
Dengue Outbreak Response and Control in Khyber Pakhtunkhwa, Pakistan: A Mixed Methods Study
- DOI
- 10.2991/jegh.k.191125.001How to use a DOI?
- Keywords
- Dengue fever; dengue control strategies; dengue mortality and morbidity in KP; Pakistan; mixed method study; dengue outbreaks in KP
- Abstract
Background: Since 2008, dengue fever outbreaks had occurred repeatedly in various districts of Khyber Pakhtunkhwa (KP) province of Pakistan. Most importantly the outbreak of 2017 caused 70 deaths, about 121,083 suspected and 24,938 confirmed cases in 23 districts of KP. In 2018, an abrupt decline in suspected and confirmed dengue cases was observed and 2018 was declared as dengue outbreak free. This study characterizes and explores the control and response measure activities of the outbreak. In addition, we explored the challenges faced and lessons learned for control of future dengue outbreaks from the perspectives of health authorities and dengue response staff in the KP province of Pakistan.
Methods: This was a mixed methods study with quantitative data on dengue outbreaks obtained from health department in KP followed by qualitative study to explore activities and responses that enabled the Dengue Response Unit (DRU) for a successful dengue outbreak control in 2018. In-depth interviews were conducted with the key informants from the department of health and the dengue response unit.
Results: The quantitative data analysis revealed a huge decline of suspected and confirmed dengue cases in comparison with the previous year in most of the KP districts. A similar decline in dengue reported cases was also observed from previously high dengue burden 14 union counsels of Peshawar district. Among the 70 verified deaths in 2017, 44 (63%) were males and 26 (37%) were females. The cases were about 20% each from age groups of 21–30, 41–50, and 51–60 years. The qualitative study findings showed four prominent major themes for successful control: (1) control and response strategy; (2) organizing specific dengue control and response intervention activities; (3) addressing dengue control and response challenges; and (4) generating lesson for future dengue control and response.
- Copyright
- © 2019 Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Dengue fever also known as break bone fever is a serious and sometimes fatal infection. It transmits through mosquito bite (most commonly by Aedes aegypti and Aedes albopictus types of mosquitoes), and it affects all ages of the population. The disease may be characterized from mild symptoms to life-threating condition. The symptoms may range from moderate headache, nausea, vomiting, muscular pain, and high-grade fever to severe abdominal pain, persistent vomiting, bleeding gums, low pulse, and narrow pulse pressure. Neurological symptoms may include confusion, unconsciousness, and shock [1,2]. Early detection and timely initiation of appropriate treatment can reduce mortality to <1% compared with 2–5% if left untreated [3].
Recently, dengue pandemic has been noted in various parts of the world. It is estimated that about 2.5 billion people are at risk of contracting the disease every year [4]. Asia alone contributes to 70% of the global burden of dengue [3]. In the Americas, about 2.38 million dengue cases caused a death toll of 1032 in 2016 with most cases from Brazil [5]. Smaller outbreaks were reported in the Northern America (Florida) in 2009 and 2010 as well as in Europe (France) in 2013–18 [6,7]. Dengue fever outbreaks routinely and progressively happen each year in South and Pacific Asian countries including India, Bangladesh, Sri Lanka, Indonesia, and Malaysia [8]. India and Myanmar have also been severely affected by dengue outbreaks in recent years with 21,000 cases in 2015 and 89,832 cases in 2011–2015, respectively [9,10].
In Pakistan, dengue hemorrhagic fever was recognized as a major public health problem in 2006 when the first major outbreak caused 4800 positive cases and 50 death toll. This was followed by 2008 outbreak that hit the entire country [11]. A massive outbreak in 2011 in Punjab province affected more than 21,597 individuals and claimed 365 precious lives [12]. Since then, every year thousands of positive cases and hundreds of deaths have been reported [13,14].
In Khyber Pakhtunkhwa (KP) province of Pakistan, the disease has been there since 2006 with low magnitude [12]; however, in 2013 an estimated 9024 positive dengue cases with 70 deaths were reported in Swat [15]. This was followed by another outbreak in 2014 claiming the lives of many men, women, and children. In 2016, 272 dengue cases were reported by a health facility in Batkhela, a locality of Swat district [16].
The dengue outbreaks remained confined to specific geographical areas (districts) in 2013–16 [17,18]. In 2017, the outbreak spread to the entire province. Out of 95,000 suspects, 20,000 emerged as confirmed cases and claimed 61 lives. Most of these cases were reported from Peshawar district, the provincial capital [19,20].
The aim of this study was to document the burden of dengue in KP province of Pakistan and to assess the dengue outbreak control and response measures undertaken by the provincial health authorities in 2017–18. The study also looked at the gaps, challenges, and lessons learned from previous dengue outbreaks.
