
Clinical, Imaging, and Laboratory Characteristics of Adult Mexican Patients with Tuberculous Meningitis: A Retrospective Cohort Study
- DOI
- 10.2991/jegh.k.191023.001How to use a DOI?
- Keywords
- Meningitis; tuberculosis; tuberculous meningitis; meningeal tuberculosis; Mexico; outcome
- Abstract
Tuberculous Meningitis (TBM) is the most common form of central nervous system Tuberculosis (TB), accounting for 5–6% of extrapulmonary TB cases. Nowadays, TBM continues to be a major topic in public health because of its high prevalence worldwide. This retrospective study aimed to describe the clinical, laboratory, and imaging characteristics at admission; and in-hospital outcome of adult Mexican patients with TBM. We collected data from medical records of patients aged ≥18 years diagnosed with TBM according to the uniform case definition for clinical research who were treated at Tijuana General Hospital between January 2015 and March 2018 and compared them according to the subtype of diagnosis. We included 41 cases (26 males, median age 28 years, range 18–57 years), 13 (31.7%) patients were HIV positive, and 21 (51.2%) were illicit drug users. At admission, 7 (17.1%) patients were in stage I, 22 (53.6%) in stage II, and 12 (29.3%) in stage III. A definitive diagnosis was established in 23 (56.1%) patients, probable in 14 (34.1%), and possible in four (9.8%). Molecular testing was positive in 83% of the cases, yielding significantly higher positive results than other microbiological studies. There were eight (19.5%) deaths, without statistical difference between mortality and not having a definitive diagnosis (p = 0.109). We found that the baseline characteristics of our population were similar to those described by other authors worldwide. In this series, molecular testing showed to be very useful when used in the early stages, particularly in subjects with subacute onset of headache, fever, weight loss, and altered mental status.
- Copyright
- © 2019 Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Tuberculous Meningitis (TBM) is the infection of the meninges by Mycobacterium tuberculosis (Mtb) [1]. First described by Green in 1836 [2], TBM is the most common form of central nervous system tuberculosis (TB), accounting for 5–6% of extrapulmonary TB cases and for 1% of the total TB cases worldwide [1,3,4]. TBM is described as a subacute illness with a duration of symptoms that ranges 5–30 days with clinical features such as a low-grade fever, headache, and signs of meningeal irritation; in advanced stages, there may be focal neurological deficits, cranial nerve paralysis, and seizures [1,5,6].
The global incidence of TBM is unknown [7]; in 2017, Mexico had an overall prevalence of 0.35 cases per 100,000 inhabitants [8]. The global HIV epidemic has increased the number of adults affected by TBM. Data from a study that included a database of 1699 adult patients from five different studies reported a mortality rate of 23% in non-HIV patients and 51.3% for HIV-infected patients [9], reaching 100% in cases of drug-resistant Mtb [3]. Despite its high incidence, to our knowledge, the clinical features and outcome of the Mexican adult population with TBM have not been described. The aim of this study is to describe the characteristics at admission and in-hospital outcome of adult Mexican patients with TBM and compare them according to the subtype of diagnosis.
2. MATERIALS AND METHODS
2.1. Study Design and Patient Selection
In this retrospective study, we collected from medical records the clinical, laboratory, and imaging characteristics at admission; treatment and in-hospital outcome of adult patients aged ≥18 years with suspected or confirmed TBM treated from January 2015 to March 2018 at Tijuana General Hospital, a secondary care hospital in the city of Tijuana located in the northwest region of Mexico. Cases with missing data and those having an alternate microbiological diagnosis were excluded. Demographic data; risk factors such as concomitant medical illnesses, contact with an active pulmonary TB patient, HIV status, illicit drug use; signs and symptoms at presentation like fever, weight loss, days of illness, headache, level of consciousness, cranial nerve paralysis, focal neurological signs, and seizures; Cerebrospinal Fluid (CSF) analysis; microbiology; and neuroimaging studies at presentation were registered. The Thwaites criteria, which scores five variables that include clinical features, CSF analysis, and the blood white cell count, were used to categorize the patients; a score ≤4 points was considered as a possible TBM case [10].
