
Assessing the overuse of antibiotics in children with URTIs in Saudi Arabia: Development of the parental perception on antibiotics scale (PAPA scale)
- DOI
- 10.1016/j.jegh.2012.11.005How to use a DOI?
- Keywords
- Validity; Upper respiratory tract infections; Antibiotics overuse; Delphi Technique; Psychosocial; Measurement instrument; Saudi Arabia; Australia
- Abstract
Background: Antibiotic overuse is influenced by several factors that can only be measured using a valid and reliable psychosocial measurement instrument. This study aims to establish translation and early stage validation of an instrument recently developed by this research team to measure factors influencing the overuse of antibiotics in children with upper respiratory tract infections in Saudi Arabia.
Method: The content evaluation panel was composed of area experts approached using the Delphi Technique. Experts were provided with the questionnaires iteratively, on a three-round basis until consensus on the relevance of items was reached independently. Translation was achieved by adapting Brislin’s model of translation.
Results: After going through the iterative process with the experts, consensus was reached to 58 items (including demographics). Experts also pointed out some issues related to ambiguity and redundancy in some items. A final Arabic version was produced from the translation process.
Conclusion: This study produced preliminary validation of the developed instrument from the experts’ contributions. Then, the instrument was translated from English to Arabic. The instrument will undergo further validation steps in the future, such as construct validity.
- Copyright
- © 2013 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
1.1. Antibiotics and upper respiratory tract infections
Despite the effectiveness of antibiotics to treat bacterial infections, they are often inappropriately used to treat viral infections. This overuse is currently one of the major public health issues worldwide [1–4]. Several problems are associated with the overuse of antibiotics; for instance, development of antibacterial resistance, increasing the burden of chronic diseases, rising costs of health services, and the development of side effects (e.g. adverse gastrointestinal effects). Antibiotic overuse was found to be significantly frequent in children, especially when presenting with viral upper respiratory tract infection (URTI) [5].
Several researchers have studied this increasing consumption of antibiotics through the years and an increasing trend of inappropriate consumption has been demonstrated in Saudi Arabia and many other countries [6–12]. Moreover, Al-Shimemeri et al. [13] found that antibiotics were the drugs most commonly prescribed by the primary care physicians for all age groups, representing 40–63% of the total drug prescriptions in the Asir region, in southern Saudi Arabia. Similarly, Ahmed and Al-Saadi [6] studied the prescribing patterns of 200 doctors in Saudi Arabia and found that among the most frequent drug categories prescribed for all age groups were antibiotics. Thus, information from these resources emphasizes the need for continuing medical education on the physicians’ rational prescribing behavior.
This overuse of antibiotics is influenced by several factors. Numerous studies attempted to discover these factors; some assessed attitudes, beliefs, and knowledge of antibiotic use [14–20], others assessed behaviors (e.g. over-the-counter medication and self-medication) [2,16,20–26], and some studies measured the patients’ perceptions regarding patient–doctor interaction, patient satisfaction, and patients’ experience with antibiotics [18,28,29]. These studies provide a framework for the present study.
Self-medication is an important issue in Saudi Arabia [22] and several adjacent countries, including Kuwait [24], Jordan [26,30] and Sudan [20]. Factors influencing this behavior in Saudi Arabia need to be measured in order to minimize the overuse of antibiotics in children with URTIs. Information regarding the antibiotic consumption in Saudi Arabia is very limited, and there are no reports on the trends in antibiotic use among Saudi children, especially those with URTIs [31]. Thus, it is important to measure this phenomenon in Saudi Arabia.
1.2. Validity
In order to measure the psychosocial constructs influencing the overuse of antibiotics, a valid and reliable instrument needs to be available. Kimberlin and Winterstein [32] studied the issues related to the validity and reliability of measurement instruments used in research; they believe that the psychosocial phenomenon, such as antibiotics overuse, could only be measured using psychosocial measurement instruments. Furthermore, an extensive literature review has shown that there is no validated instrument that measures the factors influencing antibiotics overuse in children with URTIs [33].
Marshall et al. [34] demonstrated the significance of validity and reliability in measurement instruments in a study conducted to examine schizophrenia; they found that non-validated scales resulted in a type-one error where participants were 40% more likely to report that the treatment was effective when non-validated scales are used compared with validated ones.
