
Abridged version of the expert consensus document on arterial stiffness☆
The full text of this article was originally published in Eur. Heart j. 27(21) November 2006, pp 2588–2605 and this abridged version is published by kind permission of the European Society of Cardiology.
- DOI
- 10.1016/j.artres.2007.03.003How to use a DOI?
- Keywords
- Artery; Arterial stiffness; Hemodynamics; Pathophysiology; Prognosis; Cardiovascular events
- Abstract
In recent years great emphasis has been placed on the role of arterial stiffness in the development of cardiovascular diseases. The present article is an abridged version of an expert consensus document reporting the proceedings of several meetings of the European Network for Non Invasive Investigation of Large Arteries, and providing an updated and practical overview of the most relevant methodological aspects and clinical applications in this area. It provides recommendations for the determination of regional, local and systemic of arterial stiffness, and for the noninvasive determination of wave reflections. Clinical applications of arterial stiffness are also discussed.
- Copyright
- © 2007 Published by Elsevier B.V. on behalf of Association for Research into Arterial Structure and Physiology.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
In recent years great emphasis has been placed on the role of arterial stiffness in the development of cardiovascular (CV) diseases. The present article is an abridged version of an expert consensus document1 reporting the proceedings of several meetings of the European Network for Non Invasive Investigation of Large Arteries, and providing an updated and practical overview of the most relevant methodological aspects and clinical applications in this area. References have been mostly limited to longitudinal studies showing the predictive value of arterial stiffness and wave reflection for CV events. Extensive references (n = 169) are available in the full version of the expert consensus document.1
Non-invasive determination of arterial stiffness
In contrast to systemic arterial stiffness, which can only be estimated from models of the circulation, regional and local arterial stiffness can be measured directly, and non-invasively, at various sites along the arterial tree. A major advantage of the regional and local evaluations of arterial stiffness is that they are based on direct measurements of parameters strongly linked to wall stiffness.2 Tables 1–3 give the main features of various methods, the recommendations for standardization of subject conditions, and indices of regional stiffness.
| Device | Methods | Measurement site | |
|---|---|---|---|
| Regional stiffness | Complior® | Mechanotransducer | Aortic PWVa |
| Sphygmocor® | Tonometer | Aortic PWVa | |
| WallTrack® | Doppler probes | Aortic PWVa | |
| Artlab® | Doppler probes | Aortic PWVa | |
| Ultrasound systems | Doppler probes | Aortic PWVa | |
| Local stiffness | WallTrack® | Echotracking | CCAb, CFA, BA |
| NIUS® | Echotracking | RA | |
| Artlab® | Echotracking | CCAb, CFA, BA | |
| Various vascular ultrasound syst. | Echotracking | CCAb, CFA, BA | |
| MRI device | Cine-MRI | Ao. | |
| Systemic stiffness (waveform shape analysis) | Area method | Diastolic decay | |
| HDI PW CR-2000® | Modif. Windkessel | ||
| SV/PP | Stroke volume and pulse pressure | ||
| Wave reflections | Sphygmocor® | Augmentation index | All superficial arteries |
| Pulse trace® | Finger photoplethysmography |
PWV = pulse wave velocity.
Aorta = carotid–femoral, also carotid–radial and femoro-tibial PWV.
All superficial arteries, including particularly those mentioned: Ao. = aorta; CCA = common carotid artery; CFA = common femoral artery; BA = brachial artery; RA = radial artery; and SV/PP = stroke volume/pulse pressure.
Device and methods used for determining regional, local, and systemic arterial stiffness, and wave reflections (adapted from Ref. 1)
| Confounding factor | In practice |
|---|---|
| Room temperature | Controlled environment kept at 22 ± 1 °C |
| Rest | At least 10 min in recumbent position |
| Time of the day | Similar time of the day for repeated measurements |
| Smoking, eating | Subjects have to refrain, for at least 3 h before measurements, particularly from drinking beverages containing caffeine |
| Alcohol | Refrain from drinking alcohol 10 h before measurements |
| Speaking, sleeping | Subjects may neither speak nor sleep during measurements |
| Position | Supine position is preferred. Position (supine, sitting) should be mentioned |
| White coat effect | Influence on blood pressure and pressure-dependent stiffness |
| Cardiac arrhythmia | Be aware of possible disturbance |
Recommendations for standardization of subject conditions (adapted from Ref. 1)
| Term | Definition (units) |
|---|---|
| Stroke change in diameter | Change in diameter during systole = systolic diameter (Ds) − diastolic diameter (Dd), mm |
| Stroke change in lumen area | Change in lumen area during systole,
|
| Wall cross-sectional area | Surface of a cross-section of the arterial wall,
|
| Elastic properties of the artery as a whole | |
| Cross-sectional distensibility coefficient (DC) | Relative change in lumen area during systole for a given pressure change DC = ΔA/AΔP (kPa−1), with ΔP = local pulse pressure |
| Cross-sectional compliance coefficient (DC) | Absolute change in lumen area during systole for a given pressure change CC = ΔA/ΔP (m2 kPa−1), with ΔP = local pulse pressure |
| Peterson elastic modulus | Inverse of distensibility coefficient: the pressure change driving an increase in relative lumen area Peterson = AΔP/ΔA (kPa) |
| Elastic properties of the arterial wall material | |
| Young’s elastic modulus or incremental elastic modulus | Einc = [3(1 + A/WCSA)]/DC, kPa |
Indices of arterial stiffness applied to geometrical measurements of large arteries with ultrasounds (adapted from Ref. 17)
Regional measurements of arterial stiffness
The aorta is a major vessel of interest when determining regional arterial stiffness for at least two reasons: the thoracic and abdominal aorta makes the largest contribution to the arterial buffering function, and aortic PWV is an independent predictor of outcome in a variety of populations.3–13 However, all arterial sites have potential interest. Indeed, the forearm circulation is where blood pressure is commonly measured, and the lower limb arteries, are specifically altered by atherosclerosis. Measurement of local carotid stiffness may also provide important prognostic information, since the carotid artery is a frequent site of atheroma formation.