2. METHODOLOGY
A sequential explanatory mixed methods design of Quant–Qual was used. For the quantitative part, descriptive cross-sectional data previously acquired was used. Verbal consents were obtained from the participants.
2.1. Quantitative Part
2.1.1. Methods of data collection
Case definition: Any person having acute onset fever of (>38°C) for 2–10 days with at least one of the following manifestations: severe headache, retro-orbital pain, myalgia, and arthralgia was considered as a dengue suspect, and referred for laboratory testing.
Study settings: This study was carried out in KP province of Pakistan.
Sampling technique: Quantitative data was obtained from the provincial Health Department, KP, Pakistan.
Inclusion criteria: All the districts of KP that had dengue outbreaks in 2017 were included in the study. Excel-based spreadsheets of data were obtained from provincial Department of Health. Eleven districts of KP that were highly affected by dengue were selected for the study. Similarly, 14 Union Councils (UCs; administrative subdivisions of a district) with high dengue prevalence of Peshawar district were also included.
Exclusion criteria: The districts with insignificant number (n ≤ 6) of dengue cases were excluded.
Analysis plan: The data were analyzed using Microsoft Excel 2013. The data were compared for distribution and differences of dengue cases in different districts and in UCs of the most severely hit districts of the province (Peshawar). Mortality statistics were calculated by age group and gender. Monthly trend analysis was done for seasonal peaks of the outbreak.
