
Could influenza transmission be reduced by restricting mass gatherings? Towards an evidence-based policy framework
- DOI
- 10.1016/j.jegh.2011.06.004How to use a DOI?
- Keywords
- Influenza; Mass gathering; Transmission; Evidence; Policy
- Abstract
Introduction: Mass gatherings (MG) may provide ideal conditions for influenza transmission. The evidence for an association between MG and influenza transmission is reviewed to assess whether restricting MG may reduce transmission.
Methods: Major databases were searched (Pubmed, EMBASE, Scopus, CINAHL), producing 1706 articles that were sifted by title, abstract, and full-text. A narrative approach was adopted for data synthesis.
Results: Twenty-four papers met the inclusion criteria, covering MG of varying sizes and settings, and including 9 observational studies, 10 outbreak reports, 4 event reports, and a quasi-experimental study. There is some evidence that certain types of MG may be associated with increased risk of influenza transmission. MG may also “seed” new strains into an area, and may instigate community transmission in a pandemic. Restricting MGs, in combination with other social distancing interventions, may help reduce transmission, but it was not possible to identify conclusive evidence on the individual effect of MG restriction alone. Evidence suggests that event duration and crowdedness may be the key factors that determine the risk of influenza transmission, and possibly the type of venue (indoor/outdoor).
Conclusion: These factors potentially represent a basis for a policy-making framework for MG restrictions in the event of a severe pandemic.
- Copyright
- © 2011 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
1. Introduction
It is well established that influenza is transmitted from person to person through close contact with an infected, symptomatic individual. The exact mechanisms by which transmission occurs are still unclear, but is believed to involve multiple routes, including respiratory droplets and direct/indirect contact [1] with secretions or fomites. Aerosol transmission may also occur, but controversy surrounds this [2] and some further evidence of aerosol transmission has recently been put forward [3]. This is an important issue as the mechanism of transmission is always a key factor in infection control planning.
While uncertainty persists regarding aerosols, droplet and contact transmission remain largely regarded as the most important and likely routes. Transmission through these routes clearly requires physical nearness to infected persons, via either direct touch or the propulsion of large droplets across a relatively short distance. This requirement makes the consideration of mass gatherings a crucial issue.
Whilst there is not a “standard” definition of what constitutes a mass gathering, there is an understanding that these are events that involve large numbers of people (suggested minimum of 1000 people) [4–6] congregating in finite geographical areas to share an event or experience. Individuals can be in very close proximity for variable periods of time and, if the event is over a number of days, may even share over-crowded and/or temporary accommodation.
Therefore for those infectious diseases such as influenza, where close contact is the main determinant of transmission, it appears self-evident that mass gathering events could lead to the rapid transmission of a new causative agent.
In the event of an influenza pandemic, minimizing transmission of influenza has been a priority for public health action. A variety of non-pharmaceutical public health interventions to reduce close contact between infected and susceptible individuals, or the opportunities for the virus to be picked up by susceptible people such as self-isolation of patients, respiratory etiquette and hand washing have been advocated. Banning or restricting mass gatherings has been seen as a logical extension of this policy, however, it is a particular concern of policy makers that the scientific evidence upon which to base guidance for mass gatherings is lacking. This is particularly important given the need to weigh any potential benefits against the economic and social disruption that banning or restricting mass gatherings could have on society.
There have been other systematic reviews undertaken in recent years on the broader subject of non-pharmaceutical interventions aimed at reducing transmission of respiratory viral infections [7,8]. These reviews considered a range of such interventions, and they explicitly recognized that there is a paucity of primary evidence regarding restriction of mass gatherings (and other “social distancing” measures); thus they did not primarily focus on this specific area.
The aim of this review, therefore, was to attempt to reduce this evidence gap by assessing the available evidence base relating to the utility of restrictions on mass gatherings during an influenza pandemic. This is an important policy area not only because of the impact such restrictions could have on public confidence and morale, but also because of the economic and liability issues that such action might generate. The findings of the review may be able to help inform policy statements on the effectiveness of mass gathering restriction interventions that may be deployed to help reduce influenza virus spread during a pandemic.
2. Methods
The study protocol was largely based on the University of York’s Centre for Reviews and Dissemination guidance for undertaking reviews in healthcare [9]. Work commenced in mid-July 2010 and the main part of it was completed in mid-October 2010. Further work was carried out in June 2011 to bring the literature coverage up to date.
The following specific questions were developed to capture the objectives of the review:
- •
Is there an association between mass gatherings and influenza outbreaks or spread?
- •
Are there any particular characteristics (such as size or duration) of mass gatherings that influence transmission of influenza?
- •
Does the restriction of mass gatherings reduce the spread of influenza within the community (compared with no restriction or with other interventions)?
2.1. Inclusion criteria
The following types of studies were included in the review:
- •
Randomized controlled trial
- •
Quasi-experimental study
- –
Non-randomized controlled study
- –
Before-and-after study
- –
- •
Observational study
- –
Cohort study
- –
Case-control study
- –
- •
Outbreak reports
- –
Outbreak/cluster reports
- –
Historical archival outbreak analyses
- –
- •
Surveillance reports
- –
Major event infection surveillance reports
- –
The list above is largely in hierarchical order of study design quality [9], but with the addition of outbreak and surveillance reports, not traditionally included in such lists, important to the topic of this review. To cover the other “non-standard” study design encountered, the term “quasi-experimental” is employed to describe controlled but non-randomized studies [10,11].
Only studies published in English were included. Relevant systematic and narrative reviews and operational description papers were utilized for useful background information. The reference lists of the systematic reviews were scanned to identify potentially relevant primary studies that could be considered for inclusion. Case reports, mathematical modelling and human/non-human experimental laboratory studies were excluded from the review.
Outcome measures included laboratory-confirmed influenza infection (i.e., documented by virus isolation, molecular testing such as polymerase chain reaction, and serological studies) and clinical influenza-like illness as defined by the investigators, whilst recognizing that this is less specific.
2.2. Search strategy
The search strategy focused on primary studies taking into account the issues detailed above. The term ‘influenza’ rather than ‘pandemic influenza’ was used to reflect the entire spectrum of influenza for which guidance would be relevant. The transmission of other respiratory viruses was also included because of the similarity of transmission and therefore the potential applicability of any results to influenza.
An initial “scoping” search was followed by further discussions and consultation on the work plan and search strategy. The term mass gathering on its own proved inadequate as a search term as there is no clearly accepted definition of what constitutes a mass gathering. Therefore, a range of additional terms were used, such as public gatherings, social gatherings, large crowds, mass events, festivals, Olympics, Hajj, championship, and others listed in Table 1. Transit settings such as long-distance flights and cruise ships were not included, as it was decided that these settings would fit better in a separate review of evidence for influenza transmission through transport. The final search with revised terms and refined using the “advanced search” tool on PubMed was carried out as described in Table 1, with no time period restrictions. The initial searches included the literature up till July 2010. A further search was conducted on 31 May 2011 to bring the literature coverage up to date as part of an editorial process.
| #41 | Search #22) AND #40) |
| #40 | Search #23) OR #24) OR #25) OR #26) OR #27) OR #28) OR #29) OR #30) OR #31) OR #32) OR #33) OR #34) OR #35) OR #36) OR #37) OR #38) OR #39) |
| #39 | Search “world cup” |
| #38 | Search games |
| #37 | Search festival |
| #36 | Search championships |
| #35 | Search Hajj |
| #34 | Search olympics |
| #33 | Search “big event” |
| #32 | Search “mass event” |
| #31 | Search “large event” |
| #30 | Search crowd |
| #29 | Search “large crowd” |
| #28 | Search “public event” |
| #27 | Search “social event” |
| #26 | Search “social gathering” |
| #25 | Search distancing |
| #24 | Search “public gathering” |
| #23 | Search “mass gathering” |
| #22 | Search #1) OR #2) OR #4) OR #5) OR #7) OR #8) OR #11) OR #12) OR #14) OR #15) OR #16) OR #17) OR #18) OR #19) OR #20) OR #21) |
| #21 | Search “respiratory syncytial virus” |
| #20 | Search “parainfluenza virus” |
| #19 | Search “ILI” |
| #18 | Search “flu like” |
| #17 | Search flu-like |
| #16 | Search tuberculosis |
| #15 | Search “acute respiratory tract infection” |
| #14 | Search “acute respiratory infection*” |
| #12 | Search sars |
| #11 | Search “severe acute respiratory syndrome” |
| #8 | Search coronavirus* |
| #7 | Search adenovirus* |
| #5 | Search rhinovirus* |
| #4 | Search “common cold” |
| #2 | Search flu |
| #1 | Search influenza* |
Details of PubMed database search.
In addition, secondary searches were also initially carried out in the following databases: Scopus, Excerpta Medica Database (EMBASE), and the Cumulative Index to Nursing and Allied Health Literature (CINAHL). These are described in Table 2.
| Database | Outcome |
|---|---|
| SCOPUS | 16 Hits; 2 excluded as had been found on PubMed. The remaining 14 were added to the list of titles considered for review |
| Excerpta medica database (EMBASE) | 27 Hits; 24 were excluded as had been found on PubMed. The remaining 3 were added to the list of titles considered for review |
| The cumulative index to nursing and allied health literature (CINAHL) | 6 Hits; 5 were excluded as had been found on PubMed, The last one was also excluded as had been found on EMBASE |
Search terms: flu or influenza or “respiratory infection” or flu-like or “respiratory viruses” AND “mass gatherings” or crowd or “major event” or “large crowd” or “large event” or “big event” or “mass event.”
Searches of additional databases.
2.3. Other sources
In addition to the search results, the reference lists of papers identified from the search were scanned for other potentially relevant studies. Efforts were also made to identify studies other than those published in the peer-reviewed literature; the authors’ hardcopy literature files were hand-searched to identify additional published articles or other documents of relevance.
