
Socioeconomic inequity in health care utilization, Iran
- DOI
- 10.1016/j.jegh.2013.03.006How to use a DOI?
- Keywords
- Concentration index; Inequity; Health care utilization; Socioeconomic situation
- Abstract
Reducing poor–rich inequities in health is one of the priorities of both national and international organizations and is also one of the main challenges of health sectors in Iran. Since, in the view of policy making, quantifying the size of inequity in health care utilization (HCU) is a prerequisite for achieving this goal, the current study aimed to determine and compare the socioeconomic inequity in HCU by concentration (C) index and odds ratio (OR).
Methods:
A total of 758 households, consisting of 2,131 subjects who were aged 15 or older, were involved in this cross-sectional study, and their data were gathered through interviews. Household economic index (HEI) was created by the factor analysis from the asset data. The C index and OR were used as measures to determine the overall inequity in HCU according to sex (male/female), living area (urban/rural), insurance, and types of HCU (general physician [GP], specialist, and Health Workers [HWs]).
Results:
The overall rate of HCU was 66.4%. The rates of using GP, specialist care, and HW care were 21.4%, 21.6% and 21.8%, respectively. The overall inequity in HCU was equal to 0.05 (95% confidence interval; −0.069 to 0.165). The C indexes in HCU, according to the subgroups of HCU, were measured as 0.11 (0.09–0.12) for GP, 0.115 (0.01–0.13) for specialist and −0.065 (−0.08 to −0.05) for HWs. Although the rate of utilization increased from poor to rich quintiles, the inequity regarding sex and living area was also low and non-significant.
Conclusion:
People with higher HEI used more specialist and GP care, while people with lower HEI used more HW care. The inequity in HCU was low and non-significant in different quintiles of males, females, urban and rural, as well as those who were insured.
- Copyright
- © 2013 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- Open access under CC BY-NC-ND license. http://creativecommons.org/licenses/by-nc-nd/4.0/
1. Introduction
Based on the available literature on the issue of inequity, it is clear that this topic is important regarding health policy and health decision making [1,2]. In addition, persistent disparities in health regarding socioeconomic position have had a long history in health policies in many developed and developing countries [3]. Moreover, reducing poor–rich inequities in health care has recently become one of the most important priorities of national governments and international organizations [3]. According to Iran’s health innovation and science development plan, the goal of reducing the inequity is one of the main challenges of health sectors in Iran [4]. However, establishment of the value of these differences and quantifying the size of the inequity is a prerequisite for achieving this goal [3]. Therefore, a great number of methodological studies have been recently conducted on health inequity using the methodology developed by Van Doorslaer et al., Wagstaff et al., and Kakwani et al. [5–8]. This methodology is based on a decomposition analysis of the concentration index. Also, other studies have been performed to compare the inequity indexes among countries regarding health care utilization (HCU) [5,6]. The inverse care law was described by Hart [9] for inequity in medical service access in South Wales as: “The availability of good medical care tends to vary inversely with the need for it in the population served,” followed by other researchers [10–13] and challenged in other studies [10,12]. However, in Iran, public sectors provided free primary health care for all people even for satellite rural areas. This care was delivered in the first level of the systems in health centers by health workers. The financing of specialized care, such as dental or surgical care, is not free. Nevertheless, unfortunately, no published articles on the issue of inequity in HCU in Iran were found. Hosseinpoor et al. published results of a national health services utilization survey, but that study did not utilize an inequity approach [14]. However, inequity in infant mortality was established across provinces of Iran, and a wide range of inequity was observed in different local areas [15].
Recent studies showed inequity in health indicators, such as childhood malnutrition and HCU, among developed and developing countries [2,5,15–17]. The results of these studies indicated that although inequity has decreased over the past years, there were differences in health indexes among different socioeconomic subgroups of people. In addition to the socioeconomic status, these studies showed that living area, insurance, job, age, and sex were the determinants of HCU [5,16–19].