Pulse wave velocity measurements
The measurement of pulse wave velocity (PWV) is generally accepted as the most simple, non-invasive, robust, and reproducible method with which to determine arterial stiffness. Carotid–femoral PWV is a direct measurement, and it corresponds to the widely accepted propagative model of the arterial system. Measured along the aortic and aorto-iliac pathway, it is the most clinically relevant, since the aorta and its first branches are what the left ventricle “sees”, and are thus responsible for most of the pathophysiological effects of arterial stiffness. Carotid–femoral PWV has been used in epidemiological studies demonstrating the predictive value of aortic stiffness for CV events (Table 4). By contrast, PWV measured outside the aortic track, at the upper (brachial PWV) or lower limb (femoro-tibial PWV), has no predictive value in patients with end-stage renal disease (ESRD).14
| Measurement site | First author (year, country) | Events | Follow-up (years) | Type of patient (number) | Mean age at entry (years) | Ref. |
|---|---|---|---|---|---|---|
| Aortic PWV | Blacher (1999, Fr) | CV mortality | 6.0 | ESRD (241) | 51 | 3 |
| Laurent (2001, Fr) | CV mortality | 9.3 | Hypertension (1980) | 50 | 4 | |
| Meaume (2001, Fr) | CV mortality | 2.5 | Elderly (>70) (141) | 87 | 5 | |
| Shoji (2001, Jp) | CV mortality | 5.2 | ESRD (265) | 55 | 6 | |
| Boutouyrie (2002, Fr) | CHD events | 5.7 | Hypertension (1045) | 51 | 7 | |
| Cruickshank (2002, GB) | All cause mortality | 10.7 | IGT (571) | 51 | 8 | |
| Laurent (2003, Fr) | Fatal strokes | 7.9 | Hypertension (1715) | 51 | 9 | |
| Sutton-Tyrrell (2005, USA) | CV mortality and events | 4.6 | Elderly (2488) | 74 | 10 | |
| Shokawa (2005, Jp) | CV mortality | 10 | General pop. (492) | 64 | 11 | |
| Hansen (2006, Dk) | CV mortality | 9.4 | General pop. (1678) | 55 | 12 | |
| Mattace-Raso (2006, Neth.) | CV mortality, CHD | 4.1 | Elderly (2835) | 72 | 13 | |
| Carotid stiffness | Blacher (1998, Fr) | All cause mortality | 2.1 | ESRD (79) | 58 | 19 |
| Barenbrock (2001, Ge) | CV events | 7.9 | ESRD (68) | 43 | 20 |
ESRD: end-stage renal disease; IGT: impaired glucose tolerance; CHD: coronary heart disease and pop.: population.
Countries: Dk: Denmark; Fr: France; GB: Great Britain; Ge: Germany; Gr: Greece; Jp: Japan; and Ne: Netherlands.
Longitudinal studies reporting the independent predictive value of arterial stiffness, according to the site of measurement (adapted from Ref. 1)
Position statement: pulse wave velocity
Carotid–femoral PWV is considered as the “gold-standard” measurement of arterial stiffness.
PWV is usually measured using the “foot-to-foot” velocity method from various waveforms. The “foot” of the wave is defined at the end of diastole, when the steep rise of the wavefront begins. The transit time is the time of travel of the “foot” of the wave over a known distance. These are usually obtained, transcutaneously at the right common carotid artery and the right femoral artery (i.e. “carotid–femoral” PWV), and the time delay (Δt, or transit time) measured between the feet of the two waveforms. A variety of different waveforms can be used including pressure,15 distension and Doppler.8 The distance (D) covered by the waves is usually assimilated to the surface distance between the two recording sites. PWV is calculated as PWV = D (m)/Δt (s).
However, distance should be measured precisely because small inaccuracies may influence the absolute value of PWV. The shorter the distance between two recordings sites, the greater the absolute error in determining the transit time. Some investigators recommend either (a) using the total distance between the carotid and femoral sites of measurement, or (b) subtracting the distance from the carotid location to the sternal notch from the total distance, or (c) subtracting the distance from the carotid location to the sternal notch from the distance between the sternal notch and the femoral site of measurement. All three procedures are approximations and absolute differences are unimportant in intervention studies with repeated measures. However, when comparing two populations or pooling data for normal values or for meta-analyses, differences in the methods used to assess path length will be critically important.
Some limitations should be underlined. The femoral pressure waveform may be difficult to record accurately in patients with metabolic syndrome, obesity, diabetes and peripheral artery disease. In the presence of aortic, iliac, or proximal femoral stenosis, the pressure wave may be attenuated and delayed. Abdominal obesity, particularly in men, and large bust size in women, can make distance measurements inaccurate.
Methods based on pressure sensors
Pressure waveforms can be recorded simultaneously to provide automated measurement of PWV using a number of devices. The Complior System® (Artech-Medical, Pantin, France) employs dedicated mechanotransducers directly applied on the skin.15 The transit time is determined by means of a correlation algorithm between each simultaneous recorded wave. The operator is able to visualize the shape of the recorded arterial waves and to validate them. Three main arterial sites can be evaluated, mainly the aortic trunk (carotid–femoral), and the upper (carotid–brachial) and lower (femoral–dorsalis pedis) limbs. This system was used in most of the epidemiological studies demonstrating the predictive value of PWV for cardiovascular events (Table 4).