Diagnosis of TBM was made according to the uniform case definition for clinical research in TBM, including the following diagnostic subtypes: definitive (clinical criteria, plus Mtb detection in the CSF by any method), probable (clinical criteria plus a total diagnostic score of ≥10 points when cerebral imaging is not available or ≥12 points when cerebral imaging is available plus exclusion of alternative diagnoses), and possible (clinical criteria plus a total diagnostic score of 6–9 points when cerebral imaging is not available or 6–11 points when cerebral imaging is available plus exclusion of alternative diagnoses) [11]. Severity of the disease was graded according to the modified British Medical Research Council (BMRC) criteria; defining stage I as an alert and oriented patient without focal neurological deficits, stage II as a Glasgow Coma Score (GCS) of 11–14 or 15 with focal neurological deficits, and stage III as a GCS of ≤10 with or without focal neurological deficits [4,11]; adverse in-hospital outcome was defined as death during hospitalization or discharge. Local Ethical Committee approved this study.
2.2. Data Analysis
Demographic data, risk factors, and clinical characteristics are presented as measures of central tendency. Analyses of differences between categorical variables were performed with the Fisher’s exact test and the Mann–Whitney U test for continuous variables. A p < 0.05 was considered statistically significant. All analyses were two-tailed. Statistical calculations were performed with IBM SPSS Statistics, version 23 (IBM Corp., Armonk, NY, USA).
3. RESULTS
3.1. Epidemiological Characteristics
From January 2015 to March 2018, 54 patients were admitted with TBM diagnosis. We excluded 13 cases. Among the 41 cases we studied, there were 26 (63.4%) males and 15 (36.6%) females, and the median age at onset was 28 years (18–57 years). Twenty-four (58.5%) had at least one risk factor, 21 (51.2%) patients were illicit drug users, and 13 (31.7%) were HIV positive (Table 1).
| Variables | Total (n = 41) |
|---|---|
| Demographic characteristics | |
| Sex, n (%) | |
| Male | 26 (63.4) |
| Female | 15 (36.6) |
| Age (years), median (range) | 28 (18–57) |
| Age group (years), n (%) | |
| 18–29 | 24 (58.5) |
| 30–39 | 8 (19.5) |
| 40–49 | 5 (12.2) |
| 50–59 | 4 (9.8) |
| Risk factors, n (%) | |
| Previously treated TB | 7 (17.1) |
| HIV infected | 13 (31.7) |
| Contact with an active pulmonary TB patient | 6 (14.6) |
| Diabetes | 4 (9.76) |
| Alcoholism | 11 (26.8) |
| Use of illicit drugs | 21 (51.2) |
| Methamphetamines | 18 (43.9) |
| Marihuana | 7 (17.1) |
| IV heroin | 2 (4.9) |
TB, tuberculosis; IV, intravenous.
Demographic characteristics and risk factors
3.2. Clinical Characteristics
The median duration of illness before hospitalization was 15 days (2–234 days); the main symptoms were headache in 36 (87.8%), fever in 27 (65.9%), and weight loss in 20 (48.8%). At admission, 21 (51.5%) patients had an altered level of consciousness (GCS <15 points) with a median of 13 points (8–15 points). The most frequent clinical signs were: neck stiffness in 29 (70.7%) patients, cranial nerve paralysis in 12 (29.3%), and seven (17.1%) had focal neurological signs. According to the modified BMRC criteria, seven (17.1%) patients were in stage I, 22 (53.6%) in stage II, and 12 (29.3%) in stage III (Table 2).
| Clinical characteristics | Total (n = 41) |
|---|---|
| Days of illness, median (range) | 15 (2–234) |
| Headache, n (%) | 36 (87.8) |
| Fever, n (%) | 27 (65.9) |
| Weight loss, n (%) | 20 (48.8) |
| Persistent cough ≥2 weeks, n (%) | 16 (39) |
| Vomiting, n (%) | 15 (36.6) |
| Diaphoresis, n (%) | 12 (29.3) |
| Altered level of consciousness, n (%) | 21 (51.5) |
| Neck stiffness, n (%) | 29 (70.7) |
| Cranial nerve paralysis, n (%) | 12 (29.3) |
| III nerve | 8 (19.5) |
| VI nerve | 7 (17.1) |
| VII nerve | 4 (9.8) |
| IV nerve | 3 (7.3) |
| V nerve | 2 (4.9) |
| IX nerve | 1 (2.4) |
| Focal neurological signs, n (%) | 7 (17.1) |
| Seizures, n (%) | 8 (19.5) |
| Severity, n (%) | |
| BMRC I | 7 (17.1) |
| BMRC II | 22 (53.6) |
| BMRC III | 12 (29.3) |
BMRC, British Medical Research Council.
