
Pilot use of a novel smartphone application to track traveller health behaviour and collect infectious disease data during a mass gathering: Hajj pilgrimage 2014
Joint first author.
- DOI
- 10.1016/j.jegh.2015.07.005How to use a DOI?
- Keywords
- App; Hajj; Infectious disease; Mass gathering; Smartphone; Traveller
- Abstract
This study examines the feasibility of using a smartphone application (app) to conduct surveys among travellers during the Hajj pilgrimage, where the use of apps has not been evaluated for infectious disease surveillance. A longitudinal study was conducted among pilgrims at the Hajj 2014 using an iPhone app with separate questionnaires for three study phases covering before, during, and after Hajj. Forty-eight pilgrims from 13 countries downloaded the app. Respondents were aged between 21 and 61 (median 36) years and 58.5% (24/41) were male. Of these, 85% (41/48) completed the first phase, 52% (25/41) completed both the second and third phases, and 25 of these reported meningococcal vaccination, with 36% (9/25) receiving other vaccines. All (25) reported hand hygiene use and 64% (16/25) wore a facemask at some point during the pilgrimage. Four (6%) reported close contact with camels. Respiratory symptoms commenced from the 4th day of Hajj, with sore throat (20%) and cough (12%) being the most common. Three participants (12%) reported respiratory symptoms after returning home. Conducting a prospective survey using a smartphone app to collect data on travel-associated infections and traveller compliance to prevention is feasible at mass gatherings and can provide useful data associated with health-related behaviour.
- Copyright
- © 2015 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
1. Introduction
The annual Hajj pilgrimage to Mecca, Saudi Arabia, is a striking example of intensely crowded human activity where 2–3 million pilgrims assemble from over 180 countries. Incidence of acute respiratory tract infections (ARI) is high [1,2]. Moreover, emergence of Middle East respiratory syndrome coronavirus (MERS-CoV) in Saudi Arabia and other countries poses a new public health challenge [3]. In order to reduce the risk of ARI among Hajj pilgrims, the Saudi Arabian health authority recommends a range of infection control measures [4], however, compliance to these measures is highly variable [5–8]. Several studies have addressed pilgrim knowledge, attitude, and practice (KAP) towards preventive measures and infectious diseases, finding that their understanding about the potential severity of respiratory infection and the need for protective measures was inadequate [8–13]. Gautret et al. [9] found that <50% of French pilgrims were aware of social distancing, available treatment options, and facemask use as precautionary measures against the spread of respiratory infections. Other studies assessed pilgrim knowledge of emerging infections, such as MERS-CoV and Ebola, and found that 60% of pilgrims were not aware of MERS-CoV circulation in Arabia and about 40% had no accurate knowledge of Ebola transmission. However, longitudinal studies examining these questions before, during, and after travel are lacking.
Conducting longitudinal studies among travellers during mass gatherings involves many challenges, including requirements of a large sample size and high response rate, as well as continuous follow up throughout the course of travel with real-time data capturing. Conducting such studies using conventional “pen and paper”-based methods requires significant time and resources.
Smartphones are increasingly becoming an integral part of modern life, making it possible to conduct prospective surveys among Hajj pilgrims through their use. Several studies have demonstrated their usefulness in conveying health messages in a variety of contexts and audiences, with high response and retention rates and fewer data-entry errors during descriptive studies and randomised controlled trials [14,15]. Thus, smartphones may provide better platforms to conduct prospective surveys among Hajj pilgrims than conventional “pen and paper”-based methods [14–18]. Additional advantages include constant internet connection, location-detection services, and user proximity making it an ideal tool for collecting infectious disease data during mass gatherings. Data concerning smartphone usefulness in infectious disease research at mass gatherings are very limited [19]. Therefore, we conducted a pilot study using a smartphone app to examine its feasibility to track not only Hajj pilgrim KAP regarding preventive measures, but also symptom onset and participation in high-risk activities before, during, and after Hajj 2014.