1.3. Early stage validation
Validation is a multi-step process; the preliminary validation steps are content validity and face validity.
Content validity addresses the development of items included in the instrument, and measures how well these items adequately represent the construct being measured. Carmines and Zeller [35] defined “content validity” as “the extent to which a measurement reflects the specific intended domain of content.” However, there is no statistical test to determine whether a particular measure adequately covers a content area or adequately represents a construct. Content validity usually depends on the judgment of experts’ knowledge with respect to the subject matter [36,37].
Beaulieu et al. [38] recommended checking the content validity of an instrument in three domains: (1) the completeness of items included in the developed instrument, i.e., to provide evidence that all key elements related to the study objectives are included in the instrument; (2) comprehensiveness of items included in the instrument in relation to the indicators being tested; and (3) the items are clearly stated and are unambiguous. This study will attempt to validate the instrument’s content in the above domains.
Face validity focuses on subjective assessment [39], such as, checking grammar, syntax, organization, appropriateness, and confirmation that it appears to flow logically. It is used to check if the test appears valid to personnel who administer it, to examinees who take it, and to other untrained observers [40]. This study focuses on the point of view of the personnel who administer it.
1.4. Instrument’s translation
Translating the developed survey instrument’s data is necessary since it is in English and the target population where the instrument data would be administered is for the benefit of Saudi parents (i.e. Arabic language). Therefore, cross-cultural translation is important for administering the instrument to the target population. This translation process is a difficult task, and the instrument needs to be culturally acceptable and aptly translated to be valid [41,42]. This study shows the translation process of the newly developed instrument by adopting Brislin’s [43] model of translation.
2. Method
2.1. Content and face validity
To assess the content and face validity of the survey instrument being developed, this study used a content evaluation panel to build the group brainstorming process [36]. The panel was composed of experts knowledgeable in the areas of pediatrics, infectious diseases, epidemiology, family medicine, psychology and counseling, and social sciences. After obtaining an ethical approval from the University of Dammam, Saudi Arabia, and Queensland University of Technology, Australia, Panelists were approached via email. Each panel member was independent, and anonymity of panel members was ensured. All the panelists were supplied with a document including background information and a cover letter explaining the study; expert’s response to the questionnaire was considered their consent for participation. Twenty experts were approached and agreed to participate in the study: 11 experts were from Saudi Arabia and 9 from Australia (Table 1). Half of the panelists (10) were males and half were females.
| Specialty | Nationality | Total | |
|---|---|---|---|
| Saudi | Australian | ||
| Family medicine | 2 | 0 | 2 |
| Pediatrics | 3 | 0 | 3 |
| Epidemiology | 4 | 1 | 5 |
| Pediatric infectious diseases | 1 | 0 | 1 |
| Psychology | 0 | 6 | 6 |
| Social sciences | 0 | 1 | 1 |
| Emergency | 0 | 1 | 1 |
| Quality specialist | 1 | 0 | 1 |
| Total | 11 | 9 | 20 |
Nationality and Specialty of Experts.
The study was conducted using the Delphi Technique [27], which is an iterative process seeking consensus from a group of panel members or content experts through multiple rounds of questionnaires. The Delphi Technique was used instead of focus groups because of: (1) the inability of group members used in the study to meet in person; and (2) the individuals involved are less likely to be influenced by other group members than if they were meeting in person.