Pressure waves can also be recorded sequentially from different sites, and transit time calculated using registration with a simultaneously recorded ECG. In the SphygmoCor® system (ArtCor, Sydney, Australia), a single high-fidelity applanation tonometer (Millar®) allows obtaining a proximal (i.e. carotid artery) and distal pulse (i.e. radial or femoral), recorded sequentially a short time apart, and calculating PWV from the transit time between the two arterial sites.16 PWV is determined in relation to the R wave of the ECG: the time between ECG and proximal pulse is subtracted from the time between ECG and distal pulse to obtain the pulse transit time. The initial part of the pressure waveform is used as a reference point. It is also possible to check offline the variability of measurement over a range of pulses, according to each algorithm. Since the measurements are made a short time apart, the change in the isovolumic period of the left ventricle or heart rate variability has little or no effect on measured pulse transit times.
Methods based on Doppler probes and other methods
The distension waveforms of arterial diameter, obtained from high definition echotracking devices (see below), can be used to calculate PWV. Like described above for the SphygmoCor device, PWV is calculated from waves successively obtained at a short time interval at two arterial sites (common carotid and femoral artery for instance), using the R wave of the ECG for calculating the time delay.
The transit time, required for the determination of PWV, can be measured between two flow pulses simultaneously recorded by continuous Doppler probes,8 or again sequentially with ECG gating. Measurements are usually made at the root of the left subclavian artery (i.e. suprasternal notch on the skin) and near the bifurcation of the abdominal aorta (i.e. umbilicus level on the skin). Transit time is automatically calculated following automatic recognition of the foot of the pulse. This method was used for showing the predictive value of aortic PWV for cardiovascular events in diabetic patients,8 and provides a more accurate assessment of “aortic” PWV as compared to carotid–femoral, although whether this has any specific advantage remains to be seen.
Other devices are available to calculate a PWV-based stiffness index. These devices are not so precise as those mentioned above as some propose aberrant transit tracts (i.e. ankle-arm) or estimate distance from height (i.e. height in sitting position). Some do not correct for electromechanical dissociation of cardiac action or try to correct for it using a model. The latter device demonstrated that aorto-brachial PWV predicted CV events in hypertensives.
Local determination of arterial stiffness
Local arterial stiffness of superficial arteries can be determined using ultrasound devices. Carotid stiffness may be of particular interest, since in that artery atherosclerosis is frequent. All types of classical, bi-dimensional vascular ultrasound systems can be used to determining diameter at diastole and stroke changes in diameter, but most of them are limited in the precision of measurements because they generally use a video-image analysis. At present some researchers also measure local arterial stiffness of deep arteries like the aorta using cine magnetic resonance imaging (MRI). However, most of pathophysiological and pharmacological studies have used echotracking techniques (Table 1).
A major advantage is that local arterial stiffness is directly determined, from the change in pressure driving the change in volume, i.e. without using any model of the circulation (Fig. 2). However, because it requires a high degree of technical expertise, and takes longer than measuring PWV, local measurement of arterial stiffness is only really indicated for mechanistic analyses in pathophysiology, pharmacology and therapeutics, rather than for epidemiological studies.
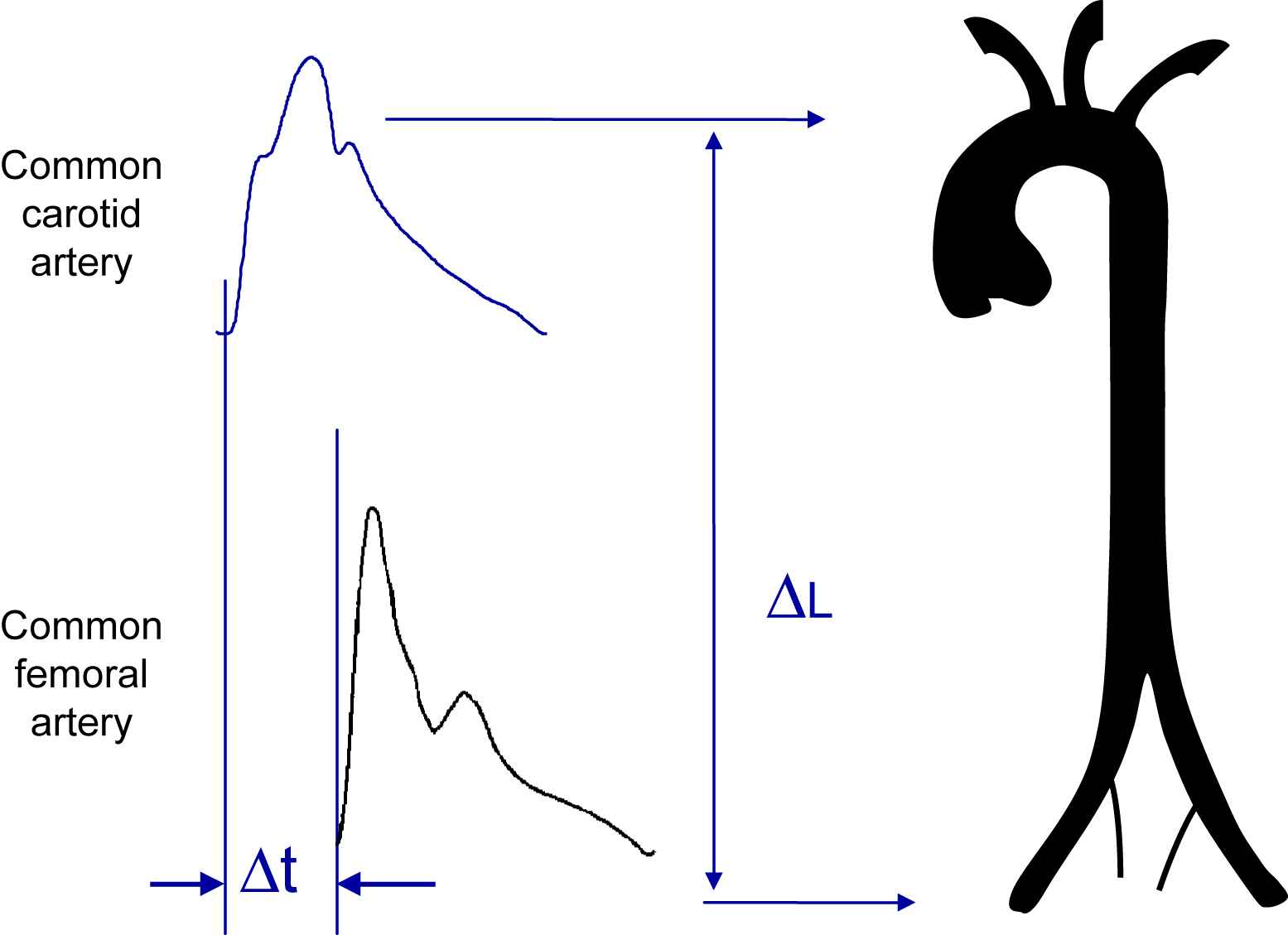
Measurement of carotid–femoral pulse wave velocity with the foot-to-foot method (from Ref. 1).