Clinical characteristics
3.3. Lumbar Puncture and Laboratory Findings
The opening pressure of the CSF had a median of 17 cmH2O (9–40), an elevated intracranial pressure (≥25 cmH2O) was detected in nine (22%) patients, proteins ≥100 mg/dL in 26 (63.4%), CSF/serum glucose ratio ≤0.5 in 35 (85.4%), leukocyte in the range of 10–500 mm3/mL in 32 (78%), mononuclear cells ≥50% in 29 (70.7%), and in one patient coinfection with Cryptococcus was detected; the blood workup showed hyponatremia (<135 mmol/L) in 22 (53.7%) patients (Table 3).
| CSF | |
| Proteins (mg/dL), median (range) | 146 (10–468) |
| Glucose (mg/dL), mean (SD) | 37.7 (±19.6) |
| Leukocytes (mm3/mL), median (range) | 147 (2–1167) |
| Mononuclear cells (%), median (range) | 70 (19–97) |
| Polymorphonuclear cells (%), median (range) | 30 (3–81) |
| Serum | |
| Leucocytes (×109/L), median (range) | 7.7 (1.94–21.16) |
| Sodium (mmol/L), median (range) | 133 (117–162) |
| Microbiological | |
| Test | Positive/total, n (%) |
| Direct acid-fast bacilli CSF smear | 6/11 (54.5) |
| CSF Löwenstein–Jensen culture | 7/16 (43.8) |
| CSF real-time PCR | 6/8 (75) |
| CSF Xpert MTB/RIF assay | 9/10 (90) |
| Sputum smear | 25/41 (61) |
| Gastric lavage smear | 6/11 (54.5) |
AST, aspartate aminotransferase; ALT, alanine aminotransferase; PCR, polymerase chain reaction.
Cerebrospinal Fluid (CSF), serum, and microbiological findings
3.4. Radiographic Findings
All the patients had a chest X-ray and a head Computed Tomography (CT); the chest X-ray revealed signs of active pulmonary TB in 23 (56.1%) patients; the head CT showed diffuse edema in 27 (65.8%) patients, meningeal enhancement in 19 (46.3%), hydrocephalus in 18 (43.9%), ischemia or stroke in 14 (34.1%), and tuberculomas in five (12.2%) (Figure 1).
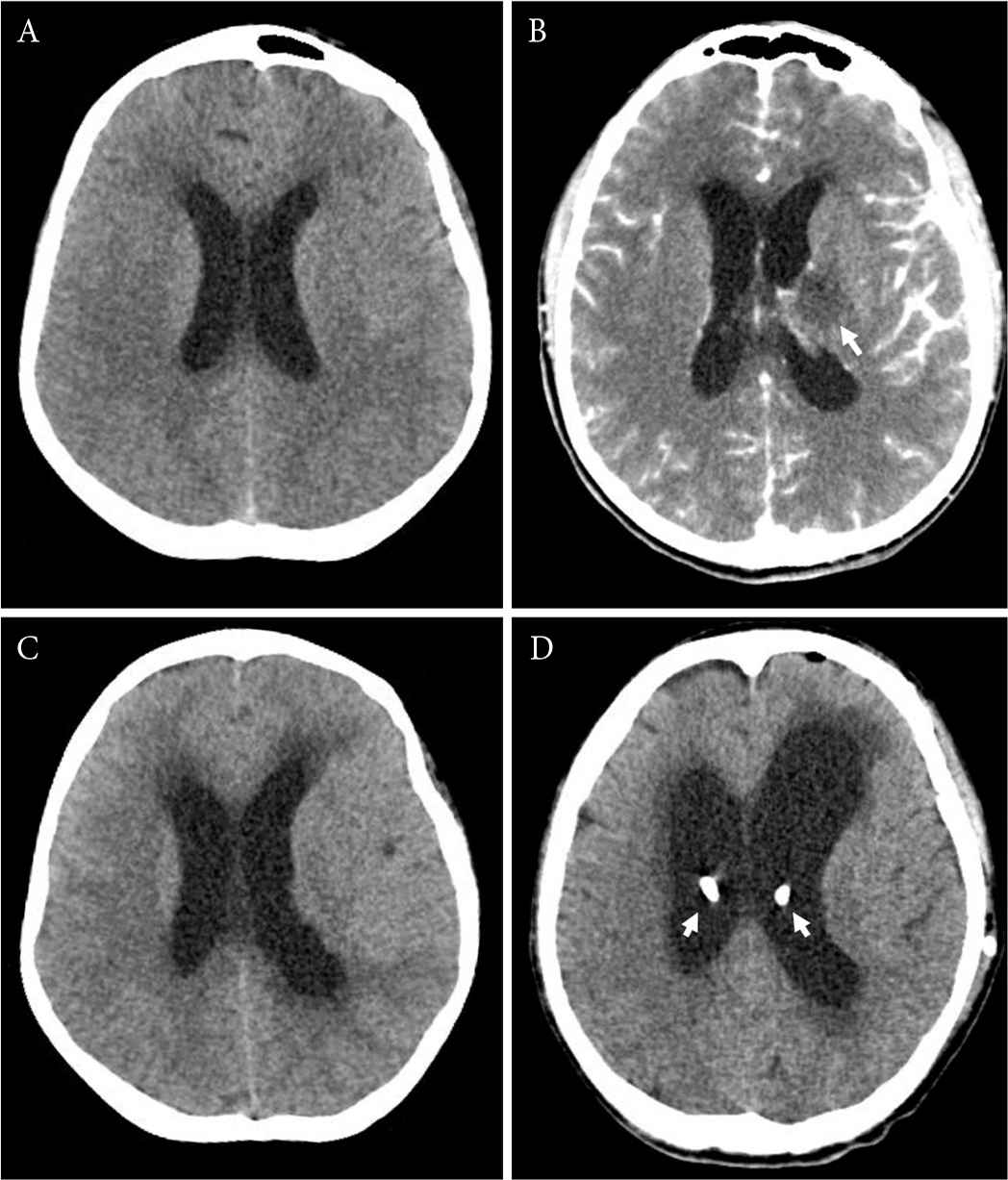