2.4. Study selection and data extraction
Study selection was conducted in stages. At all stages, scanning and reviews were done independently by the authors, who then harmonized their selections. Papers identified by the searches were scanned and some excluded on the basis of the ‘title’ for relevance to the review. The abstracts of the remaining papers were then reviewed to identify studies that appeared to meet the inclusion criteria. The full text versions of all these articles were then sought and read in full. For papers that had relevant titles but no abstracts, the full text articles were also obtained, scanned for relevance, and if relevant they were read in full. In addition, some papers that did not meet the inclusion criteria (e.g. operational descriptions of interventions, commentaries, or editorial reviews of influenza transmission or pandemic influenza) were selected to provide relevant background or supplemental information.
Data from the selected full text papers were extracted using a pre-designed form. Data elements included publication information, study characteristics, participant characteristics, the intervention (if any) and setting, outcome and results. The data extracted were used to determine the eligibility of each paper for inclusion in the review. This process resulted in a final selection of eligible articles that were then included in the review.
2.5. Temporal and situational context of the review
The main body of this work was undertaken in 2010 by the UK Health Protection Agency as part of a comprehensive influenza scientific evidence review informing the UK National Pandemic Influenza Strategy. Within this context, the work was carried out within a very tight three-month timeframe and with significantly limited resources. As a result, some of the most comprehensive steps required of a full systematic review could not be realistically accommodated. Therefore, a modified process was adopted in conducting this “rapid evidence assessment” rather than a full, formal systematic review. Rapid evidence assessments are well recognized as a pragmatic approach to include all the major elements of a full systematic review, ensuring an outcome that is as comprehensive as possible while accepting limited compromises in order to meet stipulated deadlines for feeding into the policy process [9].
Due to the time constraints, it was not practical to pursue time-intensive contacts with authors or to seek translations for non-English articles, which were therefore excluded. Articles lacking abstracts were largely excluded, and there was a limited search for unpublished studies. However, to try to mitigate these limitations, full draft versions of the review were submitted to national experts at the UK Health Protection Agency and the Scientific Pandemic Influenza committee of the UK Department of Health, seeking their comments and advice on any papers or documents that may have been omitted. Some further work was carried out in May to June 2011 to update the literature.
2.6. Quality assessment
At the outset, a strategy was developed to assess the quality of eligible studies using the Critical Appraisal Skills Programme (CASP) tools as appropriate for each type of study [12]. However, after completion of the literature search, it was clear that the types of studies and the study design types identified were not suitable for assessment by the CASP tools. Similarly for the outbreak reports included in the review, no suitable existing framework could be readily identified for quality assessment. The ORION tool was not strictly applicable as it is specific to outbreaks of nosocomial infection [13,14]. Therefore, a modified approach was adopted, whereby each paper was categorized as having low risk, some risk, or high risk for bias with respect to the relevant review question addressed by that study. The grading was assessed based on the presence of significant methodological limitations. A high risk of bias was attributed to papers with at least three significant methodological issues as identified by the review authors, while papers with at least two issues were classified as having some risk. This approach was adapted from a system previously used by Jefferson et al. [7].
The quality of the review itself was tested against checklists based on the MOOSE [15] and PRISMA [16,17] standards. Within the restrictions of the time constraints already described, key gaps and issues identified by the checklists were addressed as appropriate and/or acknowledged in Sections 2.5 (explaining the review context including time constraints) and 4.4 (recognizing the study limitations).
2.7. Data synthesis
The data synthesis was restricted to a narrative approach that included an analysis of the relationships within and between studies and an overall assessment of the robustness of the evidence and limitations of both the studies and the evidence review [9]. In addition, the synthesis considered the implications for policy and guidance development as well as future research.
3. Results
The search identified a total of 1706 papers after accounting for overlaps between the different databases. These were reviewed on the basis of ‘title’ for relevance to the review (Fig. 1), and on this basis 1593 papers were excluded. Abstracts for the remaining 113 papers were reviewed and a further 54 were eliminated.
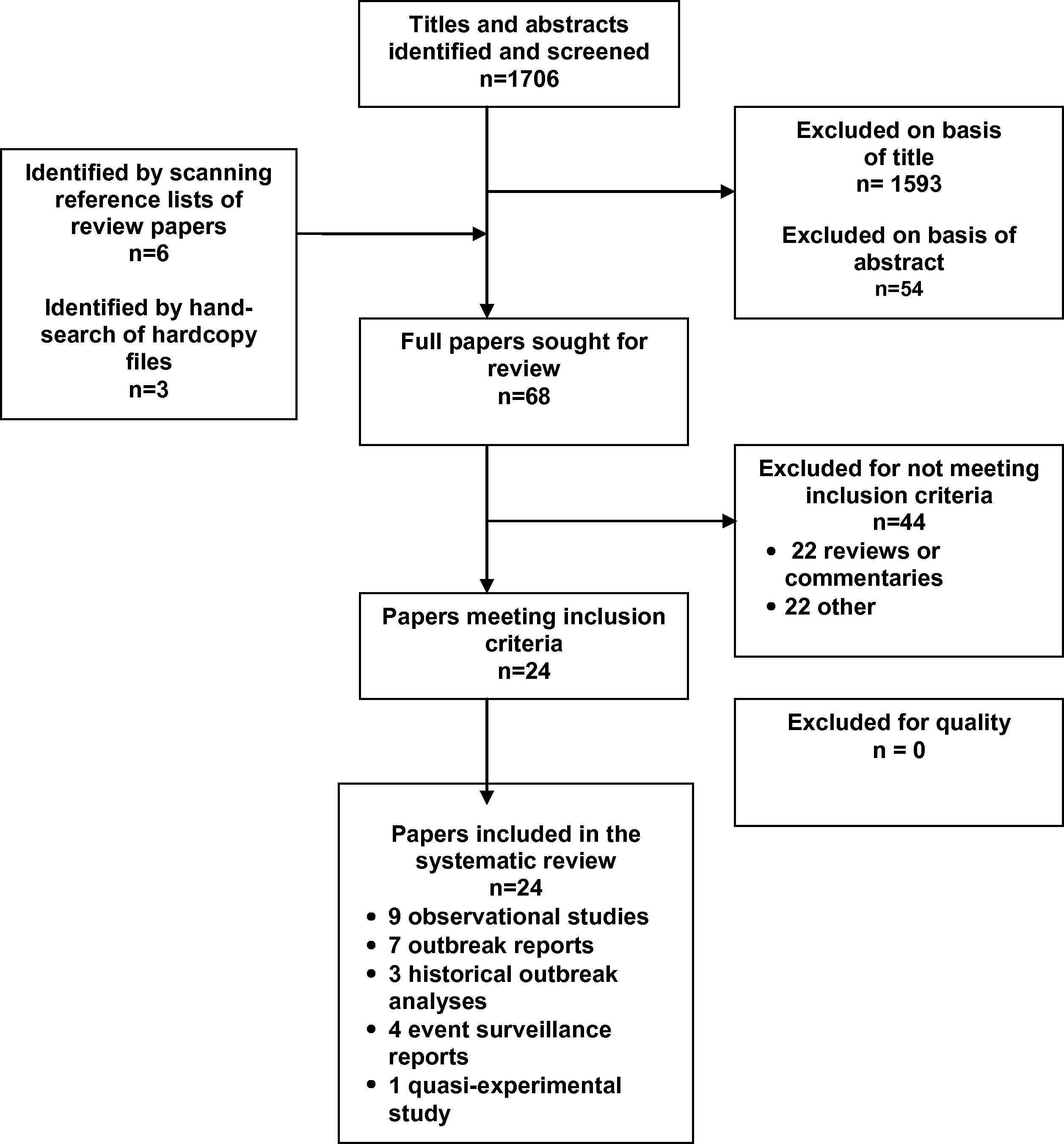
Diagram of search strategy results and article selection.
Full copies of the remaining 59 papers plus 6 papers identified from scanning the reference lists of review papers, and 3 papers retrieved from the authors’ hardcopy files, were reviewed and summarized. Table 3 provides a classification of the 68 papers that were read in full text.
| Type | Total number of papers | Number included in the review |
|---|---|---|
| Quasi-experimental study (non-randomized trial) | 2 | 1 |
| Observational study | 13 | 9 |
| Outbreak report | 8 | 7 |
| Historical outbreak archival data study | 7 | 3 |
| Event surveillance report | 7 | 4 |
| Systematic review | 3 | 0 |
| Narrative review | 6 | 0 |
| Editorial/commentary/statement/opinion | 13 | 0 |
| Background/operational/supplemental information | 9 | 0 |
| Total | 68 | 24 |
Classification of 68 papers read in full, by type of paper.
