
Combating Open Defecation through Community-led Sanitation
- DOI
- 10.2991/dsahmj.k.190626.001How to use a DOI?
- Keywords
- Economy; environment; fecal–oral route; gender equality; infectious diseases; open defecation; sustainable development goals
- Abstract
This article discusses how the practice of open defecation influences the Sustainable Development Goals (SDGs) set by the United Nations (UN) and accepted by all countries. Unfortunately, the practice of open defecation still exists. Public health is at stake because open defecation enables transmission of infectious diseases via the fecal–oral route. Open defecation could hinder achieving the targets set for sustainable development. Poverty is one of the prime reasons for open defecation and this in turn has negative effects on social outcomes, wellbeing, ecosystems, and the economy. This article highlights the areas in which open defecation could prevent attainment of SDGs, and justifies the recent sanitation interventions by various countries to curb the practice of open defecation.
- Copyright
- © 2019 Dr. Sulaiman Al Habib Medical Group. Publishing services by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Open defecation alludes to the practice whereby people go out to open fields, roadsides, bushes, periphery of water bodies, or other open spaces rather than using the toilet [1]. The practice of open defecation has deep roots and is considered culturally acceptable behavior in some low- and middle-income countries [2]. Some of the factors that contribute to open defecation are high density of population, lack of toilets, poverty, and the beliefs that defecating in the open is normal and healthy, and that building a lavatory in the house would be insanitary [3].
Target 6.2 of the United Nations (UN) Sustainable Development Goals (SDGs) emphasizes the provision of sanitation facilities and promotes hygiene habits for all. Ending the practice of open defecation is a top priority under this target. SDG 6 recommends special consideration for women, girls, and those in susceptible situations with regards to sanitation and hygiene requirements [4]. Accessibility to basic sanitation and hygiene does have a major impact on public health, child mortality, education, economic development, and ecosystem quality [5]. Women and girls are not only susceptible to the health consequences of poor sanitation, but also to the danger of physical assaults and wild animal encounters [6].
Sustainable development is achieved through three interlinked dimensions, namely, environment, society, and economics. This article focuses on the public health implications of open defecation and its consequences for sustainable development. The sanitation-related targets of the SDGs aim to ensure that all humans worldwide should have well-managed sanitation facilities by 2030 and that the practice of open defecation is eliminated. This article highlights the SDGs that will not be achieved if open defecation is not eliminated.
2. FECAL–ORAL ROUTE: HIGHWAY FOR PATHOGENS
Human feces contain various protozoa, bacteria, viruses, and helminths [7]. The fecal–oral route enables transmission of these pathogens from infected to healthy persons via direct or indirect contact with contaminated liquids, food, and carriers such as fomites [8,9]. Figure 1 shows a variant of the F diagram that was described by Wagner and Lanoix [10]. Bacteriophages are viruses that infect bacteria, and coliphages are viruses that infect coliform bacteria [11]. Bacteria that develop in the gastrointestinal tract are called enteric bacteria, which typically may not survive for long periods in the external environment. Protozoa are single-celled organisms with nuclei. Protozoan parasites that infect humans can produce cysts (or oocysts) that can survive in the environment. These cysts or oocysts have a thick cell wall that protects them and confers resistance to disinfection. Helminths are worm-like organisms that are multicellular in nature and able to thrive in humans. Common types of helminths include roundworms, tapeworms, hookworms, and trematodes. Helminth eggs are excreted from infected humans through the feces and can survive in the environment, such as in water and soil. Table 1 lists the infectious diseases that originate from the fecal–oral route [12,13].