Findings on head computed tomography of patients with tuberculous meningitis. (A) Axial unenhanced head computed tomography (CT) shows diffuse brain edema. (B) Axial contrast-enhanced head CT shows an ischemic lesion near the body of the left caudate nucleus (arrow). (C) Axial unenhanced head CT demonstrates hydrocephalus and diffuse brain edema. (D) Axial unenhanced head CT shows severe hydrocephalus that required surgical treatment with a bilateral ventriculoperitoneal shunt (arrows).
3.5. Diagnostic Studies
Microbiological studies for detection of Mtb in the CSF were performed in 32 (78%) subjects, whereas molecular testing was used in 18 (43.9%) patients (Table 3). Overall, molecular testing was positive in 83% of the cases, yielding significantly higher positive results. To detect Mtb in other organs, a sputum smear was performed in 100% of the subjects but was only positive in 25 (61%). Extraneural TB was diagnosed in 26 (63.4%) patients: pulmonary in 25 (61%) and peritoneal in one (2.4%).
3.6. Type of Diagnosis
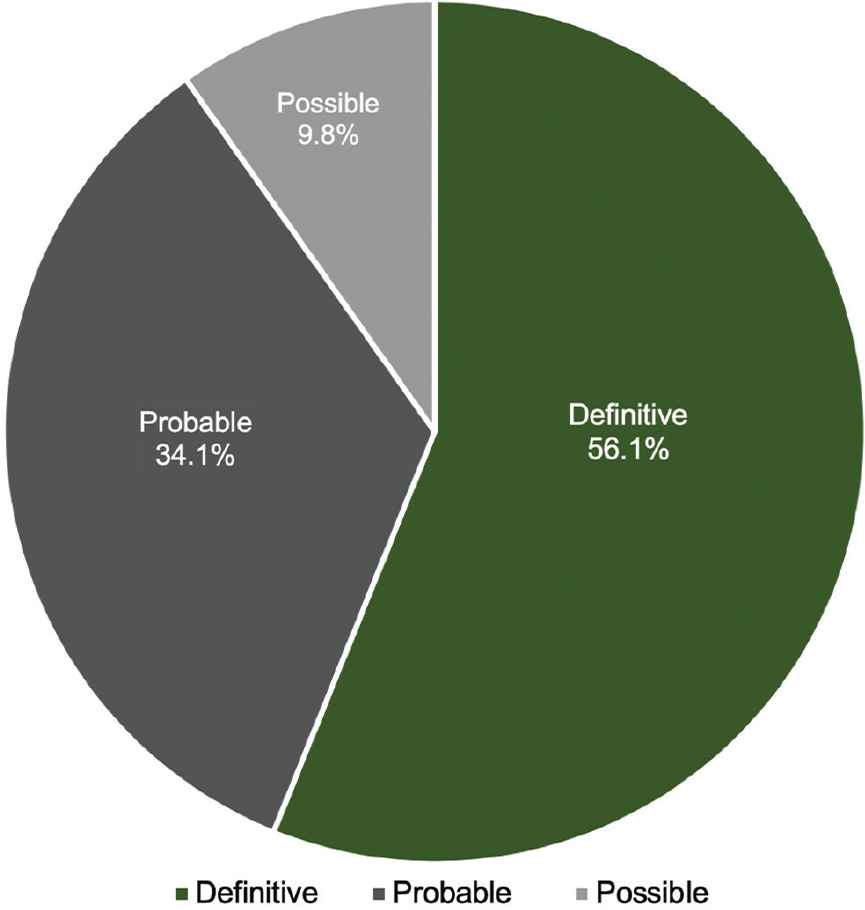
Forty (97.6%) patients fulfilled the Thwaites score criteria; the final diagnosis was classified as definitive in 23 (56.1%) patients, as probable in 14 (34.1%), and possible in four (9.8%) (Figure 2). There was no statistically significant difference between the group of patients with a definitive diagnosis and those with a positive Thwaites score (p = 0.439) (Table 4). According to the type of diagnosis, median days of illness was 26 days for the definitive diagnosis group, 16 days for the probable diagnosis group, and 4 days for the possible diagnosis group.
Type of diagnosis.
| Variables | Definitive (n = 23) | Nondefinitive (n = 18) | p-value |
|---|---|---|---|
| Demographic characteristics | |||
| Sex, n (%) | 0.004 | ||
| Male | 10 (43.5) | 16 (88.9) | |
| Female | 13 (56.5) | 2 (11.1) | |
| Age (years), median (range) | 26 (18–57) | 29 (18–53) | 0.385 |
| Risk factors, n (%) | |||
| Previously treated tuberculosis | 4 (17.4) | 3 (16.7) | 1 |