2. Methods
2.1. Study design
A prospective cohort study was conducted among Hajj pilgrims at three time points, including before, during, and after Hajj 2014 (between September 5th and October 30th). This involved using three sets of questionnaires in English, including a pre-Hajj questionnaire composed of 23 questions, seven identical pages of Hajj questionnaires (containing five questions per questionnaire) each to be completed daily over a week during the peak Hajj period, and a post-Hajj questionnaire composed of six questions. We developed an iPhone application (app) called ‘Hajj Health Diary’, utilising the ‘Health Monitor’ app template [20] and released it in the Apple app store on September 5, 2014. Users started by registering their device in our online secure research database and were assigned a unique identifier for their device. This method was used successfully in previous studies [15,16,21]. The app determined user location through the smartphone location service and recorded it in our research database each time the participant used it.
This study and the materials described below were approved by the Human Research Ethics Committee at The University of Sydney (Project No: 2014/599). The terms and conditions of downloading the app were communicated before obtaining participant consent.
2.2. Participants
Participants aged 18 years and older and participating in the 2014 Hajj pilgrimage in Mecca were included. Attendance was confirmed by tracking their location during Hajj. Participants aged less than 18 years or whose stay in Mecca during the Hajj period could not be confirmed through location-tracking services were excluded from the study.
2.3. The app content
The app consists of three main screens (Fig. 1) and an ‘about’ screen, which includes the participant information sheet and consent form. The first screen (first phase) is the pre-Hajj questionnaire, including data on participant demographics, pre-existing chronic diseases, vaccinations received before travel, factors influencing vaccination decision and uptake, perception of the risk of respiratory infection during Hajj, willingness to participate in high-risk activities, such as drinking unpasteurised milk, and awareness of official health recommendations provided by Saudi Arabian authorities. This phase lasted from September 5 to 30, 2014.
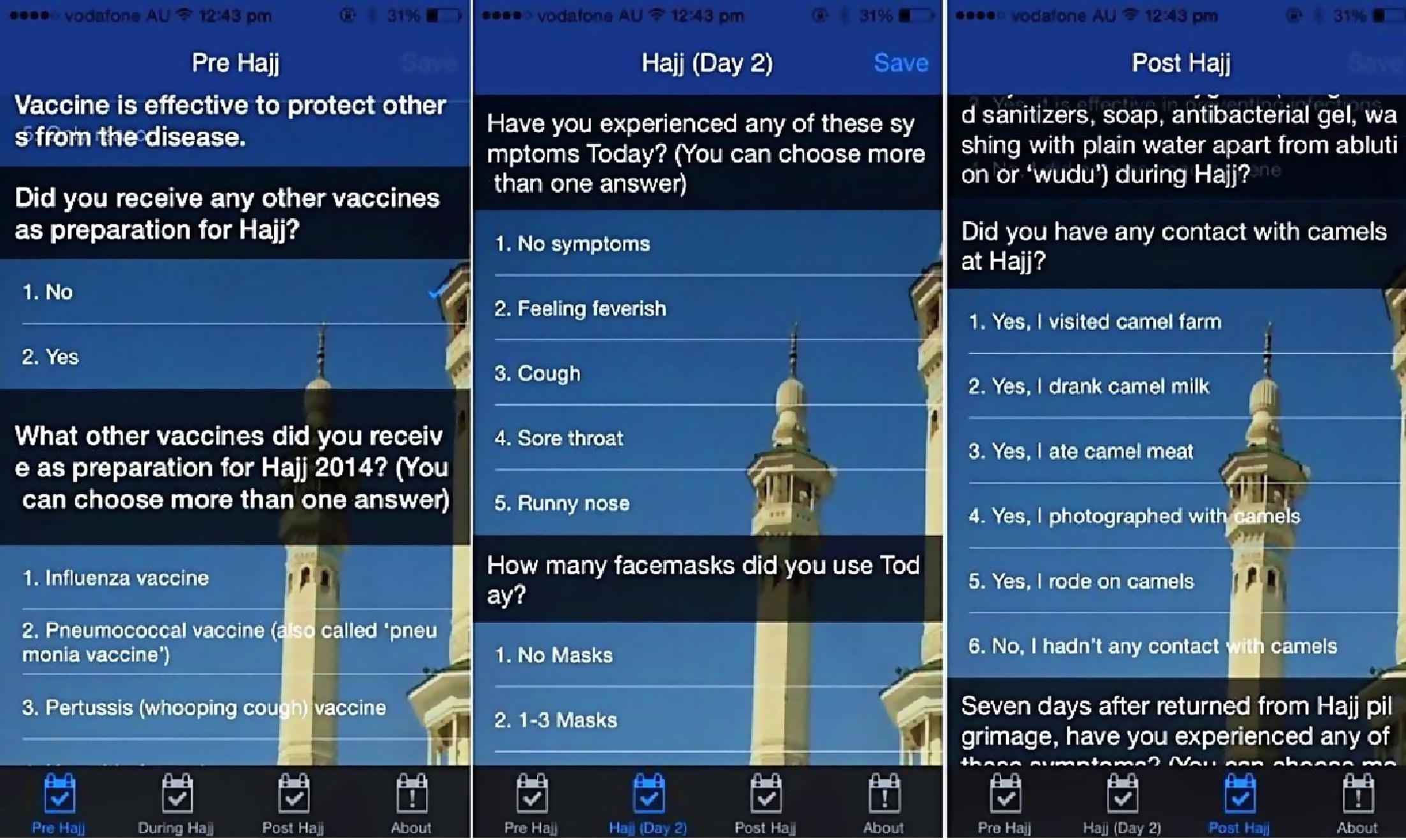
Screenshots of the “Hajj Health Diary” application.