The Delphi process consisted of three rounds (Fig. 1):
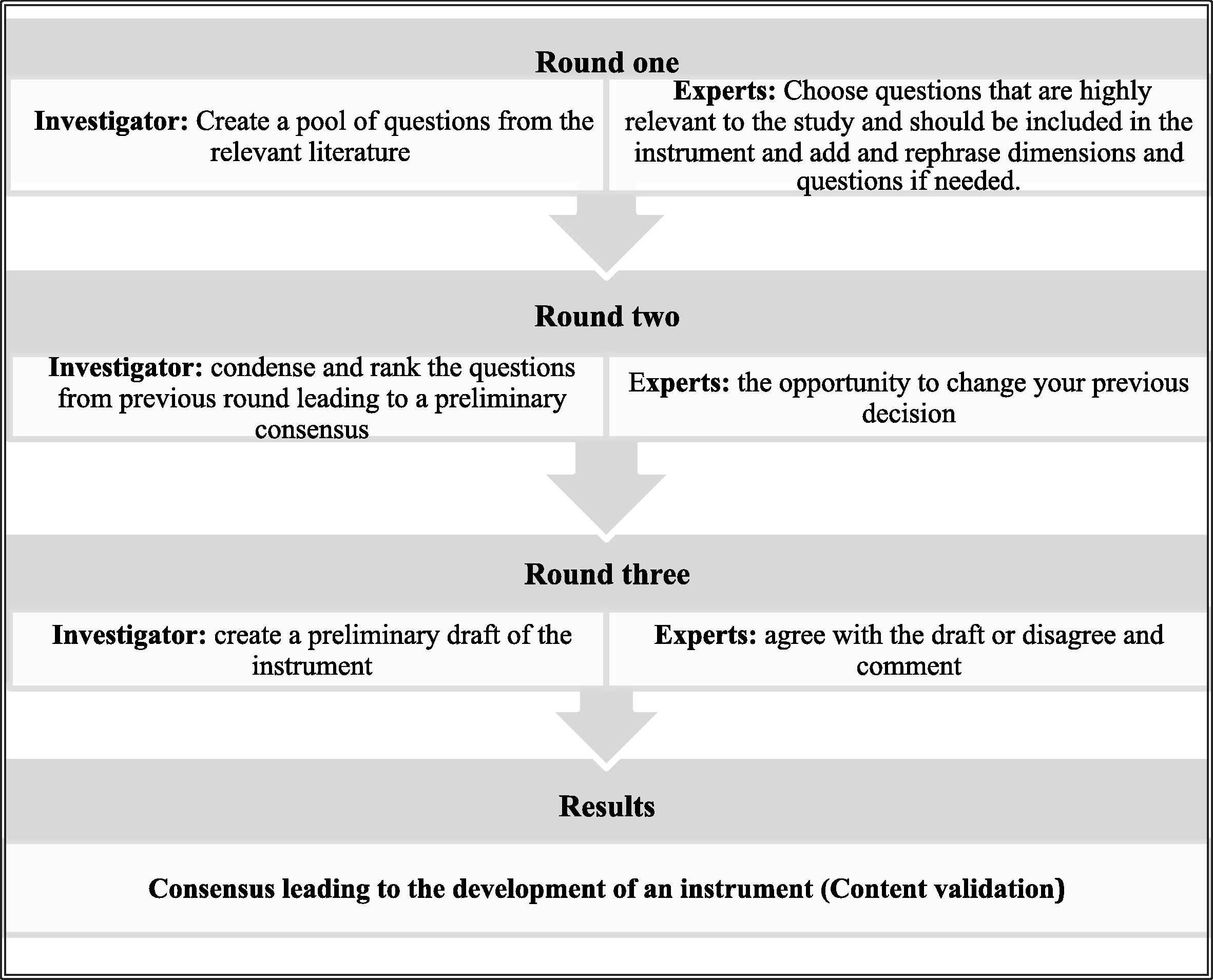
The Delphi Technique Process.
2.1.1. Round 1
In the first round, a total number of 18 experts responded (90% response rate) (Table 2). The lack of response from the two missing experts was due to their unavailability for this round. Experts were provided a pool of 80 questions, retrieved from the relevant literature [15,29,44–47]. Independent of the other panelists, each member was asked to choose the most relevant questions to measure the study objectives, i.e., factors influencing the overuse of antibiotics in children with URTIs in Saudi Arabia. In this round, experts were given complete freedom in their response and were invited to generate ideas [48]. Experts were also asked to decide on which dimension each question falls within, i.e. knowledge, behaviors, attitudes, and beliefs.
| Rounds | Round one N = 20 |
Round two N = 18 |
Round three N = 14 |
|---|---|---|---|
| Saudi experts | 11 (55%) | 9 (50%) | 8 (57%) |
| Australian experts | 7 (35%) | 5 (28%) | 4 (29%) |
| Response rate | 18 (90%) | 14 (78%) | 12 (86%) |
Overall response rate.