| HIV infected | 7 (30.4) | 6 (33.3) | 1 |
| Use of illicit drugs | 7 (30.4) | 14 (77.8) | 0.004 |
| Methamphetamine | 6 (26.1) | 12 (66.7) | 0.013 |
| Marihuana | 4 (17.4) | 3 (16.7) | 1 |
| Clinical characteristics | |||
| Days of illness, median (range) | 26 (2–234) | 10.5 (2–60) | 0.076 |
| Headache, n (%) | 20 (87) | 16 (88.9) | 1 |
| Fever, n (%) | 14 (60.9) | 13 (72.2) | 0.52 |
| Vomiting, n (%) | 9 (39.1) | 6 (33.3) | 0.75 |
| Altered level of consciousness, n (%) | 11 (47.8) | 10 (55.6) | 0.756 |
| Neck stiffness, n (%) | 17 (73.9) | 12 (66.7) | 0.734 |
| Cranial nerve palsy, n (%) | 7 (30.4) | 5 (27.8) | 1 |
| Focal neurological signs, n (%) | 10 (43.5) | 7 (38.9) | 1 |
| Seizures | 6 (26.1) | 2 (11.1) | 0.429 |
| Severity of disease, n (%) | |||
| BMRC I | 4 (17.4) | 3 (16.7) | 1 |
| BMRC II | 12 (52.2) | 10 (55.6) | 1 |
| BMRC III | 7 (30.4) | 5 (27.8) | 1 |
| Lumbar puncture and laboratory findings, n (%) | |||
| Hyponatremia (<135 mmol/L) | 12 (52.2) | 10 (55.6) | 1 |
| CSF opening pressure ≥25 mmHg | 6 (26.1) | 3 (16.7) | 0.706 |
| CSF proteins ≥100 mg/dL | 13 (56.5) | 13 (72.2) | 0.346 |
| Serum/CSF (glucose ratio ≤0.5) | 19 (82.6) | 16 (88.9) | 0.679 |
| CSF leukocytes 10–500 mm3/mL | 14 (60.9) | 14 (77.8) | 0.321 |
| CSF lymphocytes ≥50% | 16 (69.6) | 13 (72.2) | 1 |
| Head CT findings, n (%) | |||
| Hydrocephalus | 10 (43.5) | 8 (44.4) | 1 |
| Edema | 17 (73.9) | 10 (55.6) | 0.322 |
| Meningeal reinforcement | 10 (43.5) | 9 (50) | 0.758 |
| Tuberculoma | 4 (17.4) | 1 (5.6) | 0.356 |
| Ischemia | 12 (52.2) | 2 (11.1) | 0.008 |
| Diagnosis, prognosis and treatment, n (%) | |||
| Positive Thwaites score | 23 (100) | 17 (94.4) | 0.439 |
| Dead | 2 (8.7) | 6 (33.3) | 0.109 |
| Surgery for hydrocephalus | 9 (39.1) | 5 (27.8) | 0.52 |
| Mechanical ventilation | 3 (13) | 7 (38.9) | 0.075 |
BMRC, British Medical Research Council; CSF, cerebrospinal fluid; CT, computed tomography.