The second screen (second phase) included the Hajj questionnaire, which consisted of seven pages of identical questionnaires, one page for each day of the ‘peak’ Hajj period. These questionnaires asked about development of respiratory symptoms and their adherence to preventive measures. Given that the ‘peak’ Hajj period in 2014 lasted from October 1 to 7, the app pushed a local notification each day to the user to complete the questionnaire. If the user did not complete it on the same day, they were reminded to do it the next time they opened the app. Therefore, the first default questionnaire needed to be completed first before going to the next. The participant could not start completing the Hajj questionnaire before completing the pre-Hajj questionnaire and not before October 1, 2014.
The third screen (third phase) includes a post-Hajj questionnaire, including questions about participant use of infection prevention methods, involvement in high-risk activities, and development of ARI symptoms 1 week after the conclusion of Hajj. As the Hajj pilgrims usually spend up to 2 weeks in Saudi Arabia before returning to their home countries, the app pushed a daily reminder to complete the post-Hajj questionnaire from October 15 to 30, 2014.
If the participant did not have an Internet connection, data were stored locally on the device and automatically transferred to our database as soon as an Internet connection was available. To understand usage behaviour, we also collected data entry date and time and transferred it to the database. Participants had to complete all questions before submitting any of the questionnaires and could not submit any questionnaire more than once, even if they deleted and re-installed the app.
2.4. Recruitment
We used both active and passive recruitment strategies. First, we recruited Australian pilgrims through distribution of brochures during pre-Hajj travel seminars in Sydney. Second, we released the app to the Apple app store globally (and exclusively), expecting that some users searching for Hajj-related apps would find it. This was likely given that our app was the only one that would appear under the search term ‘Hajj health’ in that outlet. In the pretravel questionnaire, we included a question on how the participants heard about the app.
2.5. Identifying and tackling potential challenges
We identified a priori that there might be potential challenges, including loss of Internet connection, app de-installation and re-installation, advertent or inadvertent omission of survey questions, and failure to follow the recommended order while completing the surveys. To minimise these pitfalls, the following measures were taken:
- •
If the participant lost the Internet connection, the data would be stored locally on the device and transferred to our database as soon as the Internet connection became available.
- •
If the participant de-installed the app and re-installed it, the app would not allow resubmission of the same questionnaire, requiring the participant to start from where they finished before de-installing the app. This would also maintain the sequence of questionnaire completion.