Using some health policies, developing countries tried to decrease some inequities by universal coverage of insurance and other facilities, such as rural insurance and family physician, which are implemented in Iran [20,21]. However, the form of inequity in HCU has been changed recently in a way that higher-income groups have more medical specialist care utilization while general physician care utilization is more in lower-income groups [6]. Therefore, more studies need to be conducted in these areas on the pattern, rather than existence, of inequity in HCU and the type of utilization. Markazi province is located in the center of Iran, and in spite of high access to health, it experienced a high inequity in infant mortality rates compared with other provinces [15]. Also, with all the improvements in the health indicators in the country [22,23], the burden of diseases in this region was higher than other provinces in 2006 – respiratory system diseases were in the third rank of diseases with regard to years of life lost [24]. Moreover, previous works [18,19] showed evidences of disparity among people in different social and demographic groups in this province.
However, according to the viewpoint of policy makers, the inequity or other health indicators are more likely to be reported locally [5,15]. Therefore, it was decided to quantify the socioeconomic inequity in HCU in the Markazi province, Iran, by using the concentration (C) index and odds ratio (OR) in order to provide a measure for policy makers to use regarding the pattern of HCU in people with varied socioeconomic status.
2. Material and methods
2.1. Study area
This study was carried out using the data of the HCU survey which had been conducted in the Markazi province, Iran, from February 16 to March 1, 2008. It is one of the central provinces in Iran that is located 293 km southwest of Tehran, the capital [24]. People’s access to health services is high due to the nearness of the province to the capital and other mega cities, such as Isfahan and Qom.
2.2. Subjects and instrument
In this survey, 758 households were selected through the systematic sampling method, based on the sampling schedule of the Iranian household framework which exists in the Health Promotion and Network Development Center at the Ministry of Health and Medical Education [25]. In the selected households, the data of all members of the household (totaling 2131 subjects) who were aged 15 or older were gathered by trained interviewers. The interview method used for data collection and data entry was saved in a pre-tested questionnaire [25]. This questionnaire was used before in another HCU survey in Iran in 2002 [26].
The main outcome of this survey was to investigate whether there was a self-reported need for outpatient care services two weeks before the interview. Therefore, the timely utilization of health care was measured; utilization was defined as seeking care relative to need. In addition, regarding the subjects who reported any need to the outpatient care, the household asset data, including the number of people per number of rooms as an indicator of crowding, household sanitary facilities, e.g. bathroom, toilet, kitchen facilities, including separate kitchen, using kitchen stove, fridge, freezer, refrigerator, microwave, safe heating and cooling devices, and household electronics, such as television (black and white, color, or LCD), mobile phone, dishwasher, washing machine, vacuum cleaner, computer, Internet access at home, motorcycle, car, and ownership of residence were gathered and used for construction of the household economic index (HEI). In addition, the people who were in need of outpatient care were referred to locations near their homes. In fact, some patients were assigned to a family physician and a health worker (HW) in one category of this study because the family physician program in Iran was intended to provide free or inexpensive care for the rural and urban areas that have less than 20,000 residents [20,21].
2.3. Statistical analysis
According to the recommendations of other studies, principle component analysis (PCA) was applied to the asset data and the first component was used as the HEI [3,27,28]. In the next stage, the scores of the first component of PCA were arranged in an ascending manner, and then the subjects were categorized into five stratums. The first quintile consisted of the poorest people, while the fifth quintile included the richest ones. Therefore, each quintile included one fifth of the people.
2.4. Measuring of inequity
The C index was used as a measure of the inequity in health care utilization. The Lorenz curve (LC) plots the cumulative proportion of the population, which is ranked by HEI from the poorest to the richest, against the cumulative proportion of the health variable. The C index is defined as twice the area between the diagonal and the LC [8]. If the LC lies above the diagonal, it takes a negative value and shows that the health variables are concentrated among the poor people. On the contrary, if it lies below the diagonal, it indicates that the health variable is concentrated among the rich people and C takes a positive value [7,8]. The maximum and minimum of the C index varies from −1 to +1 [7]. In addition to the C index, the OR was calculated as another measure of the inequity. In calculating the OR, the two lowest quintiles were considered the reference group – the odds of HCU in the fourth and fifth quintiles divided by the odds of HCU in the first and second quintiles. Moreover, C and OR were estimated based on the robust estimator of regression analysis to account for the clustering effect of the household for the confidence interval [15].