Characteristics between patients with a definitive diagnosis and nondefinitive diagnostics of tuberculous meningitis
3.7. Treatment
The time from admission to anti-tuberculosis drug initiation had a median of 2 days (0–12 days), all of the patients received corticosteroids (0.4 mg/kg/day of dexamethasone) and first-line anti-tuberculosis drugs (rifampicin, isoniazid, pyrazinamide, and ethambutol). Fourteen (34.1%) patients required surgical management of hydrocephalus; nine (21.9%) ventriculoperitoneal shunt, and five (12.1%) external ventricular drain. Ten patients required ventilatory support due to an altered level of consciousness defined as a GCS ≤8 points. The median of days of hospitalization was 14 (1–34 days).
3.8. Outcome
There were eight deaths with a mortality rate of 19.5%; all of them required Mechanical Ventilation (MV); three of the subjects were in stage II and five in stage III. Three patients died of septic shock and five because of ventilator-associated pneumonia. According to the type of diagnosis two (25%) had a definitive diagnosis, five (62.5%) a probable diagnosis, and one (12.5%) with a possible diagnosis. The median of days to death since hospitalization was 12.5 days (3–35 days); univariate analysis showed a statistically significant relationship between an adverse outcome and clinical stage III (p = 0.034). There was no statistical relationship between death and not having a definitive diagnosis (p = 0.109) (Table 5).
| Variables | Discharge (n = 33) | Death (n = 8) | p-value |
|---|---|---|---|
| Demographic characteristics | |||
| Sex, n (%) | 0.22 | ||
| Male | 14 (42.4) | 1 (12.5) | |
| Female | 19 (57.7) | 7 (87.5) | |
| Age (years), median (range) | 28 (18–57) | 28.5 (18–53) | 0.869 |
| Risk factors, n (%) | |||
| HIV infected | 12 (36.4) | 1 (12.5) | 0.398 |
| Use of illicit drugs | 18 (54.5) | 3 (37.5) | 0.454 |
| Severity of disease, n (%) | |||
| BMRC I | 7 (21.2) | 0 | 0.31 |
| BMRC II | 19 (57.6) | 3 (37.5) | 0.436 |
| BMRC III | 7 (21.2) | 5 (62.5) | 0.034 |
| Suggestive Thwaites score, n (%) | 32 (97) | 8 (100) | 1 |
| Type of diagnosis, n (%) | 0.109 | ||
| Definitive | 21 (63.6) | 2 (25) | |
| Nondefinitive | 12 (36.4) | 6 (75) | |
BMRC, British Medical Research Council.
Mortality according to risk factors, severity of disease and type of diagnosis
4. DISCUSSION
Large-scale studies describing the adult population with TBM continues to be a major topic in public health because of its high prevalence worldwide. These series of patients were diagnosed and treated in a second-tier hospital, but the morbidity and mortality were still high. The clinical course of this disease has already been described in large-scale studies worldwide; most of our findings were similar when compared to those studies [12–15]. Among the risk factors we studied, 51.2% of our patients were illicit drug users, inhaled methamphetamine being the most frequent illicit drug used in 43.9% of the patients and only two (4.8%) were Intravenous (IV) drug users, contrary to other authors describing TB to be more frequent in IV drug users [16]. It is notable that illicit drug use was more frequent in patients with a nondefinitive diagnosis (30.4% vs. 77.8; p = 0.004). We also detected that 61% of our patients had active pulmonary TB, compared with the 30–50% described in the literature [4]. In 2002, Thwaites et al. [10] described criteria to differentiate between TBM and non-TBM; according to those criteria, 97.6% of our patients were categorized as having TBM and a definitive diagnosis was made in 23 (56.1%) patients, without statistical difference between both groups (p = 0.439).