- •
To avoid any omission or delay in completing the questionnaires, the app would push a daily reminder to complete the current survey.
3. Results
3.1. App utilisation
The app was downloaded by 48 pilgrims from 13 countries (Table 1). Of them, 85% (41/48) completed the first phase (pre-Hajj questionnaire) and of those, 61% (25/41) completed all three study phases (Fig. 2). Of the 41 participants who completed the pre-Hajj questionnaire, 28 (68.3%) opened the app in Saudi Arabia at least once while having Internet connection.
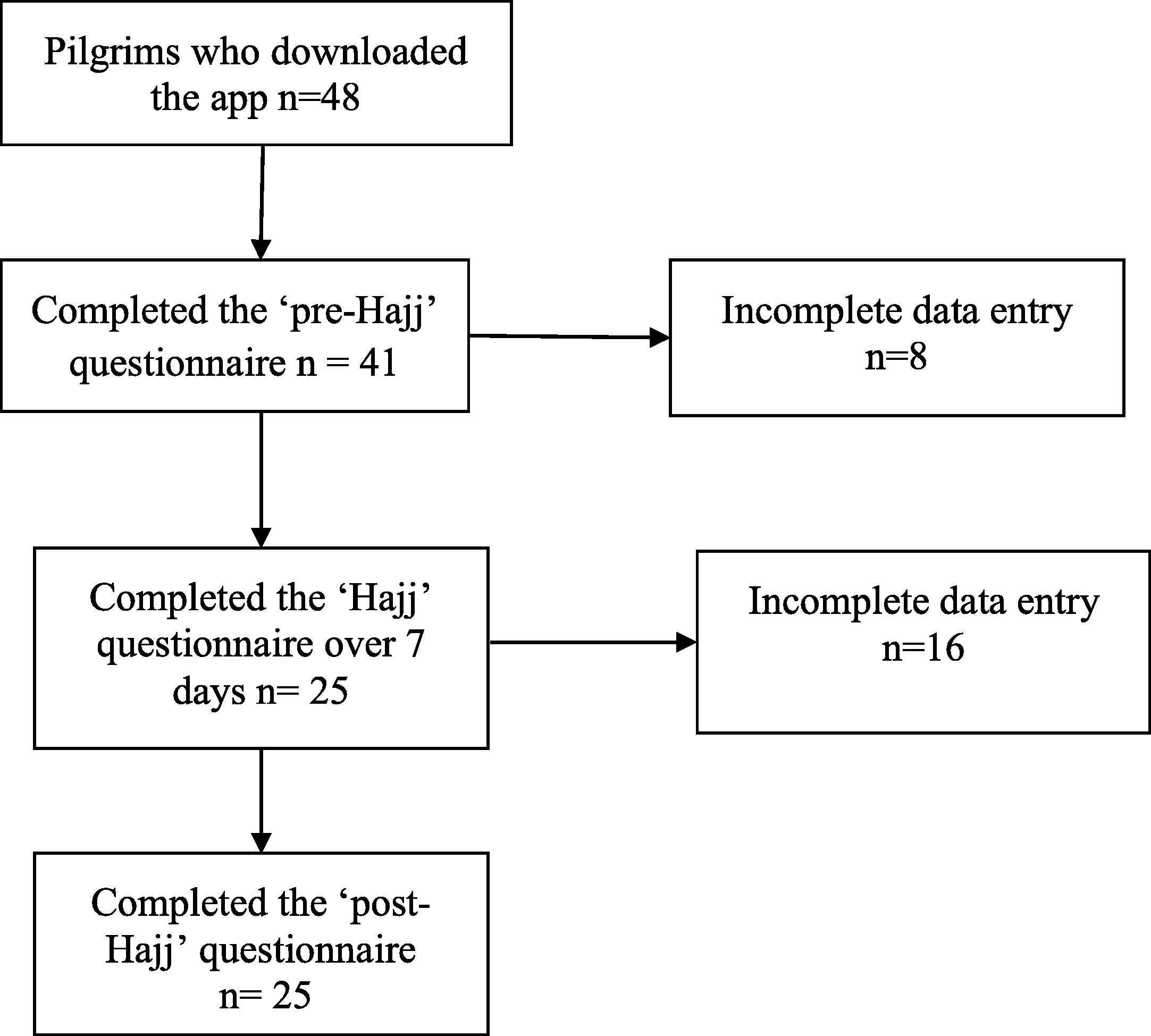
Flowchart showing response rates of participants during each study phase.