2.2. Qualitative Part
After completing the analysis of the quantitative data, in-depth interviews were conducted to probe the contributing factors that led to significant control of dengue outbreak in the year that followed the first outbreak (2017).
2.2.1. Data collection method
Study setting: An interview guide was developed and pilot tested. Six key informant interviews were conducted with Dengue Response Unit (DRU) at provincial Health Department using purposive sampling technique. All the information about the study participants were kept in lock and key and only the primary investigator had the access rights.
Analysis plan: The qualitative data was analyzed using ATLAS.Ti 0.8 version software (Scientific Software Development GmbH, Germany).
Data coding: A unique identification code number was assigned to each study participant. The responses to various interview questions were audiotaped and transcribed together with add on reflexive notes of the investigator for better understanding of the data content and reducing the subjectivity. The transcribed data were then shared with the participants for agreements or disagreements (if there were any). Deductive content analysis method was used. Codes, categories, subthemes, and themes were generated from the responses and experiences expressed by study participants about dengue epidemic control, response activities, challenges faced, and lessons learned. Similar ideas and concepts were identified and organized through codes in ATLAS.Ti 0.8 version. Comparable codes were assembled into subcategories and categories. Similar categories were merged to form themes. Thematic analysis was done through ATLAS.Ti 0.8 version software (Figure 1).