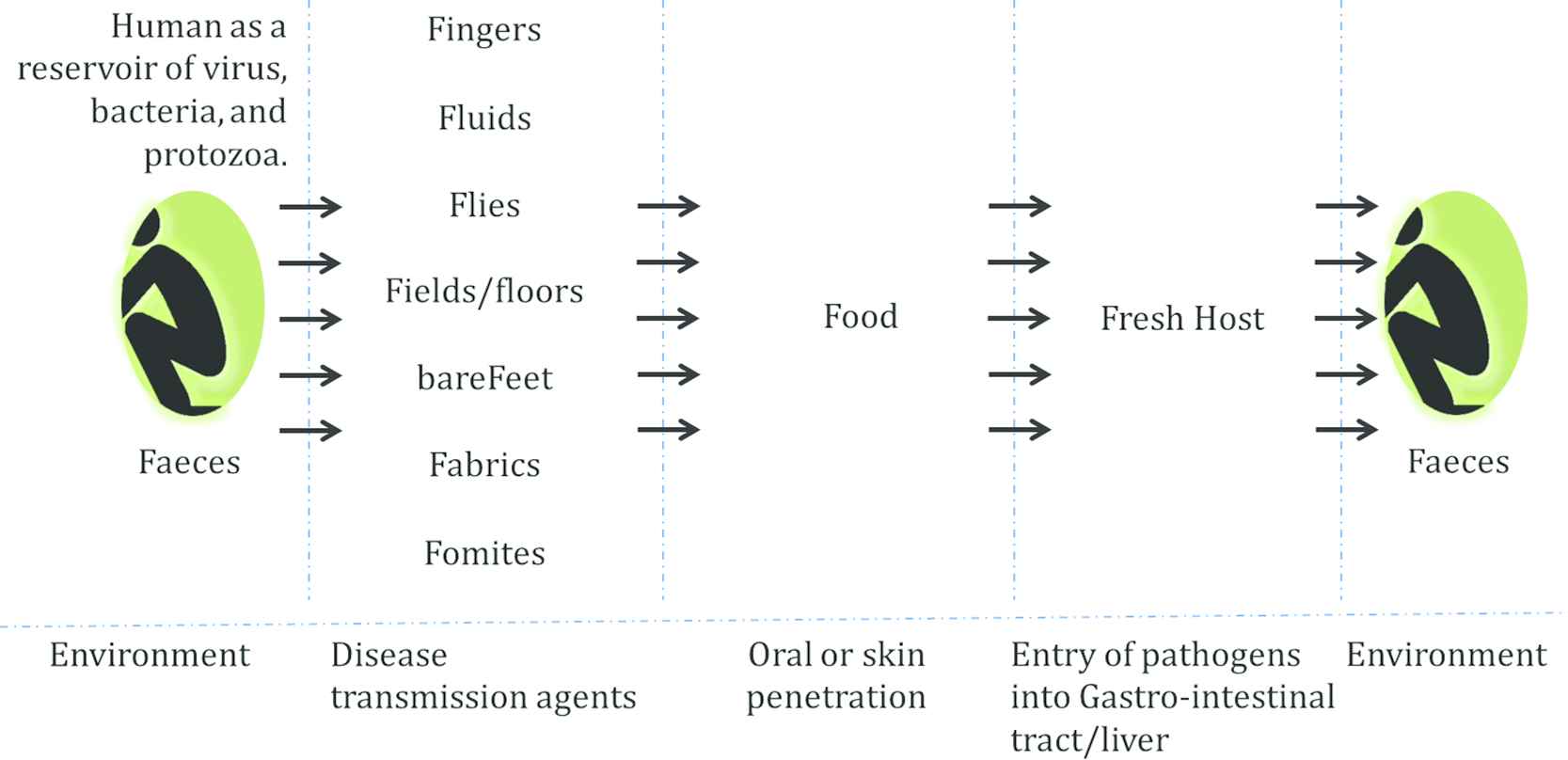
Figures representing a form of F diagram. The basis for transmission of infectious diseases from human to human is through the fecal–oral route.