| Country | Downloads N | Completed pre-Hajj survey n (%) | Completed Hajj survey n (%) | Completed post-Hajj survey n (%) |
|---|---|---|---|---|
| United States | 17 | 15 (88.2) | 12 (70.6) | 12 (70.6) |
| Australia | 12 | 12 (100) | 6 (50) | 6 (50) |
| Russia | 4 | 3 (75) | 1 (25) | 1 (25) |
| France | 3 | 1 (33.3) | 1 (33) | 1 (33) |
| United Kingdom | 3 | 3 (100) | 2 (66.7) | 2 (66.7) |
| Canada | 2 | 2 (100) | 1 (50) | 1 (50) |
| India | 1 | 1 (100) | 0 (0) | 0 (0) |
| Azerbaijan | 1 | 0 (0) | 0 (0) | 0 (0) |
| South Africa | 1 | 1 (100) | 1 (100) | 1 (100) |
| Saudi Arabia | 1 | 1 (100) | 0 (0) | 0 (0) |
| China | 1 | 0 (0) | 0 (0) | 0 (0) |
| Hong Kong | 1 | 1 (100) | 0 (0) | 0 (0) |
| United Arab Emirates | 1 | 1 (100) | 0 (0) | 0 (0) |
| Total | 48 | 41 (85) | 25 (52) | 25 (52) |
Downloads and response rates by country.
The respondents were aged between 21 and 61 (median 36) years and 58.5% (24/41) were male. A large portion (46.3%, 19/41) was university educated and 80.5% (33/41) were employed. Sixteen (39%) participants had pre-existing chronic diseases, including five with diabetes (12.2%), three each with hypertension, bronchial asthma, and hypercholesterolemia (7.3%), and one with heart disease (2.4%). The participants stayed in Mecca for a median of 14 days (range, 9–30 days), 70.7% (29/41) attended Hajj for the first time, and only 9.8% (4/41) were aware of annual Saudi Arabian health recommendations for Hajj pilgrims.
In terms of how the participants heard about the app, 41.5% (17/41) reported first seeing it in the Apple app store, 19.5% (8/41) heard about it in pre-Hajj seminars, 12.2% (5/41) from the study researchers, and 26.8% (11/41) from other sources.
Regarding convenience of using the app, 53.6% (22/41) found it very convenient, 31.7% (13/41) found it slightly convenient, 9.8% (4/41) found it a little inconvenient, and 4.9% (2/41) found it very inconvenient. Those who found it inconvenient (to any degree) left the survey incomplete.
Concerning usage behaviour, the number of participants who completed the Hajj questionnaire on the day the reminder was pushed, i.e., the 1st day, was 31, but dropped to 27 on the 2nd day and remained at 25 from the 3rd day onward (Fig. 2). Those who did not complete the Hajj questionnaire on the specified day completed it within the next 1–6 days. All participants who completed the Hajj questionnaire subsequently also completed the post-Hajj questionnaire.
3.2. Traveller knowledge, attitude, and practice
Of those who completed the study phases, all reported receiving the compulsory meningococcal vaccine. The main factors driving meningococcal vaccine uptake were severity of the disease 80% (20/25) and effectiveness of the vaccine 76% (19/25). Only 9 (36%) pilgrims received other vaccines before Hajj (8 had influenza vaccine and one pneumococcal vaccine). Three of these had comorbidities.