After full text review, 24 papers were classified as meeting the inclusion criteria. These included a quasi-experimental study (a non-randomized trial) [18], nine observational studies [19–27], seven outbreak reports [28–34], three historical outbreak archive analyses [35–37], and four event surveillance reports [38–41]. Details for each of these studies are summarized in Table 4. The 44 papers that were read but not included in the review are listed in Table 5.
| Investigator (Reference number) | Study design and participants | Reported results | Comments |
|---|---|---|---|
| (A) Quasi-experimental study | |||
| Qureshi et al. [18] | Controlled, non-randomized, open-label (non-blinded) influenza vaccine trial. Vaxigrip (Aventis – Pasteur) was used as a “vaccine probe” to investigate the incidence of vaccine-preventable influenza-like illness (ILI) among Pakistani pilgrims to the Hajj religious gathering in 1999. There were 2070 participants spread across five groups of pilgrims (1120 vaccine group; 950 control group). Participants followed up to record ILI symptoms using daily health status report forms and clinic report forms for those referred to local hospitals during Hajj |
ILI attack rate: Vaccine group 36%; control 62% Vaccine efficacy 38% Vaccine preventable ILI incidence of 22/100 control participants |
Limitations include:
|
| (B) Observational studies | |||
| Deris et al. [20] | A relatively small (n = 387) cross-sectional study of Malaysian pilgrims who had just completed the Hajj. Participants were recruited at the post-Hajj transit center for returning pilgrims. Occurrence of respiratory symptoms was elicited by questionnaire | Almost all participants had at least one respiratory symptom (cough 91.5%). The prevalence of ILI was 40.1%, even though 72% received influenza vaccination before the trip | Limitations include:
|
| Rashid et al. [27] | A cross-sectional comparison of viral respiratory infections between UK and Saudi pilgrims at Hajj 2006. Pilgrims with symptoms of URTI were recruited from a dedicated UK pilgrims’ walk-in clinic service at the event; and a Saudi clinic which mainly served Saudi pilgrims but was open to everyone A total of 260 pilgrims were recruited, having presented with URTI several days after the start of Hajj (infection presumed acquired during the event). They completed questionnaires, and provided nasal swabs for testing by both on-site rapid diagnostic screening (to guide antiviral therapy) and later analysis by real-time RT-PCR |
UK pilgrims: n = 150. 38 (25%) had at least one virus; 17 (11%) had influenza. Saudi pilgrims: n = 110. 14 (13%) had at least 1 virus; 11 (10%) had influenza. There were similar influenza proportions between the two, despite differences in vaccination rates. A risk-group analysis was done to compare those “at-risk” for influenza with those who were not | Laboratory confirmation was a strength of the study Limitations include:
|
| Balkhy et al. [24] | A cross-sectional study of pilgrims from different parts of the world attending the Hajj 2003 event Participants were pilgrims or event workers presenting at dedicated walk-in clinics with URTI on days 10, 11 and 12 of the Hajj (making it likely that infection was acquired during the event) 500 URTI patients who completed questionnaires and had throat swabs were included. 52.8% were males and most participants were in the 20–40 year age group. Swab samples were subjected to viral studies to detect a range of respiratory viruses (inoculation into designated cell lines, followed by immunofluorescence studies) |
54 (10.8%) of the 500 URTI patients tested positive for at least one virus, and a number had multiple infections. Influenza was the most common virus, found in 30 individuals (representing 6% of the total 500 URTI patients) By simple extrapolation of these findings to the total event population of approximately 2 million, it was estimated that at least 400,000 pilgrims would develop URTI, of which 24,000 would have influenza |
A notable strength of the study was that influenza infection was confirmed by viral studies Limitations include:
|
| Rashid et al. [23] | A cross-sectional study estimating the incidence of laboratory-confirmed influenza and RSV infection in British Hajj 2005 pilgrims who developed URTI symptoms. The study also compared a rapid point-of-care diagnostic technique with definitive PCR testing Participants were recruited (a) among pilgrims presenting at designated British Hajj clinics with URTI symptoms; and (b) by visiting several groups of pilgrims in their camps and inviting those with symptoms to participate. Symptoms were documented by questionnaire and clinical examination; and nasal swabs taken |
202 URTI symptomatic persons were tested; 28 (14%) had PCR-confirmed influenza (20 with AH3 strain, 7 with B strain, and 1 with AH1). All presented 4 days or more after reaching the Hajj, suggesting infection during the event. Influenza vaccination was not significantly protective. Nine other persons had RSV infection. There were no complications found on follow-up checks 12 weeks after the Hajj | The use of laboratory confirmation was a strength of the study Limitations include:
|
| Choudhry et al. [19] | Prospective cohort study of ARI incidence among Riyadh residents attending the 2002 Hajj in Mecca, Saudi Arabia. Pre-Hajj questionnaire administered at recruitment at travel vaccine clinics. Post-Hajj telephone interviews were used to collect data on ARI incidence | Of 1027 participants, 39.8% developed ARI during or within two weeks of Hajj. Older subjects and those with underlying disease (diabetes) were more at risk. Stay at Hajj area for 5 days or more was associated with increased risk of ARI | Limitations include:
|
| Gautret et al. [26] | An observational study of French pilgrims in the 2009 Hajj. The study primarily focused on the influence of preventive measures on the occurrence of influenza in these pilgrims 405 intending French pilgrims were recruited from pre-Hajj mandatory meningococcal vaccination clinics; 247 people who completed a post-Hajj telephone questionnaire were included in the study. The mean age was 58 years and the male:female ratio was 1:1. The use of a range of preventive measures was recorded |
22 participants (8% of 247) had ILI, defined as a triad of cough, sore throat and fever. Cough was the most common respiratory symptom found (48.5% of participants) The use of preventive measures including vaccination and face masks did not significantly reduce symptoms |
Limitations include:
|
| El Bashir et al. [25] | Influenza serological study of a cohort of UK pilgrims attending the 2003 Hajj. Participants were recruited among worshippers at a single mosque in East London who intended to attend the Hajj. Venous blood samples and questionnaires were completed before and within 2–3 weeks after the Hajj; 115 participants were enrolled Haemagglutination inhibition tests were used for laboratory assessment, with influenza diagnosis based on seroconversion defined as at least fourfold antibody titre rise |
44 (38%) of the pilgrims developed influenza (based on seroconversion). A total of 93 (81%) had symptoms of respiratory infection. Vaccination did not seem to be significantly protective | A small but useful study that was strengthened by laboratory testing for influenza Limitations include:
|
| Gautret et al. [22] | Prospective cohort study of French pilgrims attending 2006 Hajj, assessing influence of statin on febrile cough incidence; 580 subjects were recruited at pre-travel clinic facility; 10.3% were taking statin for hypercholesterol; 34.3% had influenza vaccine; 43% had an underlying chronic disease. A post-Hajj questionnaire was used to collect data on health problems faced during the trip | 447 participants responded. High attack rate of cough episodes (60.6% overall). In all, 13.9% had both cough and fever. Neither influenza vaccine nor statin use were protective | Limitations include:
|
| Gautret, et al. [21] | Prospective cohort study of travel-associated health problems in French pilgrims attending 2007 Hajj. 545 subjects were recruited at pre-travel clinic facility. All had influenza vaccine. A post-Hajj questionnaire was used to collect data on health problems faced during the trip | 462 participants responded. 58.9% had at least one health problem; 2.8% were hospitalized. Cough was the commonest symptom overall (51%) – about a fifth of these (overall 9%) had fever and cough; the risk of this increased with age | Limitations:
|
| (C) Outbreak reports | |||
| Pang et al. [32] | An overview report of the 2003 SARS outbreak in Beijing, China, with 2521 probable cases reported over a 3-month period from March to May, and 7.6% case fatality rate The authors also reported the control measures taken by health authorities against the outbreak. They analysed the timeline of response measures against the epidemiological progression of the outbreak, attempting to identify which control measures were the most effective |
A range of medical, physical and social control measures were taken at different time points Among these was the closure of public entertainment sites, such as theatres and indoor sports facilities. Authors concluded that control of the outbreak was achieved through a combination of factors |
As mass gatherings restriction was only part of a battery of interventions, it is hard to make out the individual effect of restrictions |
| Saenz et al. [33] | Influenza outbreak report from a medical congress held in Teheran on September 7–15, 1968. Background: The A2/Hong Kong/68 virus caused a series of outbreaks across several Asian countries in 1968, but had not been found in Teheran prior to this congress Description: during the congress, many participants developed symptoms and one of them started an investigation. Questionnaires were later sent to all 1036 participants from 82 countries on all continents. 844 responded |
304 of 844 respondents fulfilled criteria for influenza, with a final attack rate of 36%. Illness was mostly mild; more marked and prolonged in those aged >55 years; 50 respondents returned to their home countries with fever, of which 36% were believed to have spread infection to contacts, but no large local foci developed | This was a well-reported outbreak. Surprisingly, serological test results were not reported even though samples were said to have been taken. Also, information on the numbers of cases in contacts of participants was not provided |
| Gutierrez et al. [30] | Influenza outbreak report at the “Rock Werchter” musical festival in Belgium, July 2–5, 2009, during the 2009 A(H1N1) pandemic. The event involved 113,000 participants | 30 event-linked ILI cases, with 12 confirmed A(H1N1). There were no hospital admissions; mean age 23 (range 18–45) years. The index case was identified as an Israeli participant who arrived in Belgium via London, became ill on July 3 (day after arrival) and presented to festival clinic on July 5. The median generation interval for secondary cases was estimated to be 4 (range 3–7) days. Later, two further event-linked confirmed cases were found in the Netherlands and Luxembourg. The outbreak prompted a national shift to a mitigation strategy in Belgium as it was assessed that community transmission had started | There was likely under-reporting as there was no active case-finding at the festival site. However, there was considerable national mass media and Internet publicity about the cases |