In the present study, C was calculated by the following formula, as suggested by Kakwani et al. [8].
In the above formula, μ and μt are means of the health variable in the population and the tth group, respectively. Besides, ft, is the group share of the population. Moreover, Rt, is the relative rank of the tth HEI and is obtained through the following formula:
Therefore, Rt indicates the cumulative proportion up to the midpoint of each HEI group interval. Also, the confidence interval of C was also calculated through the Wagstaff and Van Doorslaer method [29].
After calculating the C for HCU, stratification analysis was used according to sex (male/female), living area (city/rural), type of HCU (GP, specialist, and HW care), and having valid insurance in order to adjust the effect of these variables on the C index. The data were analyzed by Excel 2007 and STATA (v.9) software.
3. Results
The response rate was 99.7%. From the 2131 subjects under study, 779 had reported the need for outpatient care two weeks before the interview. Out of these subjects, 517 (66.4%) had sought their need and 97.7% of those used outpatient care. The results, which are presented in Table 1, provide information regarding the rate of HCU and three types of HCU, including using GP, specialist and HW care. The overall rate of HCU was measured as 66.4%. Moreover, the rates of HCU were calculated as 21.4%, 21.6% and 21.8% for using GP, specialist, and HW care, respectively. In addition, the rate of overall HCU and HCU in males, females, rural as well as urban areas and insured subjects in the richest quintile was higher in comparison to other quintiles. Also, the rate of using the specialist care in the first quintile was lower, while the rate of using HW care in the poorest quintile was higher.
| Poorest quintile | 2nd Quintile | Middle quintile | 4th Quintile | Richest quintile | Total/average | |
|---|---|---|---|---|---|---|
| HCU-overall | 0.558(0.04) | 0.635(0.039) | 0.686(0.037) | 0.692(0.037) | 0.748(0.035) | 0.664(0.017) |
| HCU-males | 0.483(0.066) | 0.525(0.065) | 0.689(0.059) | 0.631(0.06) | 0.686(0.055) | 0.607(0.028) |
| HCU-females | 0.602(0.049) | 0.701(0.046) | 0.684(0.048) | 0.736(0.046) | 0.8(0.043) | 0.702(0.021) |
| HCU-cities | 0.619(0.106) | 0.607(0.065) | 0.705(0.049) | 0.702(0.047) | 0.713(0.047) | 0.686(0.025) |
| HCU-rural | 0.548(0.043) | 0.65(0.048) | 0.662(0.057) | 0.677(0.059) | 0.803(0.051) | 0.646(0.023) |
| GP care | 0.167 (0.03) | 0.128(0.027) | 0.276(0.036) | 0.25(0.035) | 0.252(0.035) | 0.214(0.015) |
| Specialist care | 0.122 (0.026) | 0.224(0.033) | 0.224(0.033) | 0.237(0.034) | 0.271(0.036) | 0.216(0.015) |
| HW care | 0.256(0.035) | 0.263(0.035) | 0.179(0.031) | 0.186(0.031) | 0.206(0.033) | 0.218(0.015) |
| Insured | 0.576(0.042) | 0.667(0.04) | 0.686 (0.04) | 0.704(0.039) | 0.76(0.038) | 0.677(018) |
The estimated average of health care utilization (standard error) with regard to sex, living area and insurance in the household economic quintiles of Markazi province, Iran, 2008.