Forty-four percent (11/25) of participants were unconcerned about catching influenza while at Hajj and 76% were unconcerned about developing a cough. Forty percent (10/25) of respondents expressed concern about contracting MERS-CoV during Hajj, at least to a modest extent, while the rest did not. However, 36% (9/25) of participants were willing to visit a camel farm during Hajj and 16% (4/25) were willing to drink unpasteurised camel milk if offered in Saudi Arabia. In practice, 16% (4/25) of pilgrims (2 American, 1 Canadian, and 1 Australian) actually reported coming into contact with camels, including visiting a camel farm, taking photographs with camels, and drinking their milk (2).
The onset of respiratory tract symptoms began from the 4th day of the peak Hajj period and continued over the next several days. Sore throat (20%) and cough (12%) were the most frequently reported symptoms (Fig. 3). After returning home from Hajj, 12% (3/25) of participants reported developing a cough and sore throat within 1 week and, among these, one pilgrim from Australia reported having had contact with camels during Hajj.
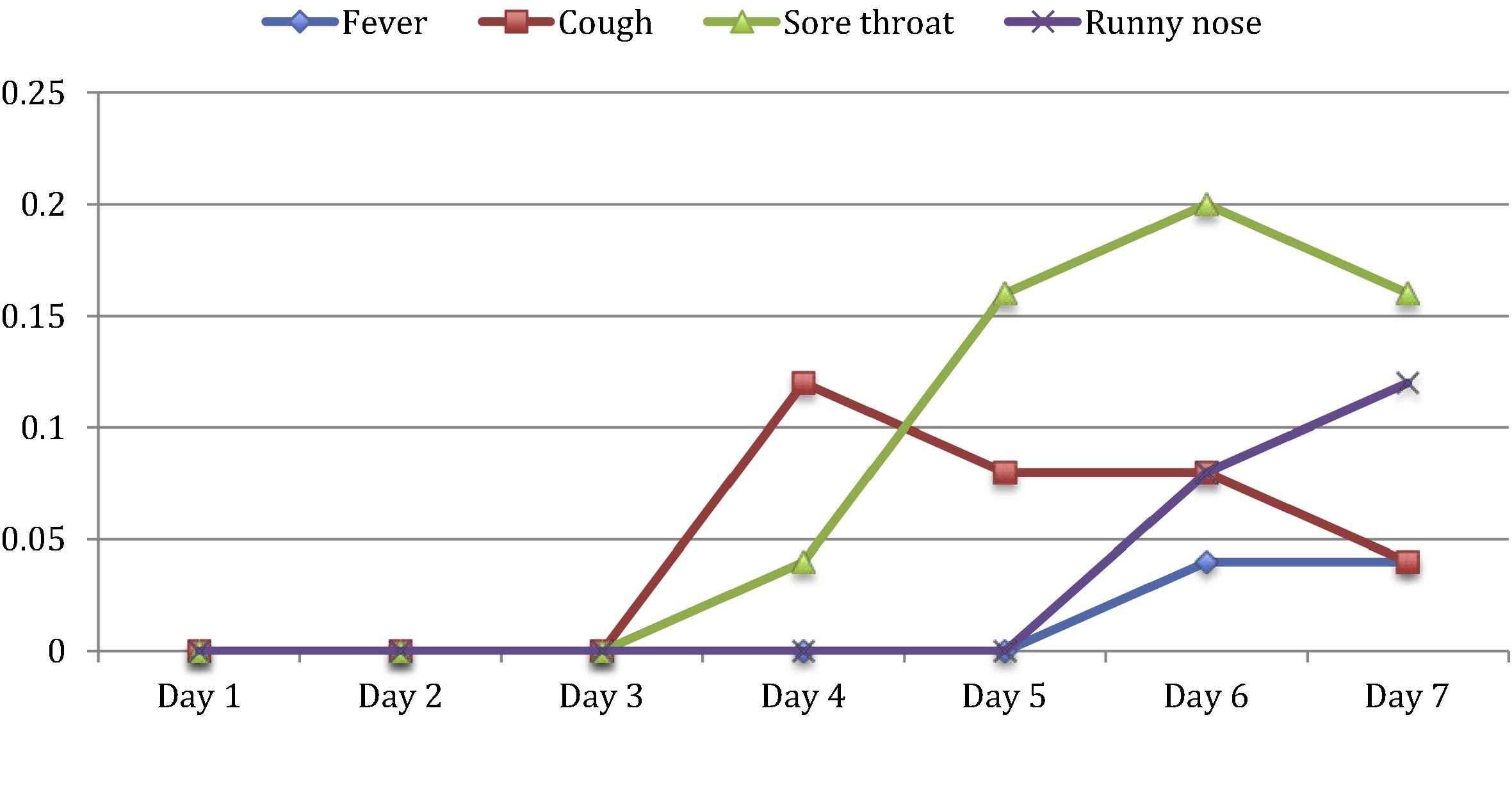
Onset of respiratory symptoms according to the days of Hajj.