| Loncarevic et al. [31] | Influenza outbreak reports at two large events held in Serbia in July 2009, during the 2009 pandemic. Prior to the events, 20 cases of H1N1 influenza had been noted. The events were: (i) The 25th Universiade – World University Games, July 1–12, involving 8600 athletes, 15,000 volunteers and staff, and 500,000 spectators; on 53 sites in 9 locations; (ii) the 10th EXIT music festival, July 9–12; involving 190,000 visitors to an open-air, multi-stage festival. There was an enhanced daily surveillance system for both events | (i) Universiade: 7 confirmed cases (4 believed linked to the Games). (ii) EXIT festival: 62 confirmed cases (47 linked to event); mostly aged 16–30 years, and all mild. A further 32 probable cases linked to the festival occurred after it ended, but not confirmed due to a change in testing policy. There were no complications or deaths | Cases may have been under-reported due to asymptomatic cases or non-presenters |
| Botelho-Nevers et al. [29] | Influenza cluster and unusual case report, linked with the Sziget rock festival in Budapest, August 11–18 2009. The event involved 390,000 participants. This was during the 2009 A(H1N1) pandemic, thus a dedicated flu medical tent was set up and the local hospital placed on stand-by | 14 people were hospitalized (3.6/100,000); 8 were confirmed PCR positive for A(H1N1) (57.1%). Background activity at the time in Hungary was ILI 7.8/100,000; and across Europe (ECDC) it was 34.9/100,000 with 15.3% A(H1N1) positivity Surveillance through EuroTravNet revealed no other cases in participants returning to other European nations The unusual case was a 23-year-old French male participant who had dual infection with A(H1N1) and varicella zoster virus. He was hospitalized in France and had a good outcome |
ILI rates were lower at the festival than the national and continental rates; however the A(H1N1) positivity was much higher than the European population rate; together possibly suggesting that many mild cases may not have presented in clinic |
| Zepeda-Lopez et al. [34] | An analysis of the 2009 A(H1N1) outbreak in Mexico. The paper described the clinical features seen in a series of confirmed cases Different epidemiological resources were used to map the spread of the virus throughout the country, including the Mexican SINAVE surveillance system and official reports from the Mexican Secretariat of Health |
202 of 751 suspected cases were confirmed infected with the novel 2009 pandemic A(H1N1) virus Two likely key contributory factors to influenza spread were noted: (i) high population density, and (ii) a mass gathering involving over 2 million people, held in Iztapalapa, Mexico City at an early stage of the outbreak |
An innovative study using various sources of information to determine the temporal-spatial dynamics of influenza transmission |
| Blyth et al. [28] | Report of influenza outbreak during the World Youth Day events in Sydney, July 15–20, 2008. This was a time of low local seasonal influenza activity, but near the onset of Australian influenza season. The largest of the series of religious events was a Papal Mass with a crowd of 400,000. The first influenza case was noted on July 16 and flu clinics were rapidly set up and symptomatic people encouraged to attend. They had paired nose and throat swabs taken and detailed virological serotyping carried out | 100 of 227 symptomatic people who voluntarily attended clinics had laboratory-confirmed influenza (a range of A and B types). Local influenza activity increased in the weeks following the event, with evidence of introduction of novel influenza viruses | The outbreak response was well-organized, resourced and reported. Data collection was not standardized as numerous clinicians manned the rapidly set-up clinics. The true extent of the outbreak is unknown. Also, as the event was held near the onset of the usual Australian influenza season, the post-event increase in flu activity may have occurred regardless |
| (D) Historical outbreak studies | |||
| Markel et al. [37] | Historical archival outbreak analysis research Setting: 1918–1919 influenza pandemic. This study examined detailed records of the period September 8, 1918 to February 22, 1919, analysing the public health responses of American cities to the pandemic; 43 American cities (all with a population at the time exceeding 100,000) and for which the most extensive records of Public Health interventions could be found, were studied. The sources of information included the period “Weekly Health Index” of the U.S. Census Bureau, official public health reports, media archives, and municipal records |
Three main categories of non-phamaceutical interventions (NPI) were applied: (a) school closures; (b) isolation and quarantine; and (c) public gathering bans (which included closing salons, sports events, entertainment venues, and some indoor gatherings). Most cities implemented a combination of these interventions, most commonly combining public gathering bans and school closures A total of 143,000 excess pneumonia and influenza deaths occurred in the 43 cities during the period studied. In general, early and sustained NPI implementation was significantly beneficial. Cities with earlier NPI reached peak mortality later and had lower peak and total mortality. Sustained and lengthier NPI implementation was associated with lower excess mortality |
The major strength of the study was to link archived data with modern techniques to produce research that is useful at this time The limitations are similar to those of Hatchett et al.[36] below |
| Hatchett et al. [36] | Historical archival outbreak analysis research Setting: 1918 influenza pandemic. This study examined detailed records of the period September 8 to December 28, 1918, focusing on the public health responses of American cities to the pandemic; 17 American cities for which complete records of Public Health interventions could be found, were studied. The sources of information included newspaper archives, municipal records, and consultations with current officials |
19 Categories of NPIs were identified. The measures of epidemic outcome included the peak death rate, and a “normalized” peak that was standardized to facilitate inter-city comparison. Among the findings were that:
|
A real strength of the study is that it combines archived data with modern techniques to produce potentially very valuable data. This allows an evaluation of an experimental situation that is very difficult to simulate as a contemporary intervention study. Limitations include:
|
| Aimone [35] | A historical examination of the response of New York City (NYC) authorities to the 1918 pandemic influenza | NYC took a number of public health actions, particularly to reduce rush-hour crowding. There were no formal closures of theatres or schools. Yet, the excess death rate due to pandemic in NYC was comparable or lower than in some other major U.S. cities | |
| (E) Event surveillance reports | |||
| Gundlapalli et al. [38] | Prospective influenza surveillance report from the Winter Olympiad, February and March 2002. Components of the surveillance program included: screening of athletes and non-athletes with respiratory symptoms; daily review of viral testing and community public health reports; and case treatment and contact prophylaxis | 2635 medical visits reported during the Games; 12% with respiratory symptoms. Three main clusters of ILI: (a) 13-man team of security staff with 3 confirmed cases; (b) a 12-member national team with 2 confirmed; (c) 8 participants of the same sport, with 5 confirmed. Overall, 188 people were screened for influenza; 36 were positive (28 type A and 8 type B). Syndromic definition of ILI (fever and cough or sore throat) was not highly predictive of confirmed influenza (sensitivity 67% and specificity 78%) | This was a well-organized systematic prospective influenza surveillance program, described by the authors as the first of its type at a large Games event Limitations include:
|
| Demicheli et al. [41] | Prospective influenza surveillance report from the Winter Olympics in Torino, Italy, February and March 2006. Components of the surveillance program included: statutory notification of infectious diseases, laboratory-based surveillance of invasive diseases, sentinel surveillance of influenza-like illness, syndromic surveillance, and toxic exposure surveillance | GP-based daily reporting of ILI showed that there was no increased ILI activity throughout the period. In fact, ILI activity was less than for the corresponding period of the previous year | Well-organized systematic prospective influenza surveillance program The report was quite brief and rather short on details |
| Lim et al. [39] | Influenza surveillance report during the disease containment phase of the 2009 A(H1N1) pandemic. More than 600 confirmed cases had occurred in Singapore prior to the Games Asian Youth Games in Singapore, June 29 to July 7, 2009 (football preliminaries started on June 20). The Games involved 9 sports at 10 venues; 1210 athletes; and 810 officials all from 43 different countries |
66 suspected cases identified at the Games medical facility; 6 confirmed and isolated in hospital. By contact tracing, 42 persons were quarantined. There was no evidence of A(H1N1) transmission associated with the Games | This was a detailed operational description and surveillance report The authors stated that no transmission took place during the Games; but it is unclear how the 6 confirmed cases were infected – possibly imported cases? |
| Schenkel et al. [40] | Infectious disease surveillance report; World Cup 2006, Germany, June 9 – July 9, 2006. There was an extensive enhanced national surveillance system built around the event, based on existing national and local systems | No respiratory events of public health relevance were reported. Infection incidents reported were (a) single cases of varicella, mumps, and S.enteritides; (b) a suspected viral gastroenteritis outbreak; and (c) a confirmed norovirus outbreak | It is not specifically stated that respiratory infections were under surveillance, but the authors stated that the system was set up “to detect adverse health events of public health relevance” – presumably including respiratory infections |
Abbreviations used: ARI = acute respiratory tract infection; ILI = influenza-like illness; NPI = non-pharmaceutical interventions; PCR = polymerase chain reaction; RSV = respiratory syncytial virus; URTI = upper respiratory tract infection.
Synopsis of studies included in the final review.