| Infection and infectious agent | Epidemiology |
|---|---|
| Viral liver diseases | |
| Infectious hepatitis – hepatitis A (genus Hepatovirus) |
|
| Intestinal infectious diseases | |
| Food poisoning by Salmonella (Salmonella gastroenteritis) – Salmonella enterica |
|
| Cholera – Vibrio cholerae | By the process of water/food ingestion of that was contaminated with vomitus or feces of infected person |
| Giardiasis – Giardia lamblia | Occurs by hand to mouth transfer of cysts from feces of an infected individual |
| Amoebiasis (amoebic dysentery) – Entamoeba histolytica |
|
| Bacillar dysentery – shigellosis (Shigella dysenteriae, Shigella flexneri, Shigella boydii, and Shigella sonnei) |
|
| Diarrhea – Escherichia coli | Ingestion of contaminated water |
| Rotavirus |
|
| Typhoid fever – Salmonella typhi |
|
| Parasitic infections (protozoal and helminthic) | |
| Hookworm disease (ancylostomiasis, necatoriasis) – Ancylostoma duodenale and Necator americanus | Through skin penetration by the infective larvae |
| Strongyloidiasis – Strongyloides stercolaris | Infective larvae will penetrate through the skin and impacts the venous circulation |
| Entrobiasis (oxyuriasis, pinworm infection) – Entrobius vermicularis | Infective eggs will directly transfer from the anus to mouth of the same or another person or indirectly though clothing, bedding, food or other articles contaminated with eggs of the parasite |
| Trichuriasis – Trichuris trichuria (whip worm) | Ingestions of contaminated vegetables |
| Ascariasis – Ascaris lumbricoides (round worm) | Ingestion of infective eggs from soil contamination with human feces |
List of infectious diseases caused by fecal–oral route transmission
Human feces are the primary source of pathogens that cause diarrheal diseases such as cholera, typhoid and amoebic dysentery [13]. Hepatitis A is highly correlated with open defecation and geophagia. On similar lines, hepatitis E spreads through drinking water contaminated by human feces. Soil-transmitted helminths are another health risk associated with open defecation. The most common helminths that infect humans are Old World hookworm (Ancylostoma duodenale), New World hookworm (Necator americanus), roundworm (Ascaris lumbricoides), whipworm (Trichuris trichiura), and threadworm (Strongyloides stercoralis) [14]. In the soil-transmitted helminth infectious life cycle, the parasites inhabit the human intestines, reproduce sexually, and produce eggs, which are transferred to the soil or external environment through the feces [15]. Under certain conditions, these fertilized eggs can live in the environment for several months. Infection occurs through accidental ingestion of eggs or penetration through the skin [16].
3. IMPACT OF OPEN DEFECATION ON THE PILLARS OF SUSTAINABLE DEVELOPMENT
Environmental factors play an important role in transmission efficiency and multiplicity of infection. For instance, disaster events like floods in regions where open defecation is prevalent can contaminate the surface water and amplify the conditions to cause an outbreak [17]. Vegetables or foodstuff can be contaminated due to the use of sewage-sullied water or other resources that contain traces of human excrement. Vegetable products that are contaminated due to infected irrigation water play an important role in spreading human pathogens.
Figure 2 depicts the environmental and economic problems caused by open defecation. The practice of open defecation is a behavioral problem at the societal level and it is a major cause of infectious diseases. Moreover, there are other less-tangible issues that are difficult to tackle, such as women’s privacy, women’s risk of physical attack and abuse, and child stunting problems.
