
Hemodynamic impacts of entrainment of heart rate and stride rate
- DOI
- 10.1016/j.artres.2012.05.001How to use a DOI?
- Keywords
- Walking; Running; Wave reflection; Enhanced external counterpulsation
- Abstract
Synchronization of heart rate and step rate has been hypothesized to create a hemodynamically favorable situation where heart motion and bodily motion are in constant harmony so that stroke volume and cardiac output enhanced and oxygen delivery to the tissues is increased. The primary aim of the present investigation was to determine the impact of synchronization of step rate and heart rate on cardiovascular functions. Twenty-three apparently healthy subjects performed treadmill running in three different conditions, one that the step rate was matched with the heart rate (matched condition), one that the step rate was ~10 steps greater or lower than heart rate (unmatched conditions). Beat-by-beat blood pressure was measured using the finger plethysmography, and stroke volume and cardiac output were calculated using the validated Model Flow method. Average heart rate and blood pressures were not different among the 3 conditions. There were no differences in double products among the 3 conditions. Stroke volume and cardiac output were greater (P < 0.05) in the matched condition than in the unmatched conditions. Our present results are consistent with the idea that synchronization of heart motion and bodily motion augments stroke volume and cardiac output, presumably through the mechanism similar to the arterial counterpulsation.
- Copyright
- © 2012 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Muscular activity, both voluntary and involuntary, has a strong tendency to be periodic, and the rhythms of several physical and physiological activities (e.g., pulse, respiration, stepping, chewing) are usually in accord.3 Human locomotion is no exception and is characterized by up and down movements of torso and trunk and alternating movements of right and left limbs. Bodily movement during running or treadmill exercise generates pressure waves in the arterial system. It has been suggested that when heart rate and step rate are synchronized, negative pressure waves generated by upward bodily movements reaches the heart during systole, decreasing myocardial oxygen consumption, and augmenting ventricular ejection by decreasing afterload, whereas its positive component returns during diastole, enhancing coronary perfusion pressure.8 In this context, synchronization of heart rate and step rate could mimic arterial counterpulsation (as provided by intra-aortic balloon pump) or enhanced external counterpulsation (EECP)1 and could create a favorable situation where heart motion and bodily motion are in constant harmony, with one aiding the other, so that stroke volume and cardiac output enhanced and oxygen delivery to the tissues is increased over that possible with normal cardiac function alone. Indeed synchronization between heart rate and locomotor activity has been observed in humans during a variety of activities including cycling, walking, and running.6
Accordingly, the primary aim of the present investigation was to determine the impact of entrainment of step rate and heart rate on cardiovascular functions. We hypothesized that the synchronization of step rates and heart rates would augment stroke volume and cardiac output.
Methods
Subjects
Twenty-three apparently healthy subjects (16 males, 7 females) aged 19–39 years were studied. All subjects were normotensive, non-smokers, and free of overt cardiovascular diseases as assessed by medical history questionnaire. Subjects were either recreationally active or endurance trained (e.g., runners). All procedures involved in the study were explained, and written informed consents were obtained from all the subject. The study was reviewed and approved by the local Institutional Review Board.
Procedures
Subjects were required to fast and abstain from coffee and alcohol for at least 4 h before the start of the study, and each subject was instructed not to indulge in any strenuous physical activity for 24 h prior to the study.
Blood pressure was measured using the finger plethysmography placed on the subject’s right hand (Portapress, TNO TPD Biomedical Instruments, The Netherlands). In this technique, the plethysmographic cuff is placed around the middle phalanx of the finger and the cuff pressure is modulated to maintain transmural pressure at an effective zero. Prior to each measurement period, finger blood pressure was calibrated to brachial blood pressure. In order to minimize the motion artifacts, subjects were instructed to put their right hand on the table (i.e., hand rest) positioned at the heart level and were asked not to flex and/or extend the cuffed finger throughout the measurement. All data were acquired continuously at 200 Hz with an analog-to-digital converter. Beat-by-beat results were subsequently analyzed with the Beatscope software (TNO TPD Biomedical Instruments), which calculated stroke volume and cardiac output using the validated Model Flow method.11,12 The use of this technology has been evaluated to be valid during exercise.11 Heart rate was monitored with a S610 heart rate monitor (Polar, Lake Success, NY) strapped around the chest of the subject.