| Paper citation | Brief notes |
|---|---|
| Editorials, expert statements, and similar papers | |
| Anonymous. Hajj and 2009 pandemic influenza A H1N1. Lancet 2009;374:1724 | Editorial |
| Anonymous. Human infection with new influenza A (H1N1) virus: WHO Consultation on suspension of classes and restriction of mass gatherings to mitigate the impact of epidemics caused by influenza A (H1N1), May 2009. Wkly Epidemiol Rec 2009;84(27):269–71 | WHO technical consultation report |
| Dixon B. Mass gathering: mass effect? Lancet Infect Dis 2010;10:662 | Expert opinion/reflection |
| Ebrahim SH, Memish ZA, Uyeki TM, Khoja TA, Marano N, McNabb SJ. Public health. Pandemic H1N1 and the 2009 Hajj. Science. 2009;13;326(5955):938–40. Epub 2009 Oct 29 | Expert opinion/policy paper |
| Ferguson N, Nicoll A, Schwartz B. SIP 5: Social distancing during a pandemic. Not sexy, but sometimes effective: social distancing and non-pharmaceutical interventions. Vaccine 2009;23;27(45):6383–6 | Discussion paper on social distancing |
| Franco-Paredes C, Carrasco P, Preciado JI. The first influenza pandemic in the new millennium: lessons learned hitherto for current control efforts and overall pandemic preparedness. J Immune Based Ther Vaccines 2009;7:2 | Expert commentary |
| Gatrad AR, Shafi S, Memish ZA, Sheikh A. Hajj and the risk of influenza. BMJ 2006;333:1182–3 | Expert opinion |
| Gautret P, Parola P, Brouqui P. Risk factors for H1N1 influenza complications in 2009 Hajj pilgrims. Lancet 2010;375:199–200 | Letter and opinion |
| Haworth E, Rashid H, Booy R. Prevention of pandemic influenza after mass gatherings – learning from Hajj. J R Soc Med 2010;103(3):79–80 | Editorial |
| Memish ZA, Ebrahim SH, Ahmed QA, Deming M, Assiri A (letter). Pandemic H1N1 influenza at the 2009 Hajj: understanding the unexpectedly low H1N1 burden. J R Soc Med 2010;103:386 | Expert commentary |
| Rashid H, Haworth E, Shafi S, Memish ZA, Booy R. Pandemic influenza: mass gatherings and mass infection. Lancet Infect Dis. 2008;8(9):526–7. Epub 2008 Aug 4 | Expert opinion/reflection |
| Tomes N. “Destroyer and teacher”: Managing the masses during the 1918–1919 influenza pandemic. Public Health Rep 2010;125 (Suppl. 3):48–62 | Discussion paper on the 1918–1919 influenza pandemic |
| WHO. Health conditions for travellers to Saudi Arabia for the pilgrimage to Mecca (Hajj). Wkly Epidemiol Rec 2010;22;85(43):425–8 | WHO travel recommendations |
| Narrative reviews | |
| Ahmed QA, Arabi YM, Memish ZA. Health risks at the Hajj. Lancet 2006;367(9515):1008–15 | Narrative review paper |
| Michael JA, Barbera JA. Mass gathering medical care: a twenty-five year review. Prehosp Disaster Med 1997;12(4):305–12 | Narrative review paper |
| Milsten AM, Maguire BJ, Bissell RA, Seaman KG. Mass-gathering medical care: a review of the literature. Prehosp Disaster Med 2002;17(3):151–62 | Narrative review paper |
| Oshitani H. Potential benefits and limitations of various strategies to mitigate the impact of an influenza pandemic. J Infect Chemother 2006;12(4):167–71 | Narrative review paper |
| World Health Organisation Writing Group. Non-pharmaceutical interventions for pandemic influenza, national and community measures. Emerging Infectious Diseases 2006;12:88–94 | WHO recommendations on non-pharmaceutical interventions |
| Zieliński A. Evidence for excessive incidence of infectious diseases at mass gatherings with special reference to sporting events. Przegl Epidemiol 2009;63(3):343–51 | Narrative review paper |
| Systematic reviews | |
| Aledort JE, Lurie N, Wasserman J, Bozzette SA. Non-pharmaceutical public health interventions for pandemic influenza: an evaluation of the evidence base. BMC Public Health 2007;15(7):208 | Systematic review and expert panel |
| Jefferson T, Del Mar C, Dooley L, Ferroni E, Al-Ansary LA, Bawazeer GA, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses: systematic review. BMJ 2009;21(339):b3675. doi:10.1136/bmj.b3675 | Systematic review |
| Jefferson T, Del Mar C, Dooley L, Ferroni E, Al-Ansary LA, Bawazeer GA, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database Syst Rev. 2010;2(1):CD006207 | Systematic review (Cochrane) |
| Observational studies | |
| Al-Asmary S, Al-Shehri AS, Abou-Zeid A, Abdel-Fattah M, Hifnawy T, El-Said T. Acute respiratory tract infections among Hajj medical mission personnel, Saudi Arabia. Int J Infect Dis 2007;11(3):268–72. Epub 2006 Aug 14 | Observational study of the occupational risk of influenza in healthcare facility workers at the Hajj mass gathering |
| Baum NM, Jacobson PD, Goold SD. “Listen to the people”: public deliberation about social distancing measures in a pandemic. Am J Bioeth 2009;9(11):4–14 | Cross-sectional study from Michigan – focus group discussions on attitudes towards social distancing |
| Broderick MP, Hansen CJ, Russell KL. Exploration of the effectiveness of social distancing on respiratory pathogen transmission implicates environmental contributions. J Infect Dis 2008 Nov 15;198(10):1420–6 | Non-randomized controlled social distancing intervention study in a community setting; not applicable to a mass gathering situation |
| Deris ZZ, Hasan H, Ab. Wahab MS, Sulaiman SA, Naing NN, Othman NH. The association between pre-morbid conditions and respiratory tract manifestations amongst Malaysian Hajj pilgrims. Trop Biomed 2010;27:294–300 | This paper presents further data analysis from an observational study that is already included in this review [20] |
| Eastwood K, Durrheim DN, Butler M. Responses to pandemic (H1N1) 2009, Australia. A. Emerg Infect Dis 2010;16(8):1211–6 | A follow-up cross-sectional survey on willingness to comply with potential health interventions during a pandemic |
| Hutton A, Roderick A, Munt R. Lessons learned at World Youth Day: collecting data and using postcards at mass gatherings. Prehosp Disaster Med 2010;25(3):273–7 | Cross-sectional methodological study on data collection at mass gatherings |
| Rubin GJ, Amlôt R, Page L, Wessely S. Public perceptions, anxiety, and behaviour change in relation to the swine flu outbreak: cross-sectional telephone survey. BMJ 2009;2(339):b2651. doi:10.1136/bmj.b2651 | Cross-sectional study of swine flu-related public perceptions |
| Outbreak report | |
| Witkop CT, Duffy MR, Macias EA, Gibbons TF, Escobar JD, Burwell KN, et al. Novel Influenza A (H1N1) outbreak at the U.S. Air Force Academy: epidemiology and viral shedding duration. Am J Prev Med 2010;38(2):121–6. Epub 2009 Oct 21 | Outbreak report from a training academy |
| Historical analyses | |
| Caley P, Philp DJ, McCracken K. Quantifying social distancing arising from pandemic influenza. J R Soc Interface. 2008 Jun 6;5(23):631–9 | Modeling-based historical outbreak analysis of social distancing during the 1918–1919 pandemic |
| McSweeny K, Colman A, Fancourt N, Parnell M, Stantiall S, Rice G, et al.. Was rurality protective in the 1918 influenza pandemic in New Zealand? N Z Med J. 2007 Jun 15;120(1256):U2579 | Historical analysis of the effect of residential location on mortality during the 1918 influenza pandemic |
| Nishiura H, Chowell G. Household and community transmission of the Asian influenza A (H2N2) and influenza B viruses in 1957 and 1961. Southeast Asian J Trop Med Public Health 2007 Nov;38(6):1075–83 | Historical outbreak analysis of community setting transmission during the 1957 pandemic and the 1961 epidemic |
| Wallinga J, van Boven M, Lipsitch M. Optimizing infectious disease interventions during an emerging epidemic. Proc Natl Acad Sci USA 2010;107(2):923–8. Epub 2009 Dec 28 | Vaccine-focused historical study of interventions during the 1957–1958 influenza epidemic |
| Event surveillance | |
| Coletta M, Dewey L, White-Russell M, Powell T, Toney D, Cheek J, et al. Surveillance for early detection of disease outbreaks at an outdoor mass gathering – Virginia, 2005. MMWR Weekly 2006;55:71–74 | Brief description and report of surveillance for a mass gathering event in Virginia. Insufficient information regarding the syndromic surveillance system used |
| Giorgi Rossi P, Sangalli M, Faustini A, Forestiere F, Perucci CA. Infectious diseases in Rome during the Millennium Year. Euro Surveill 2003;8(9):181–5 | Brief description and report of surveillance activities for the Millennium Year event in Rome. Respiratory virus infections were not among the target diseases for enhanced surveillance |
| Gonçalves G, Castro L, Correia AM, Queirós L. Infectious diseases surveillance activities in the north of Portugal, during the EURO 2004 football tournament. Euro Surveill 200;10(4):86–9 | Description and report of surveillance activities for the Euro 2004 football event in Portugal. Respiratory virus infections were not among the target diseases for enhanced surveillance |
| Other types of studies | |
| Avery JG, Chitnis JG, Daly PJ, Pollock GT. Medical planning for a major event: the Pope’s visit to Coventry Airport, 30 May 1982. Br Med J (Clin Res Ed). 1982 Jul 3;285(6334):51–3 | Operational medical response to a mass gathering event |
| Barr AC, Lau RC, Ng NW, da Silva MA, Baptista M, Oliveira VF, et al. What would you do? Managing a metro network during mass crowd events. J Bus Contin Emer Plan 2010;4(2):174–80 | Operational paper on transport issues related to mass gatherings |
| Fizzell J, Armstrong PK. Blessings in disguise: public health emergency preparedness for World Youth Day 2008. Med J Aust 2008;189(11–12):633–6 | Description of planning and response to a mass gathering event |
| López-Cervantes M, Venado A, Moreno A, Pacheco-Domínguez RL, Ortega-Pierres G. On the spread of the novel influenza A (H1N1) virus in Mexico. J Infect Dev Ctries 2009;3(5):327–30 | Background information on the 2009 A(H1N1) outbreak in Mexico |
| Markel H, Stern AM, Cetron MS, Theodore E. Woodward award: non-pharmaceutical interventions employed by major American cities during the 1918–1919 influenza pandemic. Trans Am Clin Climatol Assoc 2008;119:129–38; discussion 138–42 | Presentation and discussion paper on data from the 1918–1919 influenza pandemic. The substantial research report arising from the study was included in the study [37] |
| Memish ZA, McNabb SJ, Mahoney F, Alrabiah F, Marano N, Ahmed QA, et al. Jeddah Hajj Consultancy Group. Establishment of public health security in Saudi Arabia for the 2009 Hajj in response to pandemic influenza A H1N1. Lancet 2009;374(9703):1786–91. Epub 2009 Nov 14 | Consultation and recommendations on public health planning and response for the Hajj 2009 |
| Poggensee G, Gilsdorf A, Buda S, Eckmanns T, Claus H, Altmann D; RKI Working Group Pandemic Influenza, Krause G, Haas W. The first wave of pandemic influenza (H1N1) 2009 in Germany: from initiation to acceleration. BMC Infect Dis 2010;10:155 | Epidemiological description – initial period of the 2009 H1N1 outbreak in Germany |
| van Hal SJ, Foo H, Blyth CC, McPhie K, Armstrong P, Sintchenko V, et al. Influenza outbreak during Sydney World Youth Day 2008: the utility of laboratory testing and case definitions on mass gathering outbreak containment. PLoS One 2009;3;4(9):e6620 | An analysis of epidemic testing strategies |
Excluded papers. This is a summary list of the 44 articles that were excluded after full text review as they did not meet the inclusion criteria.
3.1. Quasi-experimental study
One quasi-experimental study by Qureshi et al. [18] attempted to investigate the incidence of vaccine preventable influenza-like illness among Pakistani pilgrims to the Hajj religious gathering in 1999. The Hajj is an annual religious event that takes place over a number of days in a very small geographic area of Saudi Arabia usually involving 2 to 3 million pilgrims from all over the world. Accommodation is at a premium during this event and many pilgrims stay in tents specifically erected for the event and that are often over-crowded. Although primarily a vaccine efficacy study, the rates of influenza-like illness reported in vaccinated pilgrims were 36% compared with 62% in non-vaccinated pilgrims. However, these results were based on clinical endpoints without microbiologic confirmation; a non-randomized design was used, and the study was not designed to address the primary question of this review.