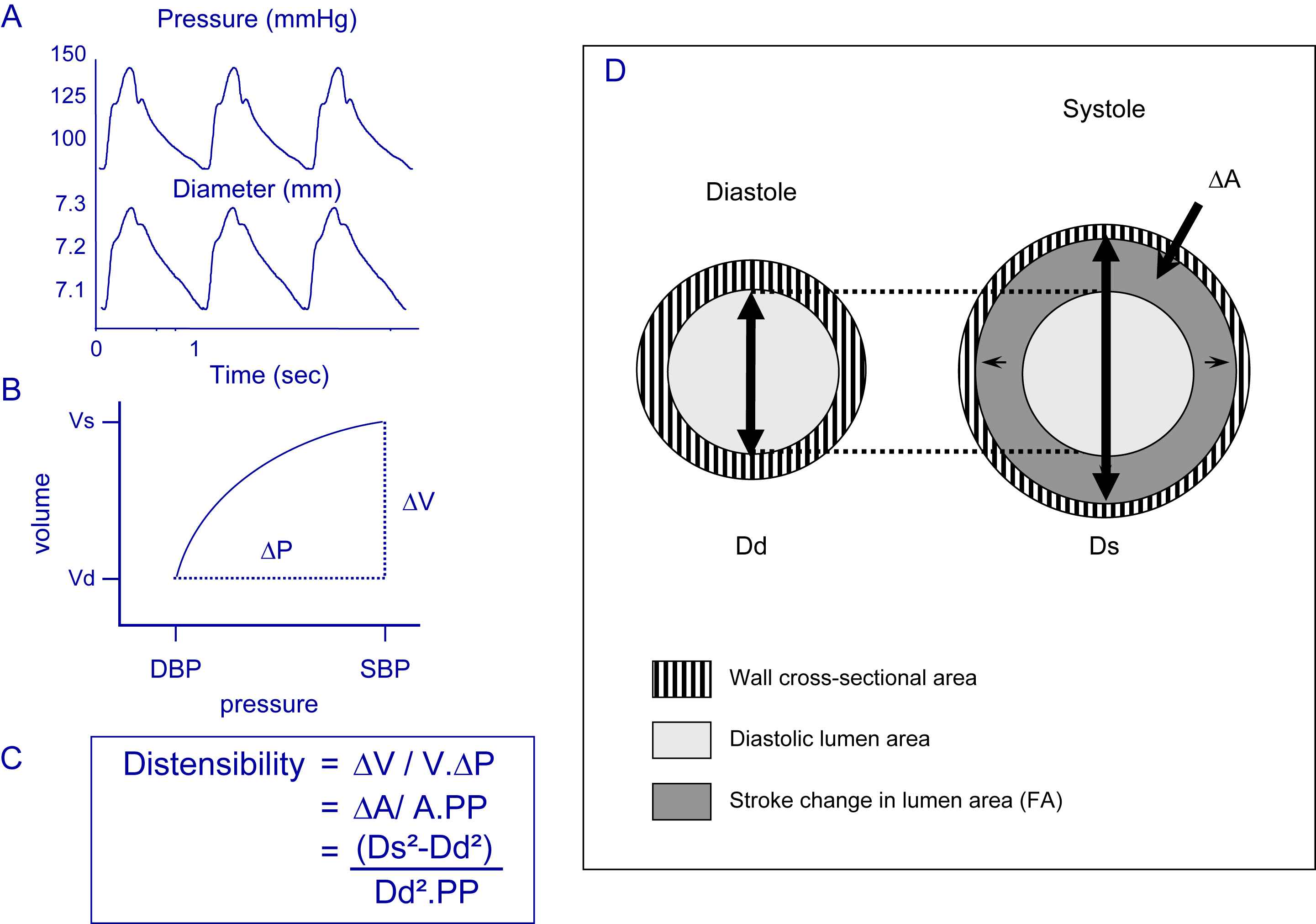
Local arterial distensibility. A: Simultaneous recording of stroke changes in BP and diameter. B: Pressure–diameter curve. C: Calculation of distensibility. D: Schematic representation of the stroke change (ΔA) in lumen cross-sectional area (LCSA). From Ref. 1.
Echotracking devices were developed to measure diameter in end-diastole and stroke change in diameter with a very high precision, 6–10 time higher than with video-image systems. Local pressure is usually obtained by applanation tonometry of the vessel in question and calibration of the waveform to brachial mean and diastolic pressures obtained by the integration of the brachial or radial waveform,17 or automatic calculation using transfer function processing (Sphygmocor, AtCor, Sydney Australia).16,18 All the superficial arteries are suitable for the geometrical investigation, and particularly the common carotid, common femoral and brachial arteries. Table 3 gives the definition of various indices used to describe the elastic properties of blood vessels, non-invasively obtained with ultrasound measurements.