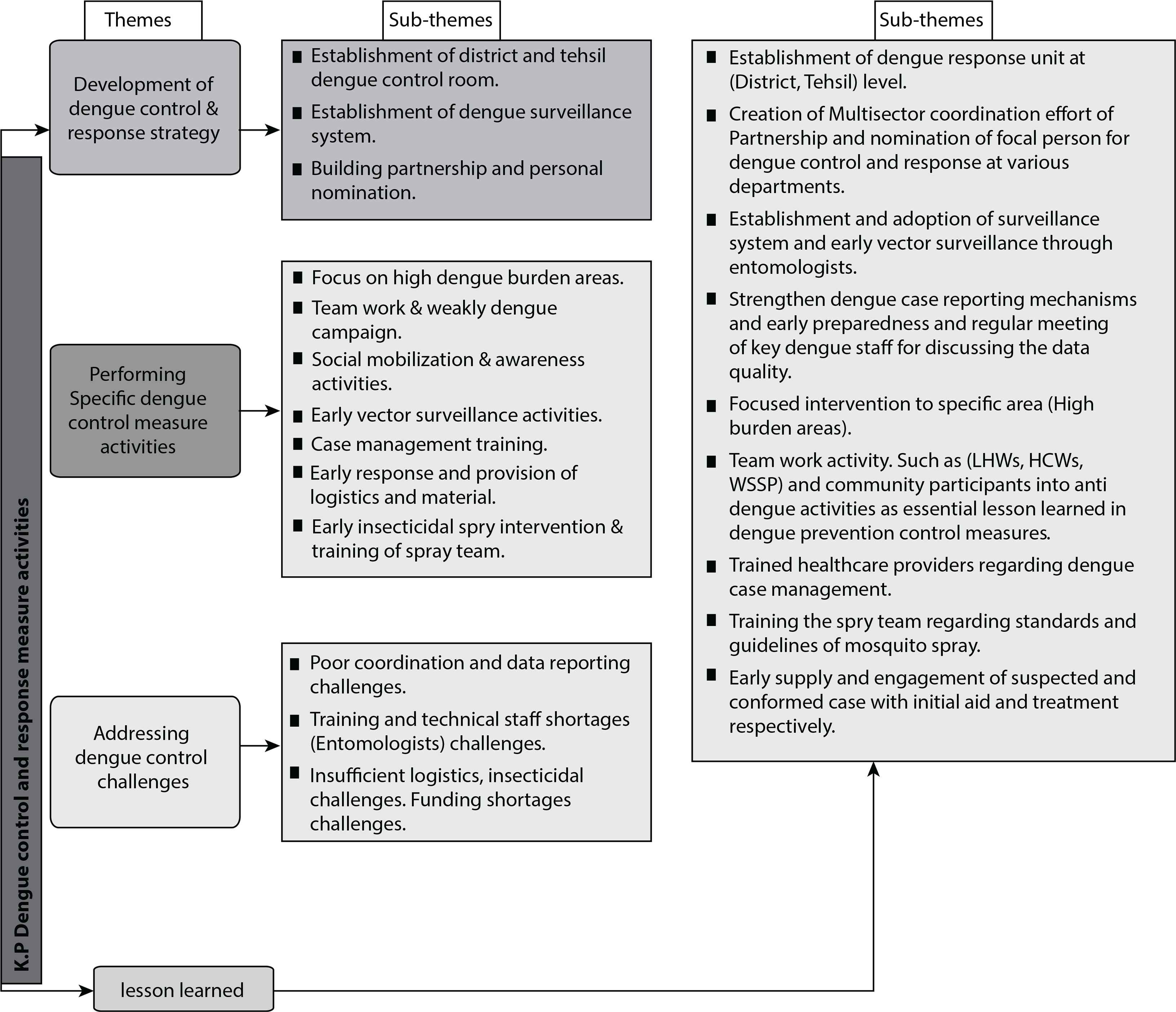
Illustrates the themes and sub-themes generated from the interview questionnaire.
3. Results
3.1. Quantitative study results
Eleven districts of KP province experienced massive dengue fever outbreak in 2017. Out of 121,083 total suspected cases, 118,188 (97.6%) were tested for dengue virus. A total of 24,938 (21.1%) tested positive for dengue. Majority (95%) of the cases (23,541) were from 91 UCs of Peshawar district. A small proportion was contributed by Mardan, Malakand, and Nowshera districts of KP (2017).
In contrast to 2017 dengue prevalence statistics, a significant reduction in dengue reported cases was observed in all districts of KP (except Haripur and Lower Dir where a slight increase in dengue cases was reported) in 2018 (Figure 2).
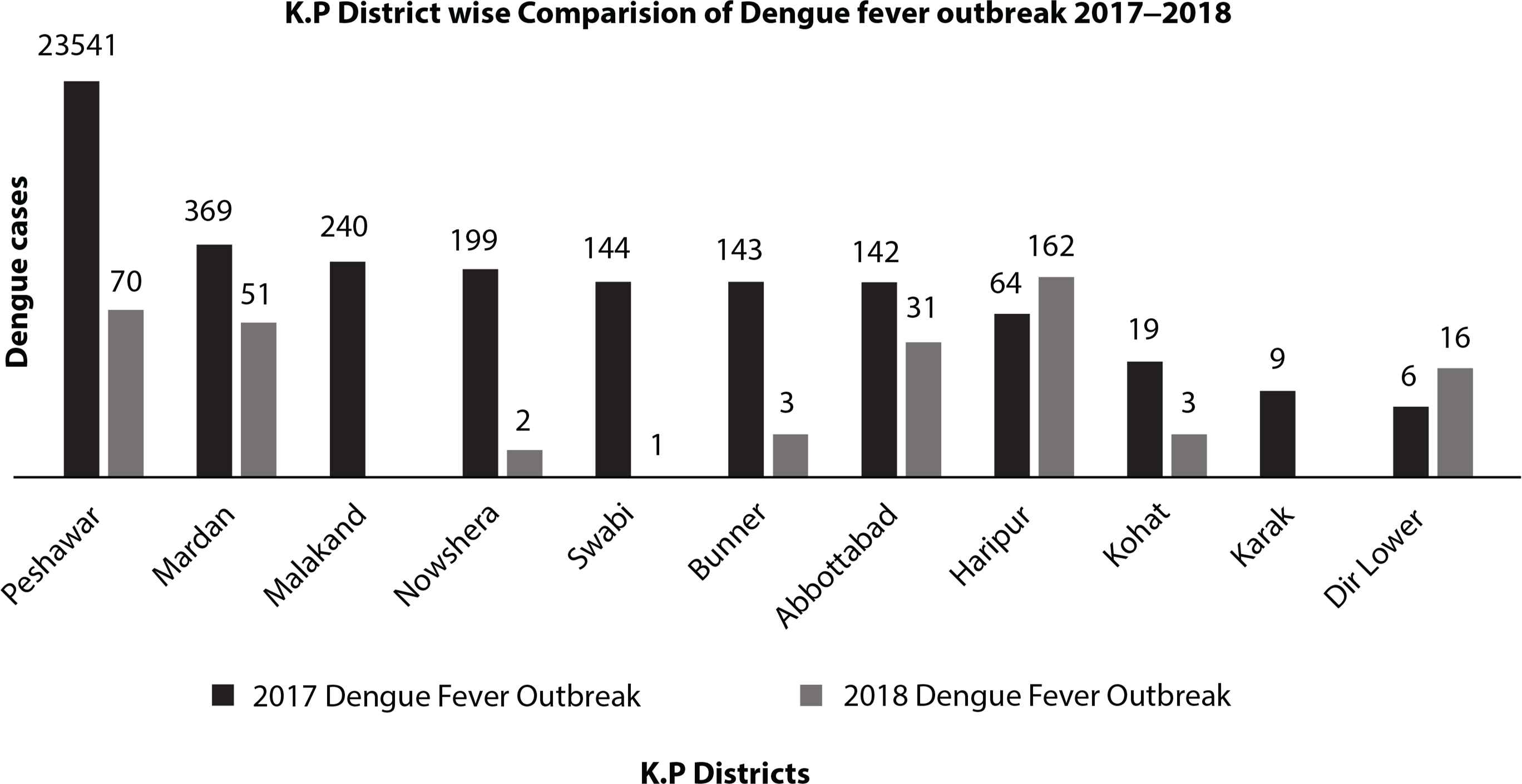
District wise distribution of dengue confirmed cases in K.P Province by 2017–2018.
In our study, a significant reduction in dengue outbreak was observed in the 14 UCs of Peshawar district with previous high dengue prevalence. As compared with 6033 dengue cases in 2017, only 13 cases were reported from those 14 high burden UCs in 2018 (Figure 3). In 2017, a total of 70 deaths occurred in Peshawar attributable to dengue, among them 63% (44) were males and 37% (26) females with majority in the age group of 21–30 and 41–60 (Figure 4), whereas no deaths were reported in the succeeding year (2018).
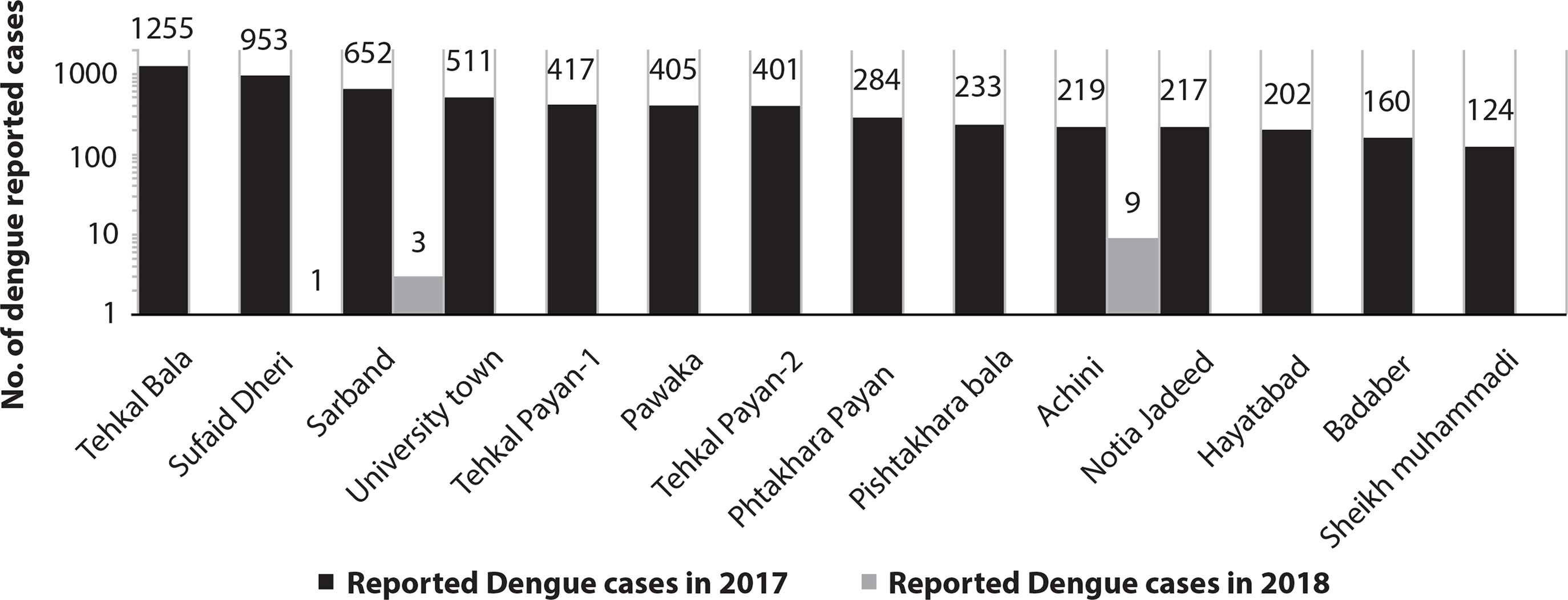
Comparison of Dengue outbreak in Peshawar UCs by 2017–2018.