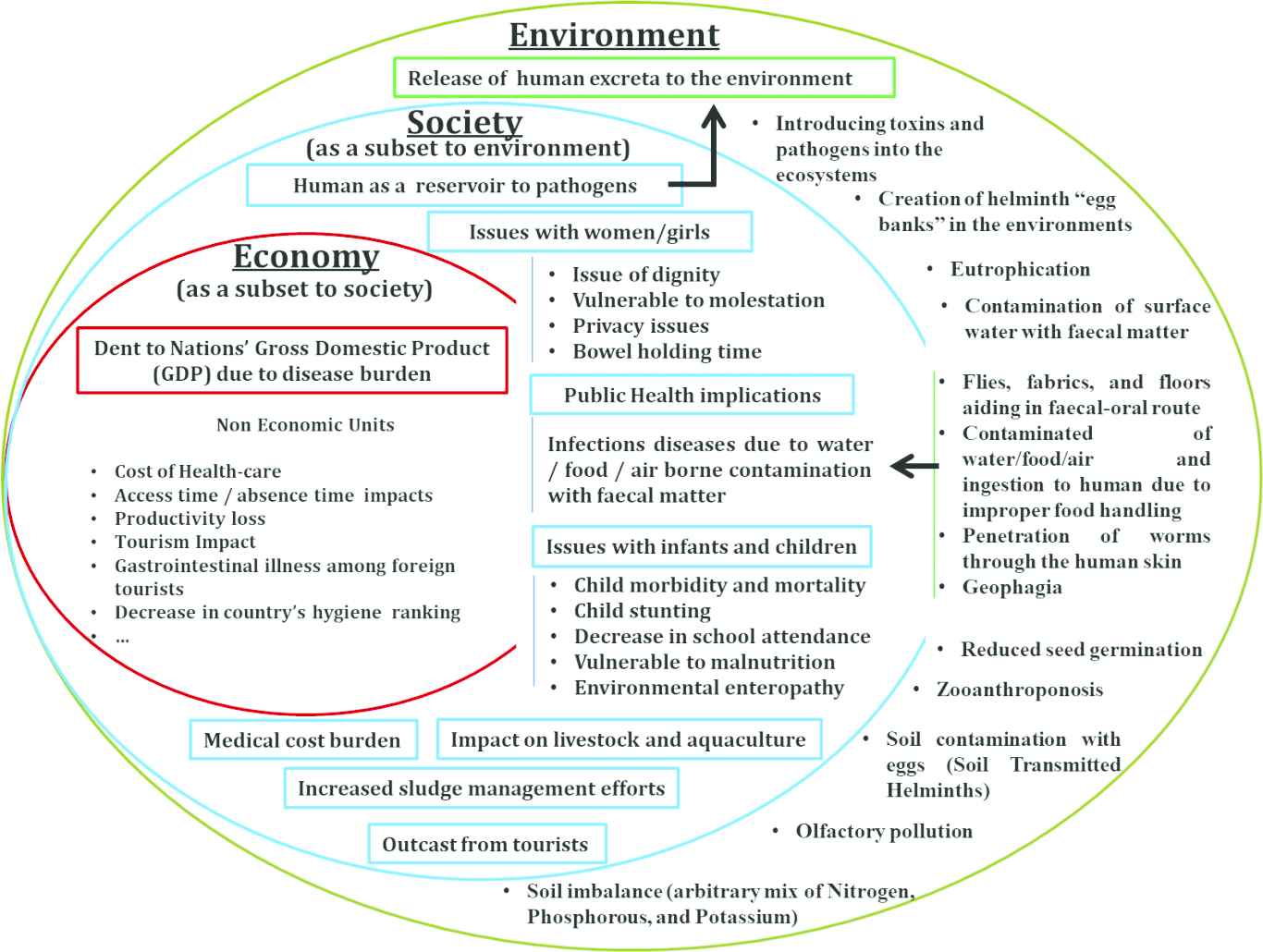
Illustration of the impact of open defecation on economy, society and environment.
Lack of sanitation facilities cost the global economy US$222.9 billion in 2015 alone, and this figure constitutes a significant portion of combined Gross Domestic Product (GDP) of the countries that were affected by poor sanitation [18]. Countries in the Asia–Pacific region carry the heaviest burden of poor sanitation, which is almost 77% of this total amount. The situation in India is the best example to understand the scale of the economic burden due to open defecation. The economic impact reported by De Francis (on behalf of the World Bank Water and Sanitation Program) is 6.4% of GDP for India in 2006. In 2015, India faced economic losses of US$106.7 billion and 5.2% of GDP [19]. Table 2 shows the top countries that were practicing open defecation as of 2015, according to the UN Children’s Fund (UNICEF) [20].