3.2. Observational studies
Nine observational studies estimated the risk of acute respiratory illness and/or influenza-like illness associated with the Hajj pilgrimage by attempting to measure its occurrence in pilgrims. Four [23–25,27] of these studies confirmed the cause of illness by laboratory testing, while the other five relied on specified symptom complexes as surrogate indicators.
Among the nine observational studies were four cross-sectional studies. Balkhy and colleagues [24] tested 500 Hajj pilgrims in 2003 who presented with symptoms of upper respiratory tract infection in the second week of the event; 30 (6%) of the 500 pilgrims tested positive for influenza. Rashid et al. [23] assessed the burden of laboratory-confirmed influenza and respiratory syncytial virus (RSV) infections in symptomatic British Hajj pilgrims in the 2005 event. Of 202 symptomatic pilgrims who underwent nasal swab testing, 28 (about 14%) had confirmed influenza (mostly A type), while only 9 (4%) had RSV infection. In the 2006 Hajj, the same investigators [27] found comparable levels of laboratory confirmed influenza (10–11%) in both UK and Saudi pilgrims. These relatively low levels of infection contrasted with the findings in the cross-sectional study by Deris et al. [20] who based their assessment on syndromic influenza-like illness rather than laboratory-confirmed infection. They found an influenza-like illness prevalence of 40% in Malaysian pilgrims who had just completed the Hajj.
The other five observational studies were similarly designed, involving groups of intending Hajj pilgrims who were recruited in their home regions or countries prior to the event, and then re-assessed after the pilgrimage. Even though three reports were described by their respective authors as “prospective cohort” studies [19,21,22], none of these five studies included an “unexposed” (non-Hajj attending) control group for comparison, indicating that they should be more accurately regarded as “before and after” studies. Choudhry et al. [19] assessed Saudi residents (attending the Hajj from a different part of the country) and found an incidence of influenza-like illness of about 40%. Three studies of French pilgrims by Gautret et al. [21,22,26] found rates of cough of between 48% and 61%; while in El-Bashir and colleagues’ serological study of UK pilgrims [25], respiratory symptoms occurred in more than 80%, but the seroconversion rate was 38% of 115 participants.
These variable data underline the difficulties of comparing different studies that employ contrasting measures of influenza. Interpretation needs to take account of the fact that studies using clinical outcomes suggest much higher levels of influenza-like conditions than the ones that involve laboratory confirmation. Even among the laboratory-based studies, differences in laboratory techniques may also be significant.
3.3. Outbreak reports
There were four types of outbreaks in the reports that were reviewed. The first of those was a paper by Pang et al. [32] that described the experience of dealing with the SARS (severe acute respiratory syndrome) outbreak of 2003 in Beijing and attempted to evaluate the control measures that were deployed. However, there was no reliable indication of the impact of mass gathering restrictions on controlling the outbreak as mass gatherings were grouped together with a number of measures loosely described as social distancing.
The next group consists of four reports of influenza outbreaks occurring at a religious event in Australia and at three large, open-air music festivals in Europe. All of the events lasted several days and involved crowds ranging from 100,000 to 400,000 people. It is particularly relevant that the three music festivals occurred during the 2009 influenza pandemic—two at the beginning and one later during the pandemic.
The report by Blyth et al. [28] described an outbreak of influenza at a large, 5-day religious event in Australia during July 2008 attended by over 400,000 participants from 170 countries. Over 100,000 of the pilgrims were accommodated in a variety of make-shift, overcrowded venues such as sports halls, community centers and schools. One hundred laboratory-confirmed cases of influenza were identified among attendees. Seven different strains of influenza were identified (four influenza A and three influenza B), highlighting the potential for the introduction of novel influenza strains.
Loncarevic et al. [31] described an outbreak of influenza at a 4-day music festival in Serbia during July 2009 involving over 190,000 participants, with a number of them coming from other European countries. Many of the participants stayed at a large campsite where overcrowding was an issue. Sixty-two laboratory-confirmed cases of H1N1 (2009) were identified; some of which were secondary cases. Although the virus was already present in Serbia at the time of the festival, the sudden increase in cases, in particular the secondary cases associated with the festival, suggests possible local spreading. The authors also reported on a small outbreak of influenza at an international sporting event held in Serbia in July over a period of 12 days and attended by over 500,000 spectators. Seven confirmed cases of H1N1 (2009) were identified in six athletes and a volunteer helping at the games. Although a much larger event, the numbers affected are considerably smaller and seem to be restricted to participants rather than those attending.
Gutierrez et al. [30] described a 4-day music festival in Belgium during early July 2009 attended by an estimated 120,000 people from all over Europe. Twelve laboratory-confirmed cases of H1N1 (2009) were identified. Although sporadic cases of H1N1 (2009) had been detected in Belgium prior to the festival, an increase in cases was observed after the event and the decision to shift to mitigation was taken almost a week after the first festival-associated cases were identified. The authors suggest that this festival highlights the potential seeding role for these events in the early stages of a pandemic.
Botelho-Nevers et al. [29] depict an outbreak of influenza at a 7-day music festival in Hungary during August 2009 attended by 390,000 people from all over Europe. Many of the participants were located on a campsite set up for the festival. Eight laboratory-confirmed cases of H1N1 (2009) were identified. Cases of pandemic influenza had already been identified in Hungary and at the time the community influenza-like illness rate was 7.8 per 100,000 against an estimated 3.6 per 100,000 at the music festival.
The third type of outbreak report described by Saenz et al. [33] involved a large, international medical conference held in Iran during September 1968 at the early stages of the 1968/1969 pandemic. The 7-day conference was attended by over 1000 participants from all over the world. It was estimated that about a third of the participants developed an influenza-like illness with an overall attack rate of 36%. The virus was isolated from throat and nasal washings; this was found to be the pandemic A/Hong Kong/68 virus. There was evidence that close contacts of returning attendees were also affected, but none of the episodes led to a rapidly expanding focus of infection. The high attack rate raises the question of whether the indoor setting may represent a particularly high risk.
Lastly, there was an innovative study examining the 2009 A(H1N1) outbreak in Mexico [34]. The authors described the details of 202 cases and then used a series of epidemiological tools to map the spread of the virus throughout the country. They identified two major contributory factors to the rapid spread of influenza: one was the very high population density in parts of Mexico City; the other was the massive religious festival involving more than 2 million people, which took place in the city’s Iztapalapa neighbourhood at the very early stage of the outbreak, shortly before the new virus was identified. It is suggested by the authors that this temporal association between the mass gathering event and the subsequent increase in numbers of cases may reflect participants returning to their own neighbourhoods across the city, and from there to other parts of the country.
3.4. Historical outbreak analyses
Inevitably for a subject of research such as mass gathering restrictions, where prospective studies present serious practical challenges, researchers have sought to utilize historical data to try to draw out major lessons for current impact. This review included three historical analyses of the non-pharmaceutical responses to the 1918–1919 influenza pandemic.
Markel et al. [37] examined the variety of non-pharmaceutical interventions that were deployed in 43 American cities during the 1918–1919 influenza pandemic. The combination of school closures and concurrent public gathering bans was implemented in 34 (79%) of the 43 cities and was the commonest combination of measures deployed. Applied early in the pandemic, this combination was significantly associated with reductions in the weekly excess death rates. Hatchett et al. [36] undertook a similar analysis on a smaller number of American cities where the timing of 19 different types of non-pharmaceutical interventions was available. They found that the early application of multiple interventions showed a trend towards lower cumulative excess mortality, but that no single intervention showed an association with improved aggregate outcomes for the pandemic. Both studies suggested that for non-pharmaceutical interventions to be beneficial, they should be applied early and in a sustained manner.
A further review of the U.S. public health response to the 1918 pandemic by Aimone [35] gave conflicting results. This review examined the public health response in New York City. In New York during the 1918 pandemic, mass gatherings were not prohibited nor were schools closed; instead, the city opted for a policy of staggered business hours to avoid rush-hour crowding, enhanced surveillance so that cases were quickly identified and isolated, and an intensive program of health education. The reported outcome measures for New York City were comparable with those seen in other American cities, and New York City experienced one of the lowest excess death rates on the eastern seaboard of the United States.
3.5. Event surveillance reports
Surveillance reports from four major sporting events within the last decade were considered suitable for review [38–41]. The study by Gundlapalli et al. [38] reported the experience of influenza surveillance during the Winter Olympics at Salt Lake City in 2002. No indication of the numbers attending was given, but it is assumed that the numbers were large. Twenty-eight cases of confirmed influenza from three clusters of influenza-like illness (ILI) were identified and these were restricted to either participants in the Games or support staff for the Games. The clusters consisted of 12 members of a national team who trained and lived together, 8 participants of a sport and 13 law enforcement officers who worked and lived in close proximity.
Lim et al. [39] reported on the experience of managing the Asian Youth Games at Singapore in June 2009. These games involved over 2000 athletes and officials from 43 countries. Although numbers of spectators are not given, it is assumed that the crowds were large. At the start of the Games, Singapore had already reported 600 confirmed cases of H1N1 (2009). Six laboratory-confirmed cases of H1N1 (2009) were identified during the 8 days of the event—four on one football team. No information on the numbers of confirmed H1N1 (2009) in the population after the Games was available.
There was no increase in ILI activity during the Winter Olympics in Torino in 2006 [41]. The final study by Schenkel et al. [40] reported on the experience of syndromic surveillance during the FIFA World Cup in Germany during June/July 2006. At the time, Germany was experiencing a very large outbreak of measles. Measles is essentially spread by the respiratory route and is highly infectious. However, despite enhanced daily surveillance, no outbreaks of respiratory disease or measles associated with the World Cup were detected.