Carotid stiffness was predictive of CV events (Table 4) in a small number of patients with ESRD19 or following renal transplantation,20 but had no independent predictive value in a larger number of patients with manifest arterial disease.13,21 This may be due to methodological reasons: the use of local (carotid) PP in positive studies19,20 and brachial PP in negative studies.13,21 In addition, upper and lower limb territories, due to their particular pathophysiology may not reflect aortic, cerebral and coronary artery damage.14
Position statement: local arterial stiffness
- -
Echotracking systems provide optimal conditions for a precise determination of local arterial stiffness, which is directly determined and requires no assumption from models of the circulation.
- -
Local arterial stiffness should be determined from (preferentially simultaneous) measurements of stroke changes in diameter and local pulse pressure.
- -
Echotracking systems additionally provide precise measurement of intima-media thickness, which allows calculation of Young’s elastic modulus.
- -
Determination of both carotid stiffness and thickness is optimal.
- -
Local measurements of arterial stiffness are indicated for mechanistic analyses in pathophysiology, pharmacology and therapeutics, rather than for epidemiological studies.
Systemic arterial stiffness
Systemic arterial compliance can be determined by various methods, including (a) a methodology based on an electrical circuit, based on a modified Windkessel model (proximal capacitive compliance and distal oscillatory compliance; HDI/PulseWave CR-2000 Research CardioVascular Profiling System; Hypertension Diagnostics Inc, Eagan, MN, USA); (b) the “area method” which requires measurement of aortic blood flow (velocimeter at the suprasternal notch) and associated driving pressure by applanation tonometry over the proximal right common carotid artery; and (c) the ratio between stroke volume and pulse pressure, which is a crude approximation. Until now, these methods did not provide evidence, in a longitudinal study, that systemic arterial stiffness or systemic arterial compliance have independent predictive value for CV events.
Non-invasive determination of wave reflections
Central pulse wave analysis
The arterial pressure waveform is a composite of the forward pressure wave created by ventricular contraction and a reflected wave. Waves are reflected from the periphery, mainly at branch points or sites of impedance mismatch. In elastic vessels, because PWV is low, reflected wave tends to arrive back at the aortic root during diastole. In the case of stiff arteries, PWV rises and the reflected wave arrives back at the central arteries earlier, adding to the forward wave, and augmenting the systolic pressure. This phenomenon can be quantified through the augmentation index (AIx) – defined as the difference between the second and first systolic peaks (P2 − P1) expressed as a percentage of the pulse pressure (Fig. 3). Apart from a high PWV, also changes in reflection sites can influence the augmentation index. In clinical investigation, not only DBP and height, which are related to reflection sites, but also age and aortic PWV, are the main determinants of AIx.
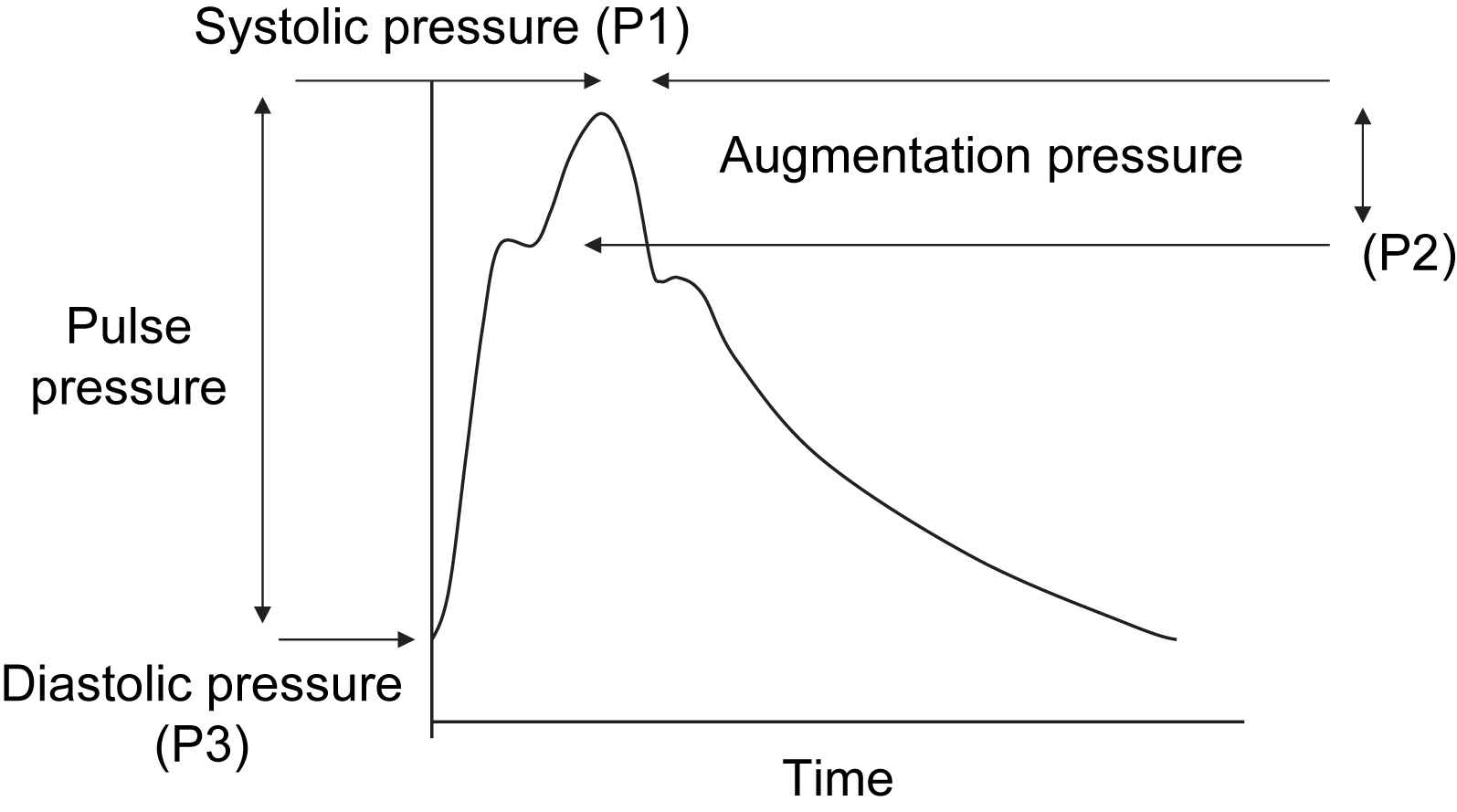
Augmentation index. Carotid pressure waveform is recorded by applanation tonometry. The height of the late systolic peak (P1) above the inflection (P2) defines the augmentation pressure, and the ratio of augmentation pressure to PP defines the augmentation index (AIx, in percent) (from Ref. 1).