| Top 10 countries practicing open defecation based on their population (in thousands) | Top 10 countries practicing open defecation based on the maximum percentage of their population (%) | ||
|---|---|---|---|
| India | 522,261 | Eritrea | 76 |
| Nigeria | 46,530 | Niger | 71 |
| Indonesia | 32,063 | Chad | 68 |
| Ethiopia | 26,998 | South Sudan | 61 |
| Kenya | 26,998 | Benin | 55 |
| Pakistan | 21,813 | Togo | 51 |
| China | 20,778 | Burkina Faso | 48 |
| Niger | 14,190 | Madagascar | 44 |
| Sudan | 10,729 | Cambodia | 41 |
| Madagascar | 10,646 | India | 40 |
| Mozambique | 10,646 | ||
Top 10 countries practicing open defecation as of 2015
Noneconomic units that are vulnerable to open defecation include the indirect costs of health impacts (e.g., cost of health care incurred in treatment of diseases due to poor sanitation, premature mortality, and loss of productivity), time impacts (e.g., cost of school/work absence), and tourism impact (e.g., loss of tourism revenues). Hutton et al. [21] mentioned that visits to open defecation sites outside the home result in waste of almost 30 min per person per day and approximately 192.5 h per person per year.
The harmful societal effects of open defecation include infectious diseases at the community level, malnutrition and stunting in children, and exposure of women and girls to the risk of molestation. Ambesh and Ambesh [2] reported that open defecation is a major cause of fatal diarrhea, and on a daily basis, many children aged <5 years succumb to diarrhea. Mara [22] mentioned a set of health problems related to open defecation: stunting and long-term cognitive impairment, intractable intestinal infections, persistent effects of soil-transmitted helminthiasis, environmental enteropathy, giardiasis, small intestinal bacterial overgrowth, and anemia. Saleem et al. [6] have reported the social and health consequences of open defecation for women: such as threats to privacy and dignity, and psychosocial stress.
Open defecation results in environmental degradation that directly affects health and quality of life [23]. Environmental impacts of accumulation of human excreta have adverse effects on the bacteriological quality of drinking water [24]. Open defecation can introduce toxins and bacteria into the ecosystem, which may harm aquatic life.
4. HOW OPEN DEFECATION CRIPPLES SDGS
The 17 SDGs are integrated, indivisible, and interlinked. Failure in any one of the targets will hamper the others. Open defecation could affect the targets related to SDG 6, SDG 3, SDG 4, and SDG 5, which deal with clean water and sanitation, health and wellbeing, quality education, and gender equality, respectively. The interlinked nature of these universal goals will influence the other SDGs dealing with the environment and economy.
4.1. Impact of Open Defecation on SDG 1
- •
Open defecation amplifies the scope of infectious diseases originating via the fecal–oral route. The disease burden may have an adverse effect on GDP and hinder efforts at ending poverty.
- •
Usually, income is calculated for the entire household. If one member becomes ill due to diarrheal disease then it may have an impact on total consumption or income of the household.
- •
The disease burden may interact with the standard operating procedure of social protection systems and may disturb the planned budget allocations.
- •
People with disease and those who are vulnerable to the infectious diseases caused by open defecation may not be in a fit condition to face environmental disasters and economic shocks.
- •
Open defecation increases government spending on essential services in connection with the health sector, which may have an impact on the planned budget allocations.
4.2. Impact of Open Defecation on SDG 2
- •
Diarrheal diseases result in undernourishment and affect the dietary vitality that is required to maintain a typical active and healthy life.
- •
- •
Soil-transmitted helminths can affect agriculture, aquaculture, and pisciculture productivity due to the introduction of geohelmthis in the soil.
- •
Open defecation can reduce the productivity of the farmland due to contaminated irrigation water. Seed germination may also be affected by toxic content of the soil that is contaminated with fecal matter.
4.3. Impact of Open Defecation on SDG 3
- •
Diarrheal diseases are predominantly due to open defecation. The neonatal and under-five mortality rates may be affected by diarrheal diseases.
- •
Water and soil contamination with the fecal material may increase morbidity and mortality. It may be difficult to counteract tropical diseases, water/food-borne diseases, and other communicable diseases if open defecation is not eradicated.