The C index and OR for overall HCU and regarding sex, living area, and type of HCU are summarized in Table 2. The C index for overall HCU was obtained as 0.053 (−0.059, 0.165). The corresponding concentration curve of the overall HCU is also depicted in Figure 1. Moreover, regarding female, male, and urban as well as rural area and insured people, the C index for HCU was calculated as 0.049, 0.065, 0.025, 0.068 and 0.048 respectively. Therefore, the size of the poor–rich inequity in the HCU was higher in males and the people living in the rural areas. However, the confidence interval for the C index also demonstrated that the inequity in the HCU, regarding sex and living area variables, was not statistically significant. Moreover, subgroup analysis, considering the type of HCU, showed that the C indexes of using GP and specialist care were 0.11 (0.09, 0.12) and 0.11 (0.01, 0.13), respectively. Also, the C index for using HW was −0.06 (−0.08, −0.05). The C index for the insured subject was measured at 0.048 (−0.074 to 0.17), which shows that there is no evidence of a difference between socio-economic groups regarding HCU. The results of this study, based on the OR, are presented in Table 2. The findings showed that the overall HCU in the two highest quintiles was 74% more than the two lowest quintiles. In addition, using specialist and GP care in the two richest quintiles was 63% and 93% higher, while using HW care was 30% lower.
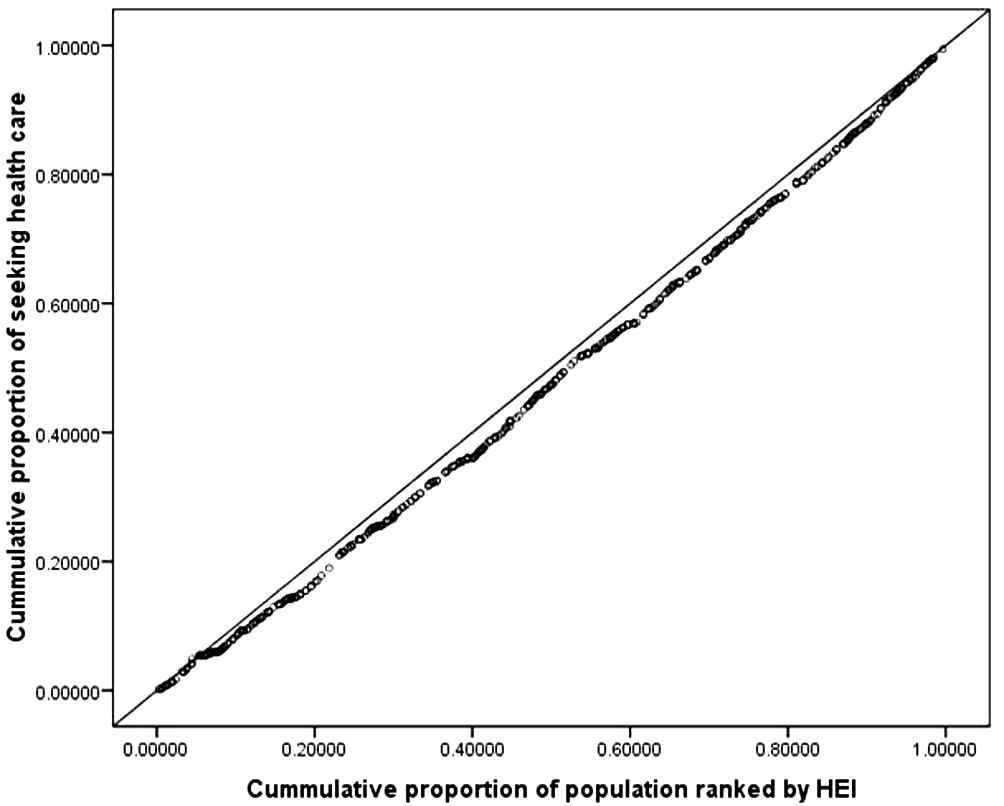
The concentration curve of the overall health care utilization in Markazi province, Iran, 2008.