2.1.2. Round 2
The persons who responded to the first round were only included in the second round and so forth in the third round. Fourteen experts out of the 18 responded in the second round (78% response rate). After the analysis of the first round, the included questions, i.e. items that obtained more than half of the experts’ agreement [49], were sent back to the experts along with the percentage of agreement for each item. Experts were asked to agree, disagree, and/or comment on the items. Then, the first draft of the questionnaire was complete based on the experts’ feedback from this round.
2.1.3. Round 3
The first draft of the questionnaire was then sent to the experts to obtain their final confirmation, where they had three options for each section of the questionnaire: (1) agree without comment, (2) agree with comment, or (3) disagree with reason. Twelve experts out of the 14 included in the previous round responded in this round (86%).
Comments and suggestions from the experts were also reviewed and discussed within the research team, and decisions were made where some comments were accepted while others were dismissed because of several reasons: (1) the comment does not apply to the study population; (2) the change requested in the comment may affect the future analysis procedures of the instrument (i.e., factor analysis); or (3) the comment or suggested question does not apply to the study objectives.
During the three rounds of the Delphi process, experts were asked to comment on the clarity and flow of the questions, including: grammar, syntax, organization, and appropriateness. The information obtained from the experts was used to assess face validity of the instrument.
2.2. Instrument’s translation
After assessing the content and face validity of the survey instrument, the instrument’s translation took place to assess translational validity by adapting Brislin’s [43] model of translation (Fig. 2). The developed survey instrument was sent to two independent bilingual translators. One was a health professional and the other was an accredited translator with a degree in linguistics. The survey was from the source language (English) to the target language (Arabic). The two versions of the translated instrument were then reviewed and compared by a panel of four persons. After consensus regarding the difference between the two translated versions of the instrument, the final (Arabic) version was ready. After that, the forward-translated version (Arabic language) was then sent to two independent bilingual translators – one health professional and the other an accredited translator – to conduct the back-translation. The panel then compared the two versions of the back-translated instrument for any differences, and came up with the final back-translated version. The research team then compared the original instrument to the back-translated instrument, and the instrument translation was achieved.