- •
Spears et al. have shown that an increase in open defecation results in increased cases of stunting and severe stunting [26].
- •
Mara [22] has reported the health implications of open defecation and that the local environment will be repeatedly exposed to pathogens from fecal matter. Environmental exposure to these pathogens will have particularly serious implications for young children as their immune and nervous systems are in the development stage.
4.4. Impact of Open Defecation on SDG 4
The targets of SDG 4 may be jeopardized by infectious diseases. Infectious diseases related to open defecation can affect school attendance. Pearson and McPhedran [27] have concluded that infectious diseases due to open defecation have a greater impact on pre-primary and primary school students and can affect the learning skills of the children.
4.5. Impact of Open Defecation on SDG 5
Target 5.2 of SDG 5 aims to eliminate all types of aggression against women and girls. Caruso et al. [28] have investigated women’s security issues in relation to sanitation and open defecation. Saleem et al. [6] reported that there is an increased risk to women and girls due to the practice of open defecation. Access to safe toilets has a prominent role in defending women’s safety and self-esteem.
4.6. Impact of Open Defecation on SDG 6
Target 6.1 of SDG 6 deals with safe and affordable drinking water. Rajgire [29] has confirmed that open defecation is one of the factors most responsible for water contamination. Open defecation not only deteriorates the quality of water for drinking purpose but also makes it unfit for household use.
Rajgire [29] and Okullo et al. [24] have shown that fecal contamination is a key factor in degrading the quality of water resources. Accumulation of human excreta puts water resources at risk; for example, during flooding, fecal material can be spread to surrounding areas. Dust particles that are blown on the wind are often deposited in water resources and may carry fecal pathogens that lead to contamination [24].
4.7. Impact of Open Defecation on SDG 8
Open defecation affects nations’ overall economic performance by causing: disease and death, loss of productivity due to illness, costs for accessing and treating drinking water, losses in education, and time spent accessing sites for open defecation. Open defecation may affect tourism; tourists may be put off by the unpleasant sight and smell of human excreta. De Francis [19] mentioned that there may be economic losses due to open defecation.
4.8. Impact of Open Defecation on SDG 10
Osumanu et al. [30] have confirmed that open defecation leads to large disparities between rich and poor. Senyk [31] has reported that in countries like India, sewage treatment is done only by the lowest caste. Infectious disease outbreaks may put a nation on the list of high-risk countries and hampers the country’s reputation globally.
4.9. Impact of Open Defecation on SDG 11
The practice of open defecation is minimal in urban areas in comparison to rural areas [31]. Manasi and Latha have found that areas with slums and migrant populations, and with no access to toilets, were predominantly practicing open defecation in an urban city like Bangalore. The area within 50 m of railway tracks acts as a universal commode for open defecation, especially in a country like India. Targets 11.5 and 11.6 deal with economic impacts of water-related disasters, such as urban floods, air quality, and waste management. Urban lands that are filled with human excreta due to open defecation will exacerbate disease outbreaks like cholera during disaster situations such as floods and earthquakes [32,33]. Thus, open defecation in urban areas will hinder achievement of targets aimed to make cities resilient and sustainable.
4.10. Impact of Open Defecation on SDG 14
Targets 14.1 and 14.2 represent issues related to marine pollution of all kinds and to protect the marine and coastal ecosystems. Eutrophication is the process of loading excessive nutrients in the water. Coastal eutrophication has negative effects on marine ecosystems that include algal blooms, increased macro-algae, and increased mortality of fish. Amin et al. [34] have reported that, due to open defecation, rivers contribute to coastal eutrophication. Open defecation may increase the expansion of single-cell microorganisms like Escherichia coli, Vibrio cholerae, Salmonella, and Enterococcus in coastal zones and estuaries. Akankali and Elenwo [35] have stated that aquatic life is reduced in coastal waters if polluted with human waste. Thus, open defecation and untreated human feces influence marine life and hinder efforts that target sustainable marine resources.