Sixty-four percent (16/25) reported wearing a facemask during Hajj, with uptake highest on Day 4 (Table 2). Protection from infectious agents and air pollutants was the main reason for mask use. Difficulty in breathing and a feeling of suffocation were commonly cited as barriers to the use of facemasks. On the other hand, all participants practiced hand hygiene at some point (mostly during the 1st 4 days) during Hajj. Respondents stated that hand hygiene was easy to implement, convenient, and believed it to be effective in preventing infections.
| Preventive measures | Day 1 n/N (%) | Day 2 n/N (%) | Day 3 n/N (%) | Day 4 n/N (%) | Day 5 n/N (%) | Day 6 n/N (%) | Day 7 n/N (%) |
|---|---|---|---|---|---|---|---|
| Facemask | 14/31 (45.2) | 14/27 (51.8) | 15/25 (60) | 19/25 (76) | 15/25 (60) | 13/25 (52) | 17/25 (68) |
| Hand hygiene | 11/31 (35.5) | 12/27 (44.4) | 13/25 (25) | 15/25 (60) | 16/25 (64) | 11/25 (44) | 7/25 (28) |
| Disposable handkerchiefs | 14/31 (45.2) | 16/27 (59.2) | 15/25 (60) | 12/25 (48) | 12/25 (48) | 17/25 (68) | 11/25 (44) |
| Avoiding ill people | 6/31 (19.4) | 4/27 (14.8) | 5/25 (20) | 7/25 (28) | 9/25 (36) | 6/25 (24) | 2/25 (8) |
| Avoiding crowded places | 5/31 (16.1) | 3/27 (11.1) | 6/25 (24) | 9/25 (36) | 12/25 (48) | 7/25 (28) | 1/25 (4) |
| Total number | 31 | 27 | 25 | 25 | 25 | 25 | 25 |
Traveller compliance to non-pharmaceutical measures during the Hajj week.
4. Discussion
Overall, this pilot study indicates that conducting a prospective survey using a smartphone app to collect data on travel-associated infections and traveller compliance to prevention is feasible, given that the response rate was >50%. This survey also demonstrates that many pilgrims partake in activities that may increase risk of acquiring emerging infections.
Of the 48 people who downloaded the app, 41 (85%) participated in the first survey and of these, 25 (61%) went on to complete it. Previous paper-based cross-sectional surveys reported response rates ranging between <20% and >80% [7,22,23]. The studies with high response rates involved recruitment with continuous follow up of worshippers throughout their pilgrimage. This approach requires significant resources and greater investment of time and cost [22,23]. Other paper-based surveys where pilgrims were not followed up continuously had response rates as low as 19.7% [7]. The strengths of our study include its low cost, ability to reach far and wide to allow real-time analyses and longitudinal follow-up, and ability to capture data daily during the peak Hajj period, something not accomplished in other studies.
This pilot survey reveals that all pilgrims complied with hand hygiene. This is supported by a review by Benkouiten et al. [24], which found that hand hygiene was the most popular non-pharmaceutical preventive measure among Hajj pilgrims. Ease of use and participant belief regarding its effectiveness against infection were important driving factors.