3.6. Systematic review
As stated in Section 2.6, the approach to quality assessment of the reviewed papers was based on a pragmatic framework for categorizing studies into low- or high-risk for bias, depending on the presence or absence of significant methodological limitations. A high risk of bias was attributed to papers with at least two significant methodological problems as identified by the review authors (Table 6).
| Study type | Author (reference number) | Risk of bias | Key assessment issues |
|---|---|---|---|
| Quasi-experimental | Qureshi [18] | High | Randomization, blinding and allocation concealment? |
| Observational studies: cross-sectional | Deris [20] Rashid [23] Balkhy [24] Rashid [27] |
High Some Some Some |
Relevant control groups? Laboratory diagnosis? Appropriate follow-up? Reliable recruitment format? |
| Observational studies: cohorts | Choudhry [19] Gautret [21] Gautret [22] El Bashir [25] Gautret [26] |
High High High Some Some |
Unexposed control groups? Laboratory diagnosis? Appropriately classified study design? |
| Outbreak reports | Blyth [28] Botelho-Nevers [29] Gutierrez [30] Loncarevic [31] Pang [32] Saenz [33] Zepeda-Lopez [34] |
Low Low Low Low Low Low Low |
Clarity of description of setting and context? Use of laboratory diagnosis? Overall data reliability? |
| Outbreak reports (historical studies) | Aimone [35] Hatchett [36] Markel [37] |
Some Some Some |
Reliability and multiplicity of data sources? In-depth methods description? Clear outcome measures? Appropriate analysis? Breadth of coverage? Applicability to contemporary setting? |
| Event surveillance reports | Demicheli [41] Gundlapalli [38] Lim [39] Schenkel [40] |
Low Low Low Low |
Prospectively planned surveillance? Specific focus on influenza/respiratory virus? Clear description of setting and context? |
Papers included in the review, assessed for risk of bias.
4. Discussion
The evidence to help address important public health questions around mass gatherings and influenza transmission is sparse, especially in the context of an influenza pandemic. In addition, the topic does not lend itself to ease of scientific investigation and there are probably many who may feel that it is self-evident that mass gatherings facilitate the transmission of infectious diseases.
This systematic search of the literature identified a limited number of studies that addressed the review questions regarding whether mass gatherings are associated with influenza transmission and whether restricting mass gatherings reduces the spread of influenza within the community.
4.1. What is a mass gathering?
In attempting to understand and describe a situation or intervention, a common understanding or definition is essential. There is currently no generally accepted definition of what constitutes a mass gathering. However, the literature on mass gathering medical care highlights an emerging consensus amongst those providing emergency medical care at organized events. In this setting, mass gatherings are considered to be organized events with more than 1000 people in attendance [4–6]. A recently published guidance document from the World Health Organisation (WHO) expanded the term to cover any organized or unplanned event involving enough people to “strain the planning and response resources of the (host) community, State or nation” [42].
The major limitation in trying to define mass gatherings is that any single definition would inevitably be too simplistic as it would need to incorporate events as diverse as the Hajj (lasting about 1 month and involving between 2 and 3 million people), and a football match (involving several thousand spectators over a period of about 2 h).
A system for classifying mass gatherings on the basis of size and duration is lacking and may be required.
4.2. What does the evidence say about mass gatherings and the risk of influenza transmission?
In recognition of the difficulties of conducting hypothesis-based studies that directly implement and assess the effects of restrictions of mass gatherings in real life, an indirect approach was taken to address the review questions as follows:
4.2.1. Are mass gatherings associated with influenza transmission?
To address whether mass gatherings are associated with influenza transmission, evidence was derived from the following:
- -
A quasi-experimental study that was primarily designed to quantify vaccine efficacy in the form of a non-randomized trial.
- -
Observational studies that assessed participants before and after exposure to mass gathering events.
- -
Reports of influenza outbreaks and other respiratory illnesses at mass gathering events.
- -
Communicable disease surveillance reports from some major events.
A number of studies [18–22] have consistently demonstrated, over a number of years, that respiratory virus transmission occurs amongst pilgrims attending the annual Hajj in Saudi Arabia, and it is recognized as an issue of international public health significance [43–46] that could be particularly important in a pandemic situation. A significant proportion of pilgrims are affected by symptoms of either an influenza-like illness or an acute respiratory illness with the proportion affected reaching about 40% in some studies [19,20]. The Hajj is, however, a unique event with almost 3 million people converging on a relatively small geographic area for a period of at least 5 days, extending up to 4 weeks. Crowd density is very high and overcrowding in the living accommodation is common. Given the unusual nature of this event, the applicability of these findings to other mass gatherings is therefore limited. There is also a question regarding the fact that several of these studies are based on clinical criteria that could be due to other viral respiratory illnesses besides influenza.
In a small number of outbreak studies involving influenza-like illness and confirmed influenza at large music festivals, there is varying evidence about the extent to which influenza transmission occurs. Outbreaks were based on laboratory diagnosis, and transmission was confirmed in all, though they had varying infection rates ranging from roughly 3 to 25 per 100,000. Two recent studies undertaken during the 2009 pandemic suggest that at the beginning of a pandemic, these gatherings may act as seeding events [30]; indeed it has been suggested at the early stages of the 1999 pandemic A(H1N1), a huge Easter season mass gathering involving 2 million people may have helped in propelling the first wave of the outbreak throughout Mexico [34].
There is no compelling evidence from event surveillance reports, such as international athletic events, the World Cup and the Winter Olympics, to indicate that these major events significantly increase community transmission of influenza. Outbreaks did occur in some cases, but these always seemed restricted to the actual competitors and staff rather than the crowds attending or the wider community.
Together, all of these reports point to the potential for influenza outbreak and transmission in connection with large, multiple-day, open-air events. Thus there is some evidence to indicate that mass gatherings may be associated with an increased risk of influenza transmission, but it seems to be very variable.
4.2.2. Does the type of mass gathering influence the association with influenza transmission?
The type of mass gathering event seems to be of considerable importance in terms of the risk of influenza transmission (Table 7). Most of the evidence supporting the role of mass gatherings in the transmission of influenza comes from events where there are crowds with high crowd densities (which may be theoretically estimated at >5 people per square metre), and where the participants are likely to live close together for prolonged periods, e.g. the Hajj pilgrimage [18–22] and large musical festivals [28–30]. In these events, accommodations which are already likely crowded are also likely to be relatively basic, such as communal camp-style living, with the probable risk of sub-optimal hygiene facilities. It seems apparent that events where close contact among participants extends beyond event venues and into accommodation areas are most associated with influenza. Event size, per se, does not seem to be a critical factor.
| Numbers of participants | Duration | Example of type of event | Evidence of association with influenza? | Venue conditions | Accommodation conditions | Comment | |
|---|---|---|---|---|---|---|---|
| Indoors or outdoor | Crowded? | ||||||
| 1000 or more | Hours | Football matches | No – World cup [40] | Outdoor | Probably not crowded | Presumed little or no crowding | Low risk: no cases detected – outdoor, uncrowded venues |
| Theatre, entertainment | No – however, closures were associated with reduction in flu transmission [36,37] | Indoor | Probably crowded | Presumed no crowding | Some risk: associated with influenza despite equivocal crowding; indoor venues may be a risk factor | ||
| Days | Congress | Yes – outbreak report [33] | Indoor | Not crowded | Presumed no crowding | ||
| 100,000 or more | Days | Music festivals | Yes – outbreak reports [29–31] | Mostly outdoor | Crowded | Crowded | High risk: crowded venues plus crowded accommodations |
| Social/religious festival | Yes – outbreak report [28,34] | Mostly outdoor | Crowded | Crowded | |||
| 500,000 or morea | Weeks | Hajii pilgrimage | Yes – observational and quasiexperimental studies [18–27] | Both indoor and outdoor | Crowded | Crowded | |
| Major international multi-event tournaments | No/localized – event surveillance reports [31,38–41] | Mostly outdoor | Not crowded | Presumed little or no crowding | Low risk: outdoor, uncrowded venues seem ideal | ||
Major multi-event gatherings like the Olympics were included in this category, even if no specific numbers of participants were given in the reports.
Evidence of event characteristics that might influence an association with influenza transmission.
In contrast, there is no convincing evidence that major organized sporting events are associated with significantly increased influenza transmission in those attending the event [38–40]. An important example of this contrast comes from Serbia, where two major events of different type and scale happened to coincide in 2009, providing a “natural experimental” opportunity for comparison [31]. In the larger event, only four event-linked confirmed influenza cases occurred at the World University Games held over a 12-day period and involving almost 25,000 athletes and staff with about 500,000 spectators. However, in a relatively smaller event held in the same month and within the same country, as many as 47 event-linked confirmed cases occurred at a 4-day music festival with around 190,000 participants.
Furthermore, in surveillance reports from recent major international sports competitions, cases or small clusters of influenza were reported, but these were mainly among the event participants rather than among the overall population of people exposed to the events [38,39]. This was true even for one major event that took place within a pandemic context [39]. These events showed no clear evidence of influenza transmission, indicating that influenza may not be a significant cause for concern at modern world sports events. This view is supported by the surveillance report from the 2006 World Cup in Germany [40], where instances of transmission were not reported, meaning that they were either not detected or very low.
This situation may in part be explained by the brief transitory nature of contact in the crowds in highly organized international sports festivals such as the Olympics and the World Cup, which are usually seated events with good spacing in-between seats and mostly in open-air settings with dilution of any infectious droplets that may be generated. The apparently low or absent influenza transmission at such events may also reflect the contemporary fact that many people who attend major sports championships tend to have planned their visit a long time ahead, as ticket sales usually start months or even years in advance. Spectators as well as participants tend to stay in more conventional accommodations such as hotels rather than tents or other forms of portable or camp-style quarters with highly crowded conditions. It is also important to note that contemporary major events are now deploying increasingly developed systems for infectious disease surveillance and control [47], which are crucial for early detection and containment where possible.