4.11. Impact of Open Defecation on SDG 15
Fecal contamination results in increased nutrient loadings to water bodies like lakes, streams, and reservoirs. This process weakens life in aquatic and terrestrial ecosystems. Excessive eutrophication has an adverse effect on biodiversity. Eutrophic algal blooms have a negative impact on the life cycle of fish species and lead to unproductive aquaculture systems. At certain times, eutrophic algal blooms degrade the recreational value of water resorts as they adversely affect the aesthetic appeal [36]. Excessive draining of fecal matter in the aquatic systems leads to a hypoxic dead zone. Low-nutrient ecosystems like peat-lands, meadows, and bogs are often affected by invasive species due to nitrogen and phosphorous from human waste. Fecal contamination gives scope to the spread of pathogens that are harmful to wildlife such as Giardia and Cryptosporidium. Open defecation may amplify the process of zooanthroponosis and thus human diseases can spread to domestic animals that roam and scavenge the shared environment. Soil-transmitted helminthiasis in agriculture zones may degrade the performance of the land due to the presence of hookworms [37]. Thus, the practice of open defecation can adversely affect the ecosystems and cause loss of biodiversity.
5. SANITATION INTERVENTIONS AND ENDING OPEN DEFECATION
The 2030 plan for sustainable development is a chance to review the sanitation practices and curb the habit of open defecation. This would have the benefit of a substantial reduction in fecal–oral-transmitted diseases. Pearson and McPhedran [27] have reported that efforts for sanitation adoption among end users results in improvement of the local environment and this attracts business to the region and benefits the local economy. Based on World Bank estimates, nations have to increases their budget allocation for hygiene and sanitation targets. Hutton et al. [21] have shown that in some low-income countries, investments in the form of sanitation interventions will return benefits that are greater than the amount invested.
Recent UN reports state that >40 countries need to accelerate efforts to end open defecation by 2030; however, on a positive note, 18 countries are already on track to meet the 2030 target for sanitation [38]. Efforts to change the behavior and social norms to end open defecation should be an essential part of the interventions. In Nepal, after years of intensive efforts propelled by UNICEF, the country is in a position to be removed from the list of countries that practice open defecation. Most African countries have introduced and scaled up community-led total sanitation efforts that focus on empowering local communities to end open defecation. The UN Water Global Analysis and Assessment of Sanitation and Drinking Water has reported that countries like Bangladesh, Ethiopia, Pakistan, Rwanda, Ghana, Indonesia, and India have recognized poor sanitation as a source of major health problems, and thus they are moving toward curbing the practice of open defecation using various community-led total sanitation and sanitation interventions [39]. The Swachh Bharat Mission is India’s flagship sanitation intervention that includes systematic involvement of government and nongovernment institutions across all levels. This 5-year project has already started yielding the desired results. Dandabathula et al. [40] have emphasized that there is a sharp decline in acute diarrheal disease outbreaks in India and the success has been attributed to the Swachh Bharat Mission.
6. CONCLUSION
By now, most countries have recognized the harmful effects of open defecation and have initiated sanitation interventions with various collaborations and substantial investments. However, the scale of this target is unprecedently large and can only be achieved by behavioral change at individual and community levels. Faster progress is required to end open defecation in regions like Central–Southern Asia and sub-Saharan Africa as the impact of open defecation will hinder the targets of SDGs.
CONFLICTS OF INTEREST
All listed authors declare no financial support, grants, financial interests or consultancy that could lead to conflicts of interest.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Dandabathula Giribabu AU - Pankaj Bharadwaj AU - Rutvik Sitiraju AU - Mithilesh Burra AU - Peddineni Prasada Rao AU - Chintala Sudhakar Reddy PY - 2019 DA - 2019/07/03 TI - Combating Open Defecation through Community-led Sanitation JO - Dr. Sulaiman Al Habib Medical Journal SP - 45 EP - 51 VL - 1 IS - 3-4 SN - 2590-3349 UR - https://doi.org/10.2991/dsahmj.k.190626.001 DO - 10.2991/dsahmj.k.190626.001 ID - Giribabu2019 ER -