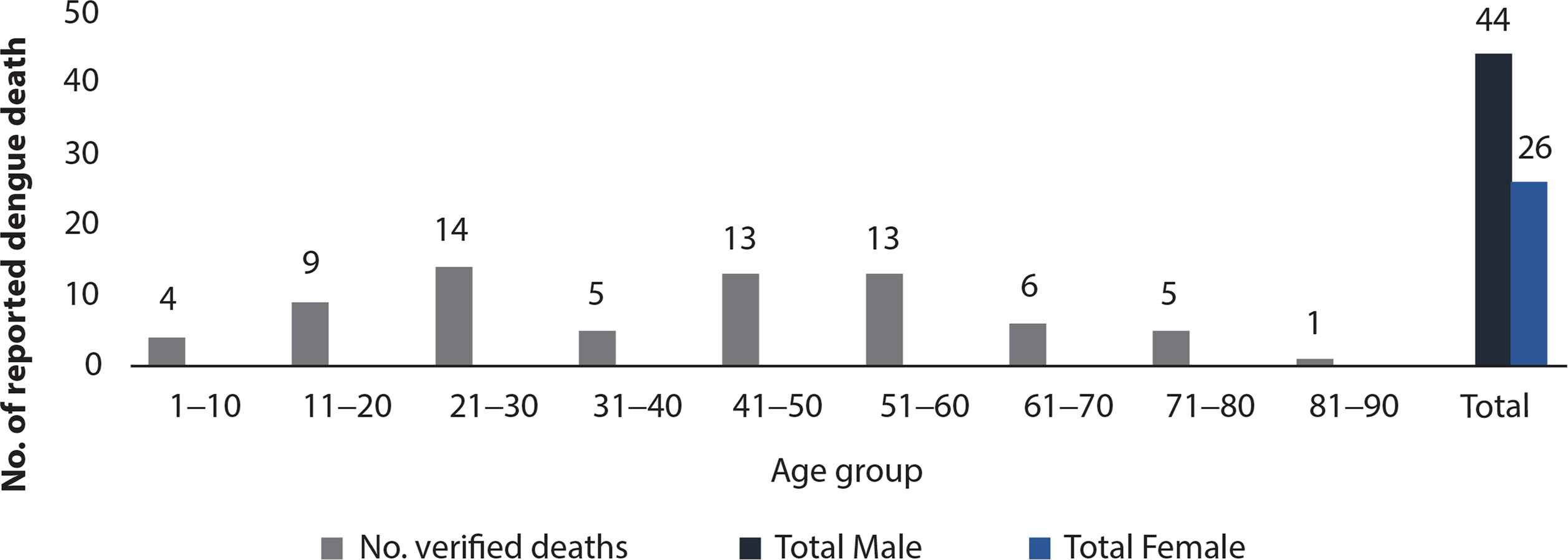
Dengue Mortality in K.P District in 2017.
The fever was found to be more in males than females. Out of the total 7951 patients, 4927 (62%) were males and 3024 (38%) were females. Furthermore, dengue was highly prevalent among the age group 21–30, 11–20, and 31–40 contributing 27%, 25%, and 17%, respectively, to dengue burden in Peshawar.
Data revealed that August, September, and October were the peak seasons for dengue outbreak in 2017. Month wise distribution of dengue outbreak in KP districts is shown in Figure 5.