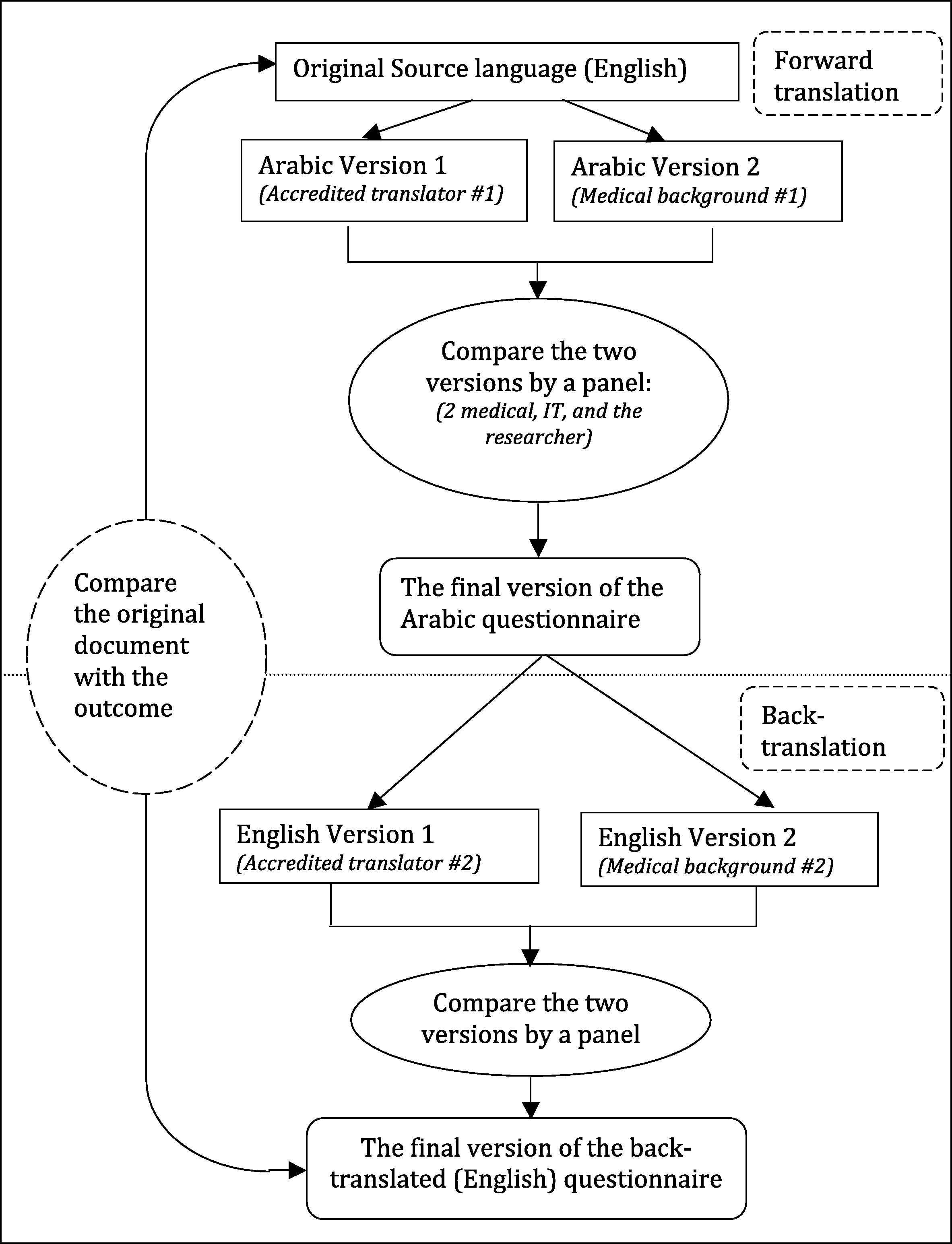
Translation Process.
3. Results
After feedback was obtained from experts, results were analyzed and condensed and only items perceived to be relevant by more than half of the panelists were included in the second round [49]. As a result, 42 items were excluded from the instrument (first-round questionnaire and last-round questionnaire are attached). After discussion within the research team, 10 questions out of the 20 suggested were added to the second round.
The second round resulted in the exclusion of 5 items and the inclusion of 2 suggested items related to antibiotics adherence, making the total number of items included in the instrument 45. After confirmation from the experts, the final version of the instrument (attached) consisted of 45 items related to three different domains: knowledge, behaviors, and perceptions (attitudes and beliefs).
In the knowledge domain, there was evident diversity between the experts’ judgments according to their specialty. Questions related to antibiotics awareness were thought to be irrelevant by all of the psychology specialists included in the study, while on the other hand the same questions were chosen by all of the medical doctors. These questions include: ‘Antibiotics are needed for: the common cold’ and ‘Antibiotics are needed for: ear infection.’ Thus, it was concluded anecdotally that the experts’ judgment is highly influenced by their specialty and that their decision on the relevance of items included in the questionnaire is highly associated with their area of expertise.
Infectious disease specialists, pediatricians, and family doctors were more interested in measuring adherence and previous experiences with antibiotics than any other kind of specialty included in the study (psychology, epidemiology, emergency medicine, and social sciences). Psychology specialists were more interested in measuring attitudes, beliefs and behaviors of the respondent, and were not interested in measuring the respondents’ expectations and satisfaction.
There was some confusion with regard to the grammar of questions related to attitudes and behaviors. After the experts’ review, it has been agreed that past tense questions are considered behavior-related questions, while present tense questions are attitude-related questions.
In addition, after comparing the results from experts according to their gender, no significant difference was found among the experts in the study.
4. Discussion
No previous study has attempted to develop and preliminarily validate a survey instrument that measures the factors influencing the overuse of antibiotics in children [33]. This study established preliminary validation steps (i.e. Content validity, Face validity, and Translational validity) of a survey instrument developed to measure the factors influencing parents to overuse antibiotics in children, especially when upper respiratory tract infections are present.