Prior to the main protocol, the subjects performed multiple bouts of running in order to search and determine a running condition in which the step rate and heart rate could be matched. This was done by manipulating the treadmill speed and/or the treadmill grade. The main protocol consisted of 6 experimental running sessions with sufficient resting intervals between bouts. The 6 running sessions were performed at the same treadmill speed and grade and were divided into three different conditions in duplicate, one that the step rate was matched with the heart rate (matched condition), one that the step rate was ~10 steps greater than heart rate, and one that the step rate was ~10 steps lower than heart rate. The subjects changed their step rate according to beep frequency set on the metronome. The mean treadmill speed and grade were 2.5 ± 0.5 m/sec and 2.0 ± 1.6%. The entire protocol took ~2 h to complete for most subjects.
Statistical analyses
Data were analyzed using ANOVA with repeated measures. Statistical significance was set a priori at P < 0.05 for all comparisons. Data are expressed as mean ± SEM in figures and mean ± SD elsewhere.
Results
Selected subject characteristics are shown in Table 1. The subjects were apparently healthy with clinically normal blood pressure. The effects of entrainment of heart rate and step rate on cardiovascular functions as compared with unmatched conditions are shown in Table 2. Average heart rate was not different between 3 conditions whereas the step rate was ~10 steps/min different in the unmatched conditions than in the matched condition (P < 0.01). Both systolic and diastolic blood pressures were not different among the 3 conditions. There were no differences in double products between the conditions. Stroke volume and cardiac output were higher (P < 0.05) in the matched condition as compared with the unmatched conditions as shown in Fig. 1. There was no significant difference in total peripheral resistance between the 3 conditions (P > 0.05). A type of “beating” pattern, where pulse pressure rhythmically increase and decrease in pattern, was observed in some subjects (Fig. 2).
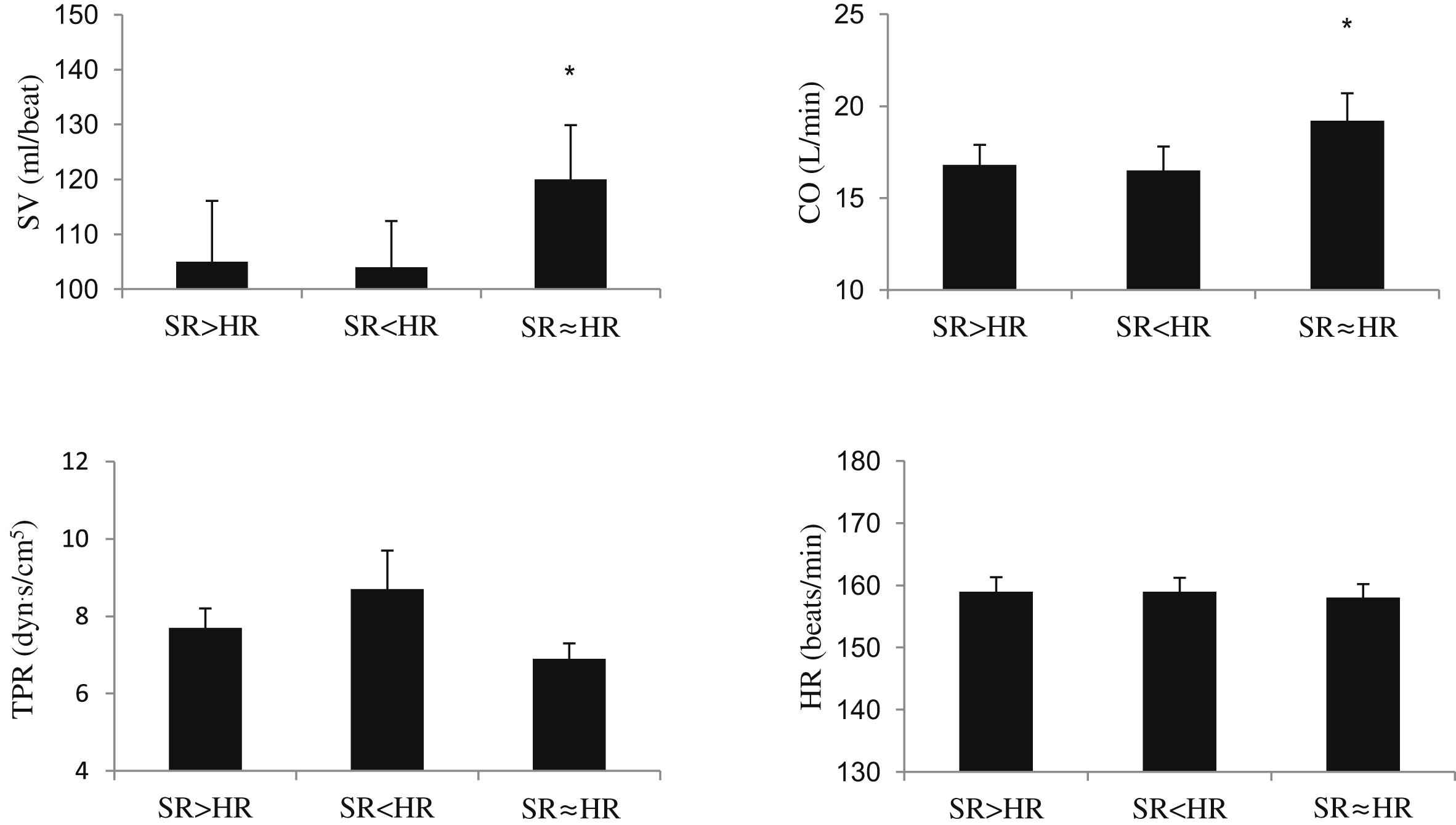
Changes in cardiac output (CO), stroke volume (SV), heart rate (HR), and total peripheral resistance (TPR) with entrainment of step rate (SR) and heart rate. Data are means ± SEM. *P < 0.05 vs. other two (ie, unmatched) conditions.
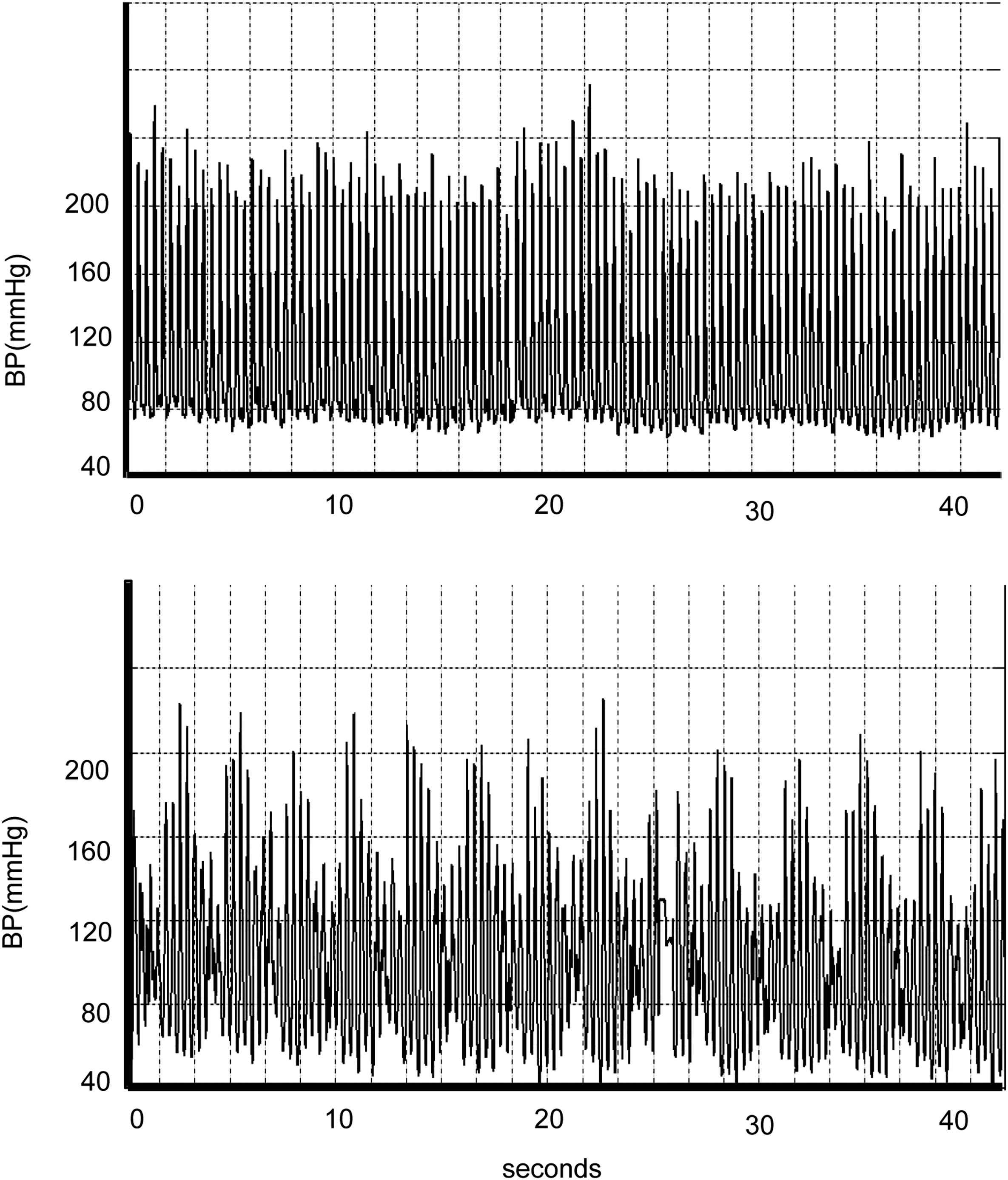
A representative recording of the beating phenomenon resulting from the combined effects of two different waves, one generated by the heart and the other generated by foot stride shock.