| Number of subjects | Concentration index (C) | Confidence interval of C | Odds ratio (OR) Q4,Q5/Q1,Q2 | Confidence interval of OR | ||
|---|---|---|---|---|---|---|
| HCU | Overall | 779 | 0.053 | (−0.059 to 0.165) | 1.74 | (1.4 to 2.08) |
| Types of HCU | GP care | 167 | 0.109 | (0.094 to 0.124) | 1.93 | (1.53 to 2.34) |
| Specialist care | 168 | 0.115 | (0.0998 to 0.131) | 1.63 | (1.23 to 2.02) | |
| HW care | 171 | −0.065 | (−0.084 to −0.046) | 0.70 | (0.32,1.07) | |
| No seeking | 273 | 0 | 0 | |||
| HCU-sex | Female | 466 | 0.049 | (−0.10 to 0.20) | 1.76 | (1.31 to 2.22) |
| Male | 333 | 0.065 | (−0.10 to 0.23) | 1.9 | (1.39 to 2.41) | |
| HCU-living area | City | 353 | 0.025 | (−0.14 to 0.19) | 1.54 | (0.99 to 2.1) |
| Rural | 426 | 0.068 | (−0.088 to 0.224) | 1.96 | (1.48 to 2.44) | |
| HCU-insurance | Insured | 678 | 0.0478 | (−0.074 to 0.17) | 1.66 | (1.29 to 2.02) |
Estimated concentration index, odds ratio and their confidence interval of health care utilization with regard to the subgroup analysis in Markazi province, Iran, 2008.
4. Discussion
The results of this study showed that a high percentage of subjects (97.7%) who sought outpatient care used it. Therefore, seeking outpatient care is considered as HCU [14]. The results of the present study showed an increasing trend among the poorest to the richest quintiles in the overall HCU and regarding sex and living area of subjects as well as insured people. Also, the pattern of using GP and specialist care was upward from poor to rich quintiles. On the other hand, HW care had approximately a decreasing trend. In addition, the present study quantified the size of the inequity in HCU in one of the central provinces of Iran. Based on the results, there is no evidence of inequity in HCU at the first glance. Although the C index of HCU was equal to 0.053 and is not statistically different from zero, the results of another study that was performed on HCU in Iran in 2002 showed that the C index varied from 0.047 to 0.78 [25]. Therefore, it is clear that the size of the inequity in the Markazi province is lower than the average of the country, and it is not statistically significant. Therefore, it can be claimed that the overall outpatient care utilization is equal among different people with different socioeconomic classes. However, these results showed that the referring pattern for using the care is different among high-income and low-income people. Since 2005, family physicians and rural insurance have extended the health insurance coverage and people’s access to health care in Iran, respectively. In addition, introducing the hospital insurance to the un-insured urban population increased the share of the insured population up to 30% in rural and 10% in urban areas [30]. These programs, alongside the primary health care services, increase the people’s access to health care in the poor or mid-quintiles and, consequently, decrease the inequity.
The results of other studies also demonstrated the socioeconomic inequity in health [2,5,15,17,19]. For example, van Doorslaer and Koolman showed significant inequities in health utilization in higher income groups in European countries, particularly in Portugal, the UK, and Denmark. Their work showed that the health utilization index varied from 0.0034 in the Netherlands to 0.0218 in Portugal among the European countries. According to the results of the present study, inequity in HCU in the Markazi province, Iran, is twofold higher than Portugal, which has the highest concentration index in Europe. Moreover, malnutrition, and infant mortality inequity is higher in lower socioeconomic quintiles in different countries [15,16]. Furthermore, Kushel et al. showed that having health insurance is related to greater use of ambulatory care and increased usage of care by 2.6-fold of people without insurance [17]. The results of another study that was conducted by Hosseinpoor et al. in 2000 [15]showed that the inequity in the Markazi province was higher than the average of Iran and other central provinces. In that study, the C index was measured as −0.1996 and −0.1789 for the Markazi province and the whole country, respectively. These results reveal the infant mortality rate in poor quintiles to be higher than rich quintiles. Besides, in the present study, the C index for overall HCU gained a positive value and showed that rich people use health care more. Therefore, the results of the two studies are the same, and it seems that the people in the poorest quintiles have lower HCU and higher infant mortality rate.