The dimensions included in the survey instrument according to the experts’ feedback were parents’ knowledge, parents’ behaviors regarding antibiotics usage (including self-medication, over-the-counter medication, previous experience, and adherence to antibiotics), and parents’ beliefs and attitudes (including expectations and satisfaction).
A few significant points were noticed when analyzing the results, such as questions about antibiotics self-medication, patient–doctor interaction, and geographical background, which all had significant feedback from the experts. Also, the format of the questions, whether open-ended or close-ended, was not consistent among the experts’ feedback. Moreover, redundancy of some of the instruments items was questionable by some experts.
Antibiotics self-medication is an important aspect to be measured when assessing the overuse of antibiotics in a community [5,16,20–24,26,50]. Antibiotics self-medication is going to be measured by asking the respondents for their source of antibiotics using these two questions: ‘I get my child’s antibiotics from the pharmacy with a prescription’ and ‘I get my child’s antibiotics from the pharmacy without a prescription.’ Experts in the study argued that these two questions could be collapsed into one question. However, these two questions are not mutually exclusive, i.e., disagreeing with one of these questions does not necessarily imply the agreement to the other. Therefore, both questions were added in the instrument.
Patient–doctor interaction and patient satisfaction are important factors influencing the overuse of antibiotics [18,27–29]. Thus, parents’ perception of the patient–doctor interaction is planned to be measured using this question: “Doctors don’t inform the parents well about their child’s condition” and similar questions. A few experts in the study believed that this question is not relevant to the study objectives; some of them thought that this would not be reliable since the study is measuring the factors influencing the parents’ overuse and the doctors’ over–prescribing of antibiotics. While others thought that doctors in Saudi Arabia do not have the time for health education owing to the large number of patients doctors see each day.
Five experts argued that the questions about the geographical background are not important and are irrelevant to the study objectives. However, from a psychosocial point of view, it has been made evident that attitudes develop throughout a person’s childhood until they reach adulthood [37]. Therefore, it is important to test this hypothesis, whether attitudes defer between participants according to their geographical background.
Many experts thought that items related to the sources of information could be collapsed into one open-ended question. This would not be applicable due to the importance of using a Likert [51] scale in the response options for ease of analysis in later stages of this instrument’s validation, i.e., factor analysis [52].
Redundancy in some of the items such as: “My child will be sick for a longer time if he/she doesn’t receive an antibiotic for cough, cold, or flu symptoms,” and “Children with the common cold get better faster when antibiotics are given” might be useful in the assessment of internal consistency reliability [36].
5. Limitations
Experts’ inability to follow-up was owing to: (1) the iterative nature of the methodology used, i.e., the Delphi Technique; and (2) the nature of their jobs, i.e., either medical doctors or academics.
6. Conclusion
An instrument was developed in this study using the relevant literature, and experts in areas including pediatrics, infectious disease, epidemiology, psychology and counseling, social sciences, and emergency medicine were used to assess the content validity of this instrument. The aspects related to the instrument’s comprehensiveness of items that measure the underlying constructs, the importance of the included items in relation to the object matter, and the clarity of the items were assessed at this phase of instrument development using experts’ judgments.
Experts’ specialties and nationalities could have an effect on their judgment on the inclusion or exclusion of certain items in the instrument. Experts’ gender, on the other hand, showed no significant difference in regard to their decision on the relevance of items included in the instrument.
The study resulted in preliminary validation of a survey instrument that includes: 9 items in the demographics section, 4 items in the child’s history section, 20 items in the knowledge section, 12 items in the behaviors section, and 13 items in the perceptions (attitudes and beliefs) section.
Acknowledgment
We thank the content experts included in the study for their invaluable input.
References
Cite this article
TY - JOUR AU - Arwa Alumran AU - Xiang-Yu Hou AU - Cameron Hurst PY - 2013 DA - 2013/01/26 TI - Assessing the overuse of antibiotics in children with URTIs in Saudi Arabia: Development of the parental perception on antibiotics scale (PAPA scale) JO - Journal of Epidemiology and Global Health SP - 3 EP - 10 VL - 3 IS - 1 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2012.11.005 DO - 10.1016/j.jegh.2012.11.005 ID - Alumran2013 ER -