| Variable | Mean ± SD |
|---|---|
| n | 23 |
| Male/female | 16/7 |
| Age (yr) | 26.8 ± 5.1 |
| Height (cm) | 171 ± 10 |
| Body mass (kg) | 69 ± 12 |
| Body mass index (kg/m2) | 23.4 ± 2.2 |
| Systolic BP (mmHg) | 118 ± 11 |
| Diastolic BP (mmHg) | 72 ± 9 |
BP = blood pressure.
Selected subject characteristics.
| Unmatched conditions | Matched condition | ||
|---|---|---|---|
| SR > HR | SR < HR | SR ≈ HR | |
| Systolic BP (mmHg) | 156 ± 18 | 160 ± 25 | 164 ± 28 |
| Diastolic BP (mmHg) | 86 ± 10 | 89 ± 15 | 86 ± 8 |
| Mean BP (mmHg) | 110 ± 12 | 113 ± 17 | 112 ± 14 |
| Heart rate (beats/min) | 159 ± 11 | 159 ± 10 | 158 ± 10 |
| Step rate (steps/min) | 169 ± 10 | 151 ± 11 | 160 ± 10 |
| Double products (U) | 24790 ± 3540 | 25424 ± 4116 | 26015 ± 4837 |
Data are expressed as mean ± SD.
BP = Blood pressure.
Effects of entrainment of heart rate (HR) and step rate (SR) on cardiovascular variables during exercise.
Discussion
The salient finding of the present study is that stroke volume and cardiac output were elevated when heart rates and step rates were synchronized. This was observed when there were no differences in both systolic and diastolic blood pressure between the 3 conditions.