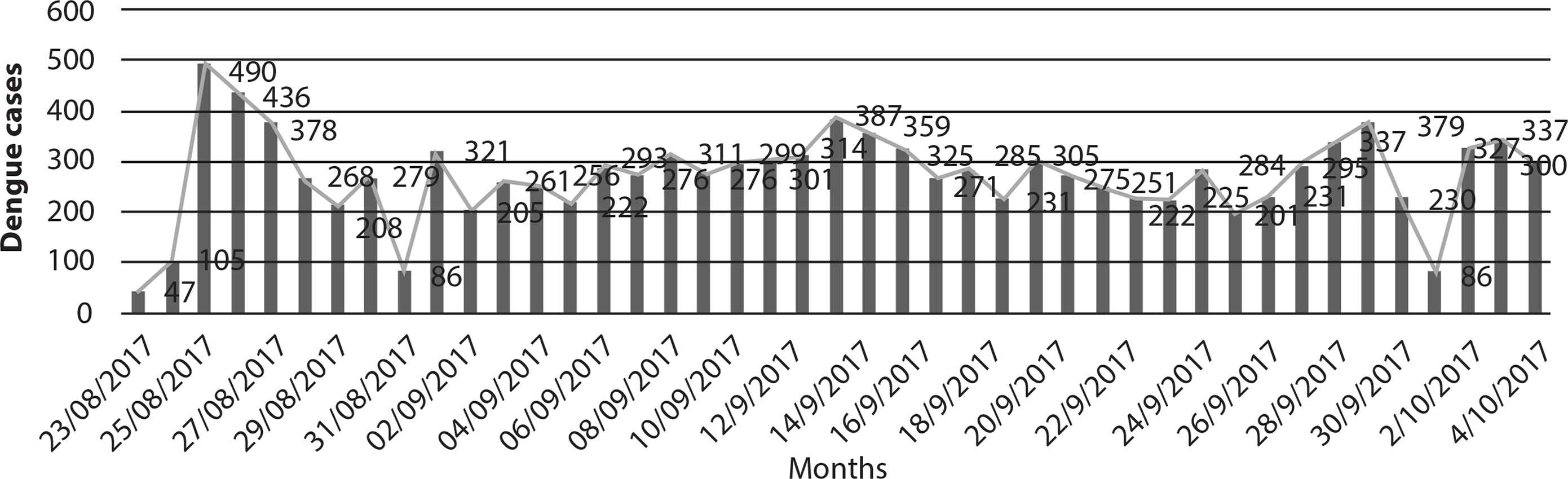
Monthly dengue outbreak trends in Peshawar.
3.2. Qualitative study result
Results are comprised of dengue control response strategies, activities, problem faced, and lesson learned with verbatim quotations used to illustrate key points. Each transcription was reviewed line by line. Free nodes were made for each sentence and then similar ones were combined to make subcategories. Comparable subcategories were merged to form categories and then subthemes and themes. The following main themes emerged:
Dengue control and response strategy: All participants highlighted the importance of and need for an evidence-based control strategy for successful control of dengue epidemics. The Health Department adopted a control strategy consisting of (a) Establishment of a DRU, (b) a functional dengue surveillance system, and (c) coalition and partnership with other sectors.
(a) Establishment of DRU
A dedicated office to control dengue epidemics did not exist until August 2017 despite having small-scale dengue outbreaks in the province for past 5 years. According to participants, a DRU was set up on priority basis for uninterrupted implementation of dengue control plans. As one of the participants mentioned,
“The first thing we did was the creation of DRU and adoption of IDSRS, which was not adopted well previously. Now we do a lot of activities for example: we are conducting effective surveillance activities to identify dengue cases and events.”
(b) Establishment of dengue surveillance system
Most of the study participants specified the importance of establishing a surveillance system even before the initiation of any intervention or dengue control activities.
The KP Health Department initially planned the establishment of Integrated Diseases Surveillance & Response System (IDSRS) with four basic surveillance systems. The dengue surveillance system also included vector management, vector surveillance and epidemiological surveillance, case management, and social mobilization.
“We devised a response plan that how we can control this outbreak to a smallest geographical region and to limit it spread to the other part of the province and other parts of Peshawar. Our initial plan was developing and adopting IDSRS.”
(c) Building anti-dengue drive collaboration effort
All participants repeated similar reflection on the importance of anti-dengue joint efforts. They had the view that without multisectoral approach, it was nearly impossible to tackle the menace of dengue. Initially, 19 line departments were formed as part of anti-dengue drive.
A focal person from each selected department was nominated and distinct roles were assigned to contribute dengue control efforts.
“We formed nineteen-line departments (19-Anti-dengue institutions). You know dengue cannot be done alone by single entity (department).”
Specific dengue control and response intervention activities
The DRU introduced specific control and response measures that worked well in preventing the likelihood and probability of dengue outbreak events in the subsequent year (2018). Fourteen high-risk UCs in Peshawar were selected for special consideration after a thorough dengue epidemiological survey in the city. The area was divided into green, yellow, and red zones. Yellow areas have some possible potential pockets for larval breeding, whereas red zone was identified by entomologist as the dense areas for larval breeding. Dedicated teams eliminated 70–80% of the potential larval breeding sites mechanically as well as chemically.
“We deploy teams to eliminate the sources potential breeding sites, and mechanically remove the larvae. Through this process we eliminated 70% to 80% of the larvae from active breeding sites.”
Training of the dengue response team and weekly dengue campaigns: According to participants, the workforce was trained on surveying the areas for detecting and eliminating potential larval breeding sites along with house-to-house awareness campaigns. Overall in KP >300 dengue control and response teams were formed, trained, and deployed to conduct weekly anti-dengue campaigns. Each team was assigned their designated roles. Women and community health workers were dedicated for house-to-house awareness and education about dengue prevention. Similarly, entomologists for active dengue surveillance, water and sanitation staff for collecting stagnant water sources as well as improvement of waste disposal were established. Technical assistance and protocols were adopted from volunteers and non-governmental organizations. The potential impact of these activities in reducing larval index has been emphasized by majority of the study participants.