The subgroup analysis, based on the type of HCU, showed evidences of inequity in the three types of health care: GP, specialist and HW care. In addition to the existence of the inequity in the types of HCU according to statistical inference of confidence interval, the pattern of the inequity in the three types was also different. Using GP care and specialist care is more concentrated in rich people, while using HW care is more common in poorer individuals. On the other hand, people in the highest quintiles use specialist and GP care more, while those in the lowest quintiles prefer to refer to HWs. This difference in the pattern of HCU is due to the structure of rural insurance and family physician programs because using the rural insurance is conditional to being referred to specialists by family physicians or HWs. Moreover, a rapid increase in health expenditure from GDP has recently occurred in Iran; based on the World Health Organization report, the cost of health increased from 5.3% of GDP in 1996 to 7.8% in 2006 [31].
The results of the present study showed that the only source of inequity in HCU is the type of health care used. Other studies [5,17,18,25,30], however, revealed sex, location of residence, and insurance as the main predictors of inequity. Stratification analysis, according to these variables, showed that with regard to male and female, rural and urban, and insured people there is no evidences of a significant poor–rich inequity, although rich people used the health care more. On the other hand, stratification, based on the types of HCU, showed that people in different HEI quintiles varied regarding the use of specialist, GP and HW care. Another study in the USA also showed that the form of inequity in HCU has changed in developed countries in a way that people in higher-income groups use specialist services more, while the lower-income groups use general physician care more [6]. Therefore, the pattern of the inequity in HCU in Iran is the same as the developed countries.
However, different studies employ various methods for construction of socioeconomic status. Therefore, the differences observed among countries or in different periods of time may be the result of different wealth and asset indexes used in different studies. In addition, constructing the HEI by the PCA is a recommended method which has been continually used in a great number of studies on health inequity [3,27,28]. Following this recommendation may be helpful for comparing the inequity indexes obtained in different countries as well as local places. Moreover, it is obvious that the problem of health inequity will not be solved by increasing the investment and modern technologies in the health system. Nevertheless, precise and practical strategies are needed in order for this problem to be solved. In fact, the inequity in health has its roots in socioeconomic status and other determinants of health. Therefore, deprivation of people who live in unfavorable conditions and urban margins from health services leads to the inequity in health [32]. Moreover, another important issue in inequity in health care is the nature of self-reported need. It may be time to reflect individuals’ preferences and tastes, especially in lower income groups, so other indexes such as number of contacts can be helpful in these studies [33].
5. Conclusion
Although the crude measure of C in this study did not show any significant evidence of inequity in HCU, the stratification analysis demonstrated a significant inequity in the types of HCU in the poor–rich quintiles. The people in higher HEI used specialist care more, while those in the lower HEI used HW care more. In the present study, no evidence of inequity was observed in HCU among poor–rich quintiles of males and females, people living in rural and urban areas, and insured people.
Author’s contribution
A.MB.; PhD student of epidemiology, working and analyzing of data and interpretation of the results, coworker in draft of article.
J.H.; Main advisor of the research, contributing to other authors in analyses and translating the article into English.
B.E.; Co-author in designing and data collection and preparing the draft of the article.
A.R; Co-author in improving the English translation of the manuscript and preparing the draft of the article.
7. Financial support
Shiraz University of Medical Sciences.
8. Conflict of interest
None.
Acknowledgments
The authors would like to thank the Shiraz University of Medical Sciences, Department of Research, for financially supporting this work (contract No. 90-5902), as well as all the engaged staff in Markazi Province, Department of Health, who cooperated in the process of data collection. The authors are also grateful to the Research Improvement Center of Shiraz University of Medical Sciences and Ms. A. Keivanshekouh for their cooperation in improving the use of English in the manuscript.
References
Cite this article
TY - JOUR AU - Abolfazl Mohammadbeigi AU - Jafar Hassanzadeh AU - Babak Eshrati AU - Abbas Rezaianzadeh PY - 2013 DA - 2013/04/19 TI - Socioeconomic inequity in health care utilization, Iran JO - Journal of Epidemiology and Global Health SP - 139 EP - 146 VL - 3 IS - 3 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2013.03.006 DO - 10.1016/j.jegh.2013.03.006 ID - Mohammadbeigi2013 ER -