In this study, we found that respiratory symptoms commenced on the 4th day of tent stay during Hajj and continued thereafter, with cough and sore throat being the most commonly reported symptoms. This is likely because the incubation period of most commonly circulating respiratory viruses is about 1–4 days [25]. Used in combination with a geographic information system as a tool for syndromic surveillance, this novel method can be used to detect real-time clusters of respiratory infections at Hajj and other mass gatherings.
Although MERS-CoV has been circulating in Saudi Arabia since 2012, no case of Hajj-associated MERS-CoV has been reported [26]. Evidence suggests that MERS-CoV can be transmitted to humans through close contact with an infected camel [27]. Interestingly, our study identified that some pilgrims had close contact with camels, including visiting camel farms, photo opportunities with camels, and drinking their raw milk. Through this survey, we identified one Australian pilgrim who had close contact with camels and subsequently developed respiratory symptoms within 1 week of returning home. Further follow up of the case was not possible, however, given that no MERS-CoV case was reported in Australia, it is highly unlikely that the person had MERS-CoV. Therefore, this pilot study suggests that smartphones could help detect patients with potential emerging infectious diseases.
Electronic surveillance to identify outbreaks of infectious diseases at a mass gathering has been attempted previously [28]. For instance, surveillance using electronic medical records deployed during the 2002 Winter Olympic Games helped detect an influenza outbreak, which was subsequently described with the aid of laboratory diagnosis [29,30]. Digital interfaces, including smartphones, were applied at the 2012 London Olympics to identify illnesses and injuries among athletes [31]. Our study, the first of its kind at Hajj, demonstrates the feasibility of a smartphone app in a prospective survey of pilgrim illness and adherence to preventive measures throughout the course of travel.
Owing to delays in development, testing, and app store approval, the app was only released a few weeks before Hajj, limiting the amount of time it was available to respondents prior to their journey. We speculate that earlier app release will result in greater numbers of participants. Because this survey was conducted only in English, multilingual applications could have expanded participation into diverse language groups. Data on pilgrim demographics show that 60–80% of pilgrims are older than 40 years of age [8,32], while most smartphone users are aged 25–44 years [33], which might have impacted study outcomes. However, since smartphone use is gradually becoming ubiquitous, respondent demographics are likely to be less important in the future. Finally, we designed the app only for iPhone users, thus excluding users of other smartphone platforms, such as Android or Windows mobile. Extending availability of this app to other platforms will likely increase participation rates.
5. Conclusion
In conclusion, this pilot study demonstrates that smartphone apps can be used to conduct surveys to prospectively gather data concerning onset and progression of symptoms and location information during mass gatherings. Such data collection can potentially reinforce education associated with disease prevention behaviours, thus improving public health. A larger study with multilingual apps for both iPhone and Android smartphones is planned for Hajj 2015.
Conflicts of interest
Professor Robert Booy has received funding from Baxter, CSL, GSK, Merck, Novartis, Pfizer, Roche, Romark, and Sanofi Pasteur for the conduct of sponsored research and travel to present at conferences or consultancy work. All funding received is directed to research accounts at The Children’s Hospital at Westmead. Dr. Anita E. Heywood has received grant funding for investigator-driven research from GSK and Sanofi Pasteur. Dr. Harunor Rashid received fees from Pfizer and Novartis for consulting or serving on an advisory board. The other authors have no competing interests to declare.
References
Cite this article
TY - JOUR AU - Amani S. Alqahtani AU - Nasser F. BinDhim AU - Mohamed Tashani AU - Harold W. Willaby AU - Kerrie E. Wiley AU - Anita E. Heywood AU - Robert Booy AU - Harunor Rashid PY - 2015 DA - 2015/08/13 TI - Pilot use of a novel smartphone application to track traveller health behaviour and collect infectious disease data during a mass gathering: Hajj pilgrimage 2014 JO - Journal of Epidemiology and Global Health SP - 147 EP - 155 VL - 6 IS - 3 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2015.07.005 DO - 10.1016/j.jegh.2015.07.005 ID - Alqahtani2015 ER -