Dengue case management training activities: Dengue case management training sessions for healthcare providers were conducted. The participants endorsed the impact of early diagnosis and initiation of recommended therapy in limiting the dengue mortality rate. As per a participant:
“We trained medical officers and clinicians in dengue case management as per international standards.”
Social mobilization and awareness activities: According to the participants, communities were educated on preventive measures and where to seek care in case of infection. Mass media campaigns against dengue were carried out through various channels, such as TV ad programs, text messages for dengue prevention, and awareness campaigns using pamphlets and posts. Local communities were mobilized through Madrassas (religious institutes) and mosques.
Early vector surveillance activities: An early active surveillance for vector management was placed in the region along with early detection of potential mosquito nests. In addition, a prompt reporting and analysis mechanism for dengue suspected and confirmed cases was also established. These activities enabled dengue control unit (DRU) to take early targeted interventions that helped in minimizing the intensity of the outbreak.
Rapid response and provision of logistics and materials: The DRU provided first aid and bed nets to the affected families. Healthcare providers were sensitized and intimated about timely availability of plasma in case of hemorrhagic fever. The dengue control management have also provided blood plasma and blood bags to the hospitals.
Early insecticidal spray intervention: In the past years and particularly during the major dengue outbreaks in the province, the insecticidal spray activities (vehicle-mounted spray) were conducted in most parts of the province. However, it did not help in minimizing the magnitude of dengue epidemic in the affected areas. Late detection of mosquito breeding sites and late insecticidal spray (fogging) activities with untrained fogging teams were considered to be the reasons for curtailed effects by the study participants. However, according to the respondents, these challenges were overcome in 2018 as insecticidal sprays and fogging activities were carried out according to dengue epidemic surveillance report.
3.3. Addressing dengue control challenges
While implementing dengue control strategy program, the DRU faced multiple challenges.
Coordination and data reporting challenges: All participants highlighted that lack of coordination among different departments and absence of uniform data reporting system were the biggest challenges faced during early developmental stage (2017) of DRU. Furthermore, physicians were not trained and informed about a dengue case definition, management, and referral and reporting system. In the early phase of the disease in 2017, a real-time reporting system was not in place. All departments were working in silos without a strong centralized system.
Technical staff shortages: Lack of technical experts, especially, entomologists in Provincial Health Department also hindered dengue-preventive activities in early developmental phase of the outbreak in 2017. As entomologists are the primary staff responsible for conducting dengue epidemiological surveillance along with mechanical removal of the larvae. The department did not anticipate the outbreak, therefore no entomologist was hired at that time.
In the early phase of 2017 dengue outbreak, the World Health Organization (WHO) provided expert entomologists upon request from the Health Department. However, as early larval sites were not detected as required, the outbreak spread to a wide geographical area affecting thousands of people. After that a special cadre was created in the Health Department and entomologists were hired. They were trained by WHO staff. As a result, in 2018, early detection of larval sites was done and larvae were removed before the start of dengue season.
Insufficient logistics and timely availability of insecticides: According to the participants, the Health Department was not prepared for 2017 outbreak. There was no early warning of the outbreak and at the time department had insufficient supplies of insecticidal sprays and bed nets. Importing anti-dengue supplies took time due to government hierarchical system that further delayed the dengue control activities in the province in 2017. These challenges had been overcome by 2018.
Funding shortages: Financial constraints remain to be one of the biggest challenges mentioned by most of the participants. In early phase of the outbreak in 2017, no or little funds were dedicated for dengue control. There were no specific funds allocated for mass media campaigns. As entomologist cadre was not introduced at the time, there was no identified budget for it as well.
Owing to the lack of a dedicated unit for dengue control, most of the funds were distributed among different departments. Random dengue control activities were carried out in a chaotic manner due to lack of a centralized policy and guidance system. Duplication of fogging and insecticidal sprays were done in the same geographical areas by different departments without coordinating with each other and disregarding the recommended intervals. This unsystematic repetition of dengue activities had further squandered the limited funds.
3.4. Lessons learned from dengue outbreak control and response
The prominent difference in successful control of expected dengue outbreak of 2018 was the implementation of dengue control strategy that lacked in 2017. The early phase outbreak in 2017 was a major one in the province, hence the Health Department was not fully prepared and well equipped, which resulted in poor control of the disease. However, in 2018, the Health Department was alert and precautionary measures were taken ahead of the dengue peak seasons that helped in limiting the outbreak in KP province. The participants unanimously considered the following activities in successful dengue control in the province in 2018.