It has been speculated that the synchronization of heart rate and step rates could augment ventricular ejection during systole, enhance coronary perfusion during diastole, and reduce myocardial oxygen demand.8 In contrast, we observed that both systolic and diastolic blood pressures were not different among all the conditions. Additionally, there were no differences in an index of myocardial oxygen demand (double products calculated as systolic blood pressure times heart rate). These results are not consistent with the notion that the synchronization of heart rate and stride rates would modulate blood pressure and myocardial oxygen demands. However, it should be noted that we did not measure “central” blood pressure in the present study and it is possible that the measurement of central, rather than peripheral, blood pressure may have yielded a very different results. Interestingly, both stroke volume and cardiac output were greater when heart rates and step rates were matched. It is not clear what explains the greater stroke volume and cardiac output when stride rate and heart rate were entrained. One possible explanation is that blood flow to working skeletal muscle might be augmented and cardiac afterload might be reduced if peak intra-arterial pressure reaches muscular beds when peak intramuscular pressure is lowest.7 This would theoretically reduce cardiac afterload and act to enhance stroke volume. Indeed a modeling study using the phase locking of heart rates to rhythmic thigh cuff occlusion as a simulation of intramuscular pressure change during locomotion supports such explanation.7 It remains to be determined if such intricate phase locking occurs in free-living or free-exercising humans. A new technique that can simultaneously monitor ECG and stride rate via force sensitive foot switches would be necessary to address such question.5 Further studies using such technology are clearly warranted.
In many exercising situations, the rates of bodily motion (e.g., stride rate) and cardiac motion (e.g., heart rate) are often very close. For example, elite distance runners have a stride rate of ~175–185 strides/min2 that is very close to their heart rate recorded during the distance race.4 There are a number of possible physiological explanations that have been suggested as to how the synchronization of bodily motions and cardiac motions could be achieved. The milking actions of muscle contractions act as muscle pump and enhance venous return and stroke volume via Frank–Starling mechanisms. Additionally, mechanoreceptors within the skeletal muscle generates afferent signals in response to repetitive muscle contractions and could affect heart rate via inhibition of cardiovagal components of arterial baroreceptors. Currently, it is unknown if such entrainment of heart rate and stride rate would result in better athletic performance in runners. Similarly, it remains to be determined whether such condition would be favorable for cardiac patients undergoing cardiac rehabilitation programs although arterial pressure, heart rate, and double products were not different between the 3 conditions. Results from the previous studies using the EECP as a rehabilitative measure support such assertion.1
During the uncoupling conditions of cardiac and locomotor rhythms, we observed rhythmic fluctuations in pulse pressure that showed a periodic widening and narrowing in pattern. These fluctuations tend to be disregarded as motion artifacts but are indeed real as has been observed in many different investigations. This peculiar pattern was first reported by Rowell et al.10 and was termed the “beat phenomenon” by Palatini et al.9 These rhythmic oscillations were not related to respiration and were not observed during cycling.9 It has been attributed to the interaction between heart rate and stride rate with the periods of high pulse pressure caused by cardiac and bodily waves being synchronized and the periods of low pulse pressure caused by cardiac and bodily waves being 180° out of phase.8
As in any other studies, the present study has several limitations that should be emphasized. First, stroke volume was indirectly estimated from the arterial waveforms. Although the model flow methods to derive stroke volume have been well validated even during exercise, it is nevertheless an indirect method to estimate stroke volume.11 Second, it was rather difficult to produce 3 different conditions, including step rates ≅ heart rates, heart rates ~10 bpm lower or higher than step rates. In some subjects, we had to perform multiple bouts of treadmill running over many days in order to create all three conditions. Even though we did not observe any subjective or objective signs of fatigue during the testing, we cannot exclude the possibility that fatigue might have affected the results. Third, even though we were successful in locking frequencies of heart rate and stride rate, we did not manipulate phase differences.
In summary, the results of the present study indicate that the entrainment of heart motion (heart rate) and bodily motion (stride rate) augments stroke volume and cardiac output presumably through the physiological mechanisms analogous to the EECP.
References
Cite this article
TY - JOUR AU - Mandeep S. Dhindsa AU - Jun Sugawara AU - Hirofumi Tanaka PY - 2012 DA - 2012/06/07 TI - Hemodynamic impacts of entrainment of heart rate and stride rate JO - Artery Research SP - 136 EP - 140 VL - 6 IS - 3 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2012.05.001 DO - 10.1016/j.artres.2012.05.001 ID - Dhindsa2012 ER -