Arterial pressure waveform should be analysed at the central level, i.e. the ascending aorta, since it represents the true load imposed to the left ventricle and central large artery walls. Aortic pressure waveform can be estimated either from the radial artery waveform, using a transfer function16,18 or from the common carotid waveform. On both arteries, the pressure waveform can be recorded non-invasively with a pencil-type probe incorporating a high-fidelity Millar strain gauge transducer (SPT-301, Millar Instruments). The most widely used approach is to perform radial artery tonometry and then apply a transfer function (Sphygmocor, AtCor, Sydney Australia) to calculate the aortic pressure waveform from the radial waveform.16,18 Indeed, by contrast to the carotid artery, the radial artery is well supported by bony tissue, making optimal applanation easier to achieve.
Individual and generalized inverse transfer functions are applied to reconstruct the aortic waveform from radial tonometry. The estimation of central aortic pressures is accepted as more accurate than the estimation of AIx. In addition, brachial artery pressures are used as surrogates of radial artery pressures for the calibration of central pressures, and this may introduce some errors. Despite these limitations, radial tonometry is popular since it is simple to perform and well tolerated. Carotid tonometry requires a higher degree of technical expertise, but a transfer function is not necessary since the arterial sites are very close and waveforms are similar. A transfer function may be useful when applanation tonometry cannot be applied at the site of the carotid artery, for instance in obese subjects, or in patients with major atherosclerotic plaques or calcified arteries, in whom this method may not be free from any risk. However, the use of a transfer function should be limited to the upper limb, where elastic properties remain relatively constant with age and disease. Two major issues in quantification of reflected waves on central pressure waveforms, i.e. the timing of the reflected wave and the estimation of absolute values of central pressures, have been detailed previously.1
Central augmentation index and central pulse pressure have shown independent predictive values (Table 5) for all-cause mortality in ESRD patients,22,23 and CV events in patients undergoing percutaneous coronary intervention24,25 and in the hypertensive patients of the CAFÉ study.26
| Parameter | First author (year, country) | Events | Follow-up (years) | Type of patient (number) | Mean age at entry (years) | Ref. |
|---|---|---|---|---|---|---|
| Central pulse pressure | Safar (2002, Fr) | All cause mortality | 4.3 | ESRD (180) | 54 | 23 |
| Williams (2006, UK) | CV events | 3.4 | HT, ASCOT study (2073) | 63 | 26 | |
| Carotid augmentation index | London (2001, Fr) | All cause and CV mortal. | 4.3 | ESRD (180) | 54 | 22 |
| Weber (2005, Austria) | Severe CV events | 2 | Undergoing PCI (262) | 66 | 24 | |
| Chirinos (2005,USA) | Severe CV events | 3.2 | Undergoing PCI (297) | 64 | 25 | |
| Williams (2006, UK) | CV events | 3.4 | HT, ASCOT study (2073) | 63 | 26 |
Legends as in Table 4; PCI: percutaneous coronary intervention.
Longitudinal studies reporting the independent predictive value of central pulse pressure and augmentation index (adapted from Ref. 1)
Position statement: central pulse wave analysis
Pulse wave analysis should be optimally obtained at the central level, i.e. at the site of the carotid artery or the ascending aorta, and either directly recorded or computed from the radial artery waveform using a transfer function. Pulse wave should be analyzed through three major parameters: central pulse pressure, central systolic pressure, and augmentation index.
Pulse wave analysis at peripheral sites
Other techniques were derived from peripheral waveform shape analysis. The determination of the amplitude ratios of the second derivative of the pulse pressure waveform, obtained by finger photoplethysmography (Fukuda Electric Co, Tokyo), was shown to be related to arterial distensibility and severity of atherosclerosis. A comparable device (Pulse Trace®, Micro Medical, Rochester, UK) has been developed, based on finger photoplethysmography, and validated in different settings and diseases.
Central and peripheral systolic and pulse pressures
Peripheral SBP and PP, most often measured at the site of the brachial artery, should not be confused with central SBP and PP, measured at the carotid site. Indeed, in peripheral arteries, reflection sites are closer than in central arteries, and reflected waves travel faster on peripheral arteries than on central arteries, which are less stiff in young subjects. Thus, according to the “amplification phenomenon”, the amplitude of the pressure wave is higher in peripheral arteries than in central arteries, and brachial SBP and PP overestimates central SBP and PP in young subjects.
Position statement: central and peripheral pulse pressures
Brachial SBP and PP should not be confounded with central SBP and PP, most often measured at the carotid site. Brachial SBP and PP overestimate central SBP and PP especially in young subjects.
Central pulse pressure, augmentation index and arterial stiffness
Because central SBP and PP, AIx and PWV increase with age, hypertension, diabetes mellitus, and hypercholesterolemia, and are associated with target organ damage (left ventricular hypertrophy, microalbuminuria, carotid intima-media thickening, and endothelial dysfunction) and clinical outcomes, they are often used interchangeably as indexes of arterial stiffness. This is an oversimplification and should not be the case for various reasons.