We reported a 19.5% mortality rate, this rate is comparable to the 23% reported by Thao et al. [9] in 2018 from a database of 951 non-HIV and 748 HIV-infected patients from where a 9-month mortality prognostic model was developed; the reported risk factors for non-HIV patients were age, history of previously treated TB, presence of focal neurological signs, and not receiving treatment with dexamethasone; as for HIV-infected patients, risk factors included an abnormal plasmatic sodium level, lower weight, and lower CD4 cell count; also, a higher BMRC severity grade at admission and a lower CSF lymphocyte cell counts were common predictors of death. A noteworthy fact is that 80% of our patients that required MV died; Misra et al. [17] compared mortality between 38 TBM patients that required MV with 36 non-MV TBM patients; of which 71% of the MV patients died and none of the non-MV patients, concluding that MV is not directly related to death in patients with TBM.
As expected, mortality had a significant relationship with later clinical stages. This highlights the importance of performing a timely diagnosis. TBM suspicion should be higher in subjects with more than 15 days of persistent headache, fever, weight loss, and altered level of consciousness. Also, there was no statistical difference between mortality, demographic characteristics, risk factors, and diagnostic subtype. In this series, the new molecular techniques for detection of Mtb in the CSF, such as real-time PCR and Xpert MTB/RIF (Cepheid, Sunnyvale, CA, USA), showed the highest rate of diagnosis with excellent timing. Xpert MTB/RIF is an automated rapid nucleic acid amplification technique that stands out as the initial diagnostic test recommended by the World Health Organization when clinical suspicion of TBM is high; this method that takes <2 h to detect Mtb and rifampicin resistance has a pooled sensitivity of 79.5% (62–90%) when compared against CSF culture [18,19], we used this technique in 10 of our patients, being positive in 90% of them. In 2017, Bahr et al. [20] compared the new generation of this assay called Xpert MTB/RIF Ultra (Cepheid, Sunnyvale, CA, USA) to the previous generation, and reported a composite sensitivity of 95% (95% Confidence Interval (CI): 77–99; 21 of 22 cases) for the Ultra Xpert MTB/RIF, better than the 79.5% previously reported for the Xpert MTB/RIF both with a specificity of 95%. Limitations of our study include its retrospective nature where data obtained from the medical records may be biased due to interobserver variability of clinical signs and the diagnostic approach of each case.
5. CONCLUSION
In this descriptive study, we report the clinical features and in-hospital outcome of an adult Mexican population with TBM. We found that most of the baseline characteristics of our population were similar to the ones described over the past decade by other authors worldwide. No statistically significant difference was found among patients with a definitive diagnosis and those with a positive Thwaites score; therefore, in our series, the latter proved to be a useful and easy to reproduce diagnostic tool to aid in the diagnosis of TBM. The new molecular testing methods yield the highest diagnosis rate, and they should be used whenever there is a high clinical suspicion for TBM, especially in patients who present with subacute onset of headache, fever, and altered mental status. The use of these tests will shorten the time in establishing a diagnosis and initiating treatment. This strategy will probably impact morbidity, mortality, and will help reduce treatment resistance in the future.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest. There is no affiliation with any organization with a direct or indirect financial interest in the subject matter discussed in the paper.
AUTHORS’ CONTRIBUTION
MGG and FAGM conceptualized the study. MGG and SNA collected and analysed the data. AGD contributed to experimental design. FAGM, SNA and AGD drafted and revised the manuscript for intellectual content.
ACKNOWLEDGMENTS
The authors would like to thank Dr. Rene Veytia-Flores for proofreading the manuscript, and also to the Department of Internal Medicine of Tijuana General Hospital for their collaboration.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Miguel García-Grimshaw AU - Francisco Alejandro Gutiérrez-Manjarrez AU - Samuel Navarro-Álvarez AU - Alejandra González-Duarte PY - 2019 DA - 2019/11/06 TI - Clinical, Imaging, and Laboratory Characteristics of Adult Mexican Patients with Tuberculous Meningitis: A Retrospective Cohort Study JO - Journal of Epidemiology and Global Health SP - 59 EP - 64 VL - 10 IS - 1 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.191023.001 DO - 10.2991/jegh.k.191023.001 ID - García-Grimshaw2019 ER -