The other situation of note relates to indoor events such as large conferences, typified by the international medical conference held over 7 days in Iran during the early stages of the 1968/1969 pandemic [33]. During this meeting it was estimated that about a third of the participants developed an influenza-like illness with an overall attack rate of 36%; the pandemic virus was isolated from those cases where testing had been undertaken. This potentially highlights the role that ventilation may play in the reduction of influenza transmission and is another factor worthy of consideration.
In summary, the type of mass gathering event seems to influence the risk of influenza transmission, key factors being the degree of crowdedness, the event duration and, possibly, whether the event is held indoors or outdoors. Multiple-day events with crowded communal accommodations may be the links to mass gatherings most associated with influenza.
4.2.3. Can influenza transmission be reduced by restriction of mass gatherings?
To address whether mass gathering restrictions can reduce influenza transmission, the mainly relevant papers found were archival studies of the 1918–1919 influenza pandemic [35–37] and an analysis of the 2003 SARS outbreak [32]. No relevant randomized controlled trials were found, reflecting the practical difficulties that such studies would involve.
Mass gatherings of varying dimensions were restricted at a large number of American cities during the 1918–1919 period. The reports again highlighted the difficulty of interpreting what was meant by a mass gathering, e.g. including schools, cinemas, theatres and other public places. In general, evidence suggests that these measures had a beneficial effect, especially where implemented early in the course of the outbreak [36,37]. However, these benefits were not universal across all the cities [35].
Restrictions were typically implemented as part of a set of interventions, e.g. combining quarantine and isolation policies with banning mass gatherings. As a result, it is extremely difficult to tease out the individual effects of mass gathering restrictions alone. Using multivariate techniques, investigators attempted to isolate the differential effects of individual restriction measures and found indications that certain interventions (such as closures of entertainment venues) had measurable specific impact [36,37], but this evidence is limited.
An analysis of the 2003 SARS outbreak in China attempted to probe the impact of mass gathering restrictions that were applied in a contemporary setting [32]. However, as with the historical studies, it was not possible to distinguish the specific effects of mass gathering restrictions from amongst the broad range of other public health interventions that were applied.
In summary, there is some evidence that when applied early and in tandem with other public health measures, such as isolation and quarantine and closures of educational institutions, mass gathering restrictions may help in reducing transmission. In a pandemic like that experienced during 2009, it is unlikely that the measures described above could be justified; however, in a much more severe pandemic, the cost–benefit equation could easily shift the other way. The application of bans on mass gatherings and other related public health measures are therefore highly dependent on an early indication of the severity as measured by its impact on individuals and society.
4.3. Practical implications of the findings of the review
There are two further, critical domains of uncertainty that need to be considered in the development of evidence-based guidance and policies regarding mass gatherings. The first domain relates to issues around the current understanding about how influenza is spread, and factors that can affect transmissibility (e.g. host factors, pathogen factors, environmental factors and particle size) [9]. Key questions remain in these areas, which may be important in making specific recommendations regarding particular types and scope of mass gathering restrictions.
The second domain impinging on the potential effectiveness of any public policy on mass gatherings includes the whole range of factors affecting adherence and compliance. For instance, the experience of the 2009 pandemic has raised significant questions around how willing people might be to comply with bans imposed on mass gathering restrictions [48–51]. Other challenging issues include the problematic ethical and legal frameworks for implementing restrictions for public health purposes [52,53], as well as considerable logistical and economic implications. If long-planned events were to be cancelled, who would be liable for the huge personal, corporate and national costs that such cancellations might incur? In considering policy recommendations within a pandemic context, the most practical approach for all but the more severe pandemics may be a strategy of encouraging voluntary restrictions. This would involve giving the public the best available information and advising rather than legislating that organizations and individuals avoid non-essential events where there is at least some evidence of transmission risk. For such a strategy to have a chance of succeeding, it would be most important to have in place a carefully and sensitively prepared communication strategy, since recommendations to avoid public gatherings are likely to run against powerful social pressures to do otherwise [54]. The success of any public health strategy—and this must be particularly true in relation to a potential or imminent pandemic situation—requires the building of trust [55] and an intelligent and purposeful engagement of the public even prior to the event [56].
There are other important issues to note. Although this review has focused on mass gatherings, limiting transmission of influenza clearly requires a multifaceted approach. Some studies in this review reflected such an approach; for example, in the historical outbreak investigations where restrictions on mass gatherings were combined with other non-pharmaceutical measures [32,36,37]. It would be prudent to apply the best evidence relating to other social distancing interventions in conjunction with any specific policies on mass gatherings.
An additional question that should be considered is whether non-pharmaceutical health interventions such as mass gathering restrictions, actually reduce the health burden of influenza, or only modify the epidemiology by temporarily delaying the eventual impact of an event such as a pandemic. It is tempting to speculate on the possibility of a reduction in disease burden; historically, some of the American cities that implemented mass gathering restrictions during the 1918–1919 pandemic seemed to achieve significant reductions in peak morbidity and mortality that may well have reduced the overall burden. However, pragmatically, countries like the United Kingdom aim to achieve a slower spread, to prolong the troughs and to flatten the peaks of the epidemic curves to buy time for countermeasures to take effect and to enable services to cope with a lower volume of activity.
In this context, the most important point to emphasize is that mass gathering restrictions must only be a part of a range of interventions. The synergistic effects of multiple interventions is what would allow the best chance to achieve significant reductions in overall burden.
4.4. The need for further evidence
More evidence is needed on this subject. There is a need for well-designed studies to more accurately quantify the nature of the infections causing flu-like symptoms at mass gatherings, confirm the key parameters that influence the transmission of influenza in these settings, and to directly assess the impact of mass gathering restrictions. But as “gold standard” randomized comparison designs are extremely difficult to apply to this kind of intervention, attention needs to focus on optimal observational study options. From a UK perspective, British people travelling abroad for mass gatherings such as the Hajj or other large events could be approached for inclusion in prospective studies for comparison with appropriately matched, non-travelling controls, with care being taken to avoid drawbacks observed in existing studies. Within the UK, mass gatherings ranging from indoor events in theatres and cinemas, to outdoor events such as football matches and major musical events like the Glastonbury festival or Travellers’ horse fairs represent potential opportunities for carefully designed prospective cohort studies to be undertaken. The biggest issue is persuading funders that given the current paucity of good studies, such further research is still needed.
4.5. Strengths and weaknesses of the review
As previously noted, this review has examined an intervention area in which there are a limited number of relevant studies and there is limited common understanding of what constitutes a mass gathering. Despite these challenges, it has been possible to extract limited strands of evidence that may be useful towards policy development. Also, within the boundaries of the inclusion criteria, and despite the limited work timescale, this review was able to capture all the relevant studies identified by recent systematic reviews investigating non-pharmaceutical interventions designed to limit transmission of influenza and/or other respiratory viral infections [7,8,57].
However, due to time constraints in carrying out this work, as described in Section 2.5, while every effort has been made to be as comprehensive as possible, it is acknowledged that the rapid evidence assessment process necessarily involved some limitations. The literature search is not necessarily exhaustive and there is therefore a possibility of incomplete retrieval of all potentially relevant studies.
While a range of study designs were reviewed, there was not a single randomized controlled trial that was suitable for inclusion. This is of course not surprising, given the formidable logistical, cost and ethical hurdles that make large-scale experimental epidemiological studies of the restriction of mass gatherings impractical and probably impossible. Some of the included studies had significant design and quality issues as duly reflected in the individual paper summaries and the discussion, and highlighted in Tables 4 and 6.
A common issue with a number of the studies included in the review is that they depended on clinical symptoms like cough or syndromes such as influenza-like illness, rather than laboratory diagnosis of influenza. In such studies it is not possible to isolate the impact of influenza as opposed to other respiratory viruses, and the risk of influenza could potentially be over-interpreted. In the studies where laboratory testing was undertaken, influenza was only confirmed in minority proportions of people with respiratory symptoms, ranging between 6% and 14% [23,24,27], but possibly up to a roughly estimated 40% in one study [25].
This review did not include specific “specialized” settings that may arguably be regarded as mass gatherings, such as groups of people travelling for periods of time on cruise ships. The authors took the view that any transit-related settings would be best considered under a separate evidence review of influenza transmission through transportation. Modelling studies were also excluded, and it is acknowledged that their inclusion may offer an additional dimension in order to build a fuller picture.
The application of quantitative techniques could have potentially enhanced the simple narrative approach that was adopted for the analysis. However, there are insufficient studies presenting quantitative data on this subject, and moreover, there is a high level of heterogeneity amongst the identified studies.
5. Conclusion
In conclusion, there are limited data indicating that mass gatherings are associated with influenza transmission. Some evidence suggests that restricting mass gatherings together with other social distancing measures may help to reduce transmission. However, the evidence is not strong enough to advocate legislation or proscription. Therefore, in a pandemic situation a cautious policy of voluntary avoidance of mass gatherings would be prudent.
6. Conflict of interest statement
None declared.
Acknowledgements
The initial scoping for this work was based on a review written by Dr. Mark Zuckerman in 2009 (unpublished); this is gratefully acknowledged. The authors are indebted to a number of colleagues who critically reviewed the manuscript or otherwise advised us at different stages, particularly Dr. Mary Chamberland, Prof. John Watson, Dr. Alison Weightman, Dr. Anna Cichowska, Prof. Angus Nicholl, Dr. Ibrahim Abubakar and Prof. Anthony Kessel. We are grateful for the comments of members of the UK Health Protection Agency Influenza and Respiratory Viruses Programme Board and the UK Department of Health Scientific Pandemic Influenza Advisory Committee. Librarians at the HPA Colindale site provided valuable bibliographic assistance. David Ishola is supported by an NIHR Clinical Lectureship.
References
Cite this article
TY - JOUR AU - David A. Ishola AU - Nick Phin PY - 2011 DA - 2011/08/17 TI - Could influenza transmission be reduced by restricting mass gatherings? Towards an evidence-based policy framework JO - Journal of Epidemiology and Global Health SP - 33 EP - 60 VL - 1 IS - 1 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2011.06.004 DO - 10.1016/j.jegh.2011.06.004 ID - Ishola2011 ER -