First, their determinants are different. Central SBP, central PP and AIx are dependent upon the speed of wave travel, the amplitude of reflected wave, the reflectance point, and the duration and pattern of ventricular ejection, especially with respect to change in heart rate and ventricular contractility whereas aortic PWV, which is the speed of wave travel, represents intrinsically arterial stiffness, according to the Bramwell–Hill formula (Fig. 1). Second, pathophysiological conditions and drugs may change central pulse pressure and augmentation index without changing aortic PWV, suggesting a predominant effect on reflection wave, heart rate or ventricular ejection, and no change in aortic stiffness. Third, AIx is much more sensitive to the effects of heart rate than aortic PWV. Fourth, in the normal population of the Anglo Cardiff Collaborative Study,27 the influence of age is higher on AIx than on aortic PWV before the age of 50, and higher on aortic PWV than on AIx after 50.
Position statement: use of central pressure, augmentation index and PWV
Central pressure, augmentation index and PWV cannot be used interchangeably as indexes of arterial stiffness. In contrast to PWV which is a direct measure of arterial stiffness, central pressure and AIx are only indirect, surrogate measures of arterial stiffness. However, they provide additional information concerning wave reflections. Central pulse wave analysis should be optimally coupled with the measurement of aortic PWV to determine the contribution of aortic stiffness to wave reflections.
In summary, various arterial parameters can be measured and calculated in order to evaluate non-invasively arterial stiffness and wave reflections. Various methods for arterial stiffness measurement are suggested to clinicians and researchers in Table 6. They have been established and ranked primarily according to various criteria: validation, limitations, predictive value and degree of technical expertise, as discussed above.
| Parameter | Main features and definition | Limitations | Predictive value for CV events | Degree of technical expertise |
|---|---|---|---|---|
| 1. Carotid–femoral PWV | +++ | + | ||
|
|
|||
| 2. Central pulse wave analysis (carotid and aortic pressure waves) | ++ | + | ||
|
|
|||
| 3. Local arterial stiffness | + | +++ | ||
|
|
|||
Methods for measuring arterial stiffness in clinical investigation
Position statement: methods for measuring arterial stiffness in clinical practice and research
- 1.
Carotid–femoral PWV is the “gold standard” for arterial stiffness, has the largest amount of epidemiological evidence for its predictive value for CV events, and requires little technical expertise.
- 2.
Central pulse wave analysis provides additional information concerning wave reflections. Central pressure and augmentation index have demonstrated their predictive value in patients with end-stage renal disease, in hypertensives, and in CAD patients, and require little technical expertise.
- 3.
Local arterial stiffness benefits from a certain amount of epidemiological evidence for its predictive value for CV events, requires a higher level of technical expertise, and is indicated for mechanistic analyses in pathophysiology, pharmacology and therapeutics.
Clinical applications
Arterial stiffness and wave reflection are now well accepted as the most important determinants of increasing systolic and pulse pressure in ageing societies, thus afford a major contribution to stroke and myocardial infarction. First, we will summarize the main pathophysiological mechanisms through which an increase in arterial stiffness and wave reflections cause CV complications. Second, we will review three major clinical applications of arterial stiffness and wave reflections: pathophysiological studies, routine use, and intervention studies.
Pathophysiology of cardiovascular complications
A generally accepted mechanistic view is that an increase in arterial stiffness causes a premature return of reflected waves in late systole, increasing central pulse pressure, thus systolic BP. SBP increases the load on the left ventricle, increasing myocardial oxygen demand. In addition, arterial stiffness is associated with left ventricular hypertrophy, a known risk factor for coronary events, in normotensive and hypertensive patients. The increase in central PP and the decrease in diastolic BP may directly cause subendocardial ischemia. The measurement of aortic stiffness, which integrates the alterations of the arterial wall, may also reflect parallel lesions present at the site of the coronary arteries. Indeed, aortic stiffening accompanying age and cardiovascular risk factors is caused by various phenomena, including breaks in elastin fibers, accumulation of collagen, fibrosis, inflammation, medial smooth muscle necrosis, calcifications, and diffusion of macromolecules within the arterial wall. All these phenomena are known to occur in parallel at the site of the coronary circulation.
An increased arterial stiffness can increase the risk of stroke through several mechanisms, including an increase in central PP, influencing arterial remodeling both at the site of the extracranial and intracranial arteries, increasing carotid wall thickness and the development of stenosis and plaques, the likelihood of plaque rupture, and the prevalence and severity of cerebral white matter lesion. The measurement of aortic stiffness, which integrates the alterations of the arterial wall, may also reflect parallel lesions present at the site of cerebral vasculature. Another explanation is given by the differential input impedance in the brain compared with other systemic vascular beds, leading to high-pressure pulsatility in brain and kidney. Finally, coronary heart disease and heart failure, which are favoured by high PP and arterial stiffness, are also risk factors for stroke.
Pathophysiological conditions associated with increased stiffness and wave reflection
Arterial stiffness and wave reflections are widely used in observational studies to analyse the determinants of hemodynamic changes observed in various clinical conditions, and to understand the pathogenesis of their CV complications. A large number of publications and several reviews reported the various pathophysiological conditions associated with increased arterial stiffness and wave reflections. Apart from the dominant effect of aging, they include (a) physiological conditions, such as sympathetic nervous system activity,28 low birth weight, menopausal status, lack of physical activity; (b) the genetic background such as a parental history of hypertension, diabetes or myocardial infarction, and genetic polymorphisms; (c) CV risk factors such as obesity, smoking, hypertension,29 hypercholesterolemia, impaired glucose tolerance, metabolic syndrome, type 1 and 2 diabetes, hyperhomocyteinemia, high CRP level, and acute inflammation30; (d) CV diseases such as coronary heart disease, congestive heart failure, and fatal stroke; and (e) primarily non-CV diseases, such as end-stage renal disease (ESRD), moderate chronic kidney disease, rheumatoid arthritis,31 systemic vasculitis and systemic lupus erythematosus.
