prognosis as compared to beta-blocker and thiazide diuretic. The long-term beneficial effect on wave reflection might be ascribed to the reversing structural abnormalities in the small arteries by both perindopril and amlodipine.17
Some beta-blockers, like atenolol, are unable to modulate wave reflection via a reduction in the wall/lumen ratio of muscular arteries and arterioles17 and-or for the negative influence of bradycardia.1
Concerning diuretics, positive effects on wave reflection were reported for indapamide25; however, they were obtained with combination therapy (perindopril) and in comparison with atenolol.
Finally, nitrates can acutely reduce central augmentation and pulse pressure via a reduction in wave reflection.26 However, by dilating arteries in systemic vascular tissue, they expose this tissue to damage similar to that occurring in the brain and kidneys with ageing,27 and long-term effect are not yet provided.
Treatment of other risk factors
Since many CV risk factors other than hypertension, are associated with increased arterial stiffness and/or wave reflections, including smoking, hypercholesterolemia, obesity, metabolic syndrome, and diabetes, the optimal control of CV risk factors would help reduce arterial stiffness and PWV.28
Conclusions
Arterial stiffness is an important new therapeutic target in patients with elevated CV risk (Fig. 3). Among anti-hypertensive agents, ACE inhibitors show positive effect on PWV beyond BP reduction. Similar results have been postulated for ARB, and to lesser extent for CCBs. Less evidence support specific beneficial effect for reducing PWV of thiazide diuretics and beta-blockers. RAS inhibition and treatment with CCBs has been related to beneficial effect on wave reflection, despite most of the data is available for combination treatment.
However, only solid evidence from future studies targeted to arterial stiffness treatment and CV prognosis,29 will support the choice of a specific antihypertensive treatment based on the beneficial effect on arterial stiffness to reduce BP and CV risk.
Conflicts of interest
Prof. Ghiadoni received grants for speaker bureau from Servier and IFB Stroder.
References
Cite this article
TY - JOUR AU - Lorenzo Ghiadoni PY - 2016 DA - 2016/02/19 TI - The effects of antihypertensive drugs on arterial stiffness☆ JO - Artery Research SP - 1 EP - 5 VL - 14 IS - C SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2016.02.001 DO - 10.1016/j.artres.2016.02.001 ID - Ghiadoni2016 ER -