The contribution of these different factors to arterial stiffness and wave reflections has been studied in multivariate analyses: the major parameters to be taken into account, when evaluating the degree of arterial stiffness, are age and blood pressure, and to a lower extent, gender and classical CV risk factors.
Arterial stiffness for routine use
A major reason for measuring arterial stiffness and wave reflections “routinely” in clinical practice comes from the recent demonstration that arterial stiffness has an independent predictive value for CV events.
Predictive value of arterial stiffness and wave reflections for CV events
Predictive value as intermediate end-point
Tables 4 and 5 summarize the longitudinal epidemiological studies which have demonstrated the independent predictive value of arterial stiffness, carotid pulse pressure and augmentation index, for CV events. The largest amount of evidence has been given for aortic stiffness, measured through carotid–femoral PWV. Aortic stiffness has independent predictive value for all-cause and CV mortality, fatal and non-fatal coronary events, and fatal strokes in patients with uncomplicated essential hypertension,4,7,9 type 2 diabetes,8 end-stage renal disease,3,6 elderly subjects10,13 and the general population.11,12 It is now well accepted that aortic stiffness is an intermediate end-point for CV events.
Data are less consistent concerning arterial stiffness measured at other arterial sites. Carotid stiffness was predictive of CV events in a small number of patients with ESRD19 or following renal transplantation,20 but had no independent predictive value in a larger number of patients with manifest arterial disease.13,21 Central augmentation index and pulse pressure, either directly measured by carotid tonometry22,23 or estimated using a transfer function from radial artery tonometry24,25 are both independent predictors of all-cause mortality in ESRD patients,22,23 and CV events in patients undergoing percutaneous coronary intervention,24,25 and in the hypertensive patients of the CAFÉ study,26 an ancillary study of the ASCOT trial (Table 5).
Position statement: predictive value of arterial stiffness and wave reflection for CV events
A large amount of evidence indicates that carotid–femoral PWV is an intermediate end-point for CV events, either fatal or non-fatal. Aortic PWV has a better predictive value than classical CV risk factors entering various types of risk score. Central augmentation index and pulse pressure have shown an independent predictive value for all-cause mortality in ESRD patients and CV events in hypertensives and patients with coronary disease.
Predictive value for the reduction in CV events
Whether the reduction in central PP is associated with a concomitant reduction in CV events, independently of the normalization of classical CV risk factors, remains to be demonstrated. Guerin et al.32 provided the first clear evidence in ESRD patients, showing that the insensitivity of PWV to reduced BP is an independent predictor of mortality. The CAFE study26 showed that central augmentation index and pulse pressure were both independent predictors of CV events in hypertensive patients, and that the reduction in central SBP and PP was higher in the amlodipine + perindopril group than in the atenolol + thiazide group, despite similar reduction in SBP and PP at the brachial level.
Position statement: predictive value of arterial stiffness and wave reflection for the reduction in CV events
Further studies are required to confirm the predictive value of arterial stiffness and wave reflection for the reduction in CV events in long-term intervention studies.
Normal values in different European countries
To allow a better understanding of the predictive value of indices of arterial stiffness for an individual patient, normal values applicable to individual populations are required. This requires both a cross-sectional and longitudinal approach in order to remove the potential influence of birth cohort effects and provide greater evidence of predictive values and causality. Differences between population normative data should be explored as they may help explain why cardiovascular risk varies between countries and what may be driving arterial stiffening.
Arterial stiffness in intervention studies
Non-pharmacological treatments which are able to reduce arterial stiffness include exercise training, dietary changes (including weight loss, low salt diet, moderate alcohol consumption, garlic powder, alpha-linoleic acid, and fish oil), and hormone replacement therapy (HRT).
Pharmacological treatments33 which are able to reduce arterial stiffness include (a) antihypertensive treatment, such as diuretics, beta-blockers, ACE inhibitors, AT1 blockers, and calcium channel antagonists; (b) treatments of congestive heart failure, such as ACE inhibitors, nitrates, and aldosterone antagonists; (c) hypolipidemic agents such as statins; (d) antidiabetic agents, such as thiazolidinediones; and (e) AGE-breakers, such as alagebrium (ALT-711).
Searching for target organ damage: measurement of arterial stiffness and wave reflection
The above paragraphs highlight the importance of arterial stiffness and wave reflection, not only for assessing CV risk, but also for predicting CV outcomes. Arterial stiffening also provides direct evidence of target organ damage, which is of major importance in determining the overall CV risk of the hypertensive patient. Indeed, measurement of arterial stiffness and wave reflection may avoid patients being mistakenly classified as at low or moderate risk, when they actually have an abnormally high arterial stiffness or central PP placing them within a higher risk group.
Position statement: arterial stiffness as target organ damage
Arterial stiffness and central pressure measurements should be considered as recommended tests for the evaluation of CV risk, particularly in patients in whom target organ damage is not discovered by routine investigations.
References
Cite this article
TY - JOUR AU - Stephane Laurent AU - John Cockcroft AU - Luc Van Bortel AU - Pierre Boutouyrie AU - Cristina Giannattasio AU - Daniel Hayoz AU - Bruno Pannier AU - Charalambos Vlachopoulos AU - Ian Wilkinson AU - Harry Struijker-Boudier AU - on behalf of the European Network for Non Invasive Investigation of Large Arteries PY - 2007 DA - 2007/06/06 TI - Abridged version of the expert consensus document on arterial stiffness☆ JO - Artery Research SP - 2 EP - 12 VL - 1 IS - 1 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2007.03.003 DO - 10.1016/j.artres.2007.03.003 ID - Laurent2007 ER -