Establishment of DRU at district and tehsil level was the hallmark of dengue prevention strategy in the province. The uniformed flow of information and coordinated control measures from DRU such as case definition, management strategy, spray and fogging timing, and vector surveillance grossly helped in successful control. As an established fact, dengue outbreak cannot be successfully controlled by the Health Department alone; however, creation of effective multisectoral coordinated efforts between all relevant departments assisted in curbing the menace of dengue in 2018 compared with 2017, where such liaisons did not fully exist. Furthermore, establishment and adoption of a dengue surveillance system facilitated in early detection and control of larval sites as well as early vector surveillance through designated entomologist. Moreover, regular meetings of the key dengue control staff helped in understating the data pattern and maintaining the data quality along with focusing on high-burden areas for targeted intervention such as insecticidal sprays, fogging, and removal of larval reservoirs. Training of the spray teams were arranged according to international standards and guidelines. Community participation were ensured by engaging local political and religious leaders for awareness campaigns and precautionary measures.
4. DISCUSSION
According to our knowledge this is the first comprehensive mixed method study that explores both the burden of dengue fever outbreak and control and response measures undertaken to tackle the spread of the disease in the province. Considerable progress on dengue control and response had been made in KP province in 2018.
Our findings show decrease in the number of positive dengue cases from 24,876 in 2017 to 339 in 2018 in 11 previously high dengue epidemic districts of the KP province. Similarly, 14 previously high dengue burden UCs of Peshawar districts showed significant reduction from 6033 cases in 2017 to 13 cases in 2018.
The reduction in the number of dengue cases and outbreak frequencies in 2018 was the result of establishment of dengue surveillance system, dengue control cells, along with its basic elements (vector and epidemiological surveillance, vector control, case management, social awareness, and social mobilization), and strengthening of reporting mechanism and data evaluation system across the province.
Establishment of dengue surveillance system and mapping of mosquito dense areas have also been reported in literature as the significant reasons of dengue control [21–23].
Evidence suggests that underreporting, misjudged cases, late detection problem, late response, and late insecticidal spray are associated with the absence of or lack of active surveillance system. Poorly designed interventions and futile activities make the situation worse instead of curbing the outbreaks [24].
In addition to the establishment of surveillance system, our study participants revealed strong connection between reduction of mosquito larval index (70–80%) and focused intervention on high-burden areas, deployment of entomologist, initiation of early vector surveillances, early insecticidal spray, deployment of teams for weekly house-to-house anti-dengue campaign. These activities are also endorsed by WHO global strategies for dengue prevention.
Furthermore, a total of 19 departments (multisectoral coordination) participated in the coordinated effort against dengue outbreak. Nomination of focal person from each department who assisted in seamless implementation of dengue control activities by eliminating ambiguous information played a significant role in limiting the spread of dengue and preventing outbreak. Significant correlation between entomological parameters and dengue incidence were reported [25,26].
Importantly, community education and awareness campaign, and case management training activities were organized in various public and private organizations. The aim was to improve both the knowledge of communities and providers. Preventive messages about dengue fever were communicated through various TV and radio channels. These activities were fruitful in limiting the dengue outbreak in 2018 in contrast to 2017, where they were not fully adopted.
Similar findings regarding the importance of these activities were also revealed by other researchers [27–29]. Data suggest that significant decrease (13%) in dengue fatality rate was observed after improved dengue case management [30]. In this study, the participants also highlighted the contribution of proper dengue case management training in substantial decrease of dengue mortality rate in KP province. These activities are cost-effective and can be applied in any geographical areas with a little modification in awareness campaigns according to the cultural needs of that area.
5. CONCLUSION
Dengue Surveillance and Response System along with four basic elements (vector and epidemiologic surveillance, vector management, community mobilization, and case management) is highly successful intervention; however, surveillance program is effective if the program is designed and implemented in a manner that encourages the communities, partnered with various stakeholders, to address broader challenges. Weekly anti-dengue campaign activities and broadening of other current dengue control and response measure activities are also useful. Development and use of electronic reporting mechanism is essential for future dengue control in the province.
ANNEXURE IN-DEPTH INTERVIEW GUIDE
| In-depth Interview Guide |
|---|
| Name |
| Designation |
| Department |
| Working in the organization since |
| Time & Interview date |
Question: Dengue control strategies in KP
Probes: Activities, campaigns, funding, policies etc.
Question: Reasons of successful dengue control
Probes: Strategies, mechanism, coordination, predications
Question: Hindrances and difficulties faced during implementation
Probes: Activities didn’t work, funding issue, community cooperation etc.
Question: Lesson learned and expansion of these policies in other geographical areas
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
UQ, AL, SA and MA contributed in conceptualization. IUK and MAM contributed in data curation–quantitative data. MAM contributed in data curation–qualitative. MAM, AL and UQ contributed in formal analysis. MAM contributed in investigation. UQ, AL and MA contributed in methodology. MAM and AL contributed in project administration. UQ and AL contributed in supervision. SA contributed in validation. AL, UQ and MA contributed in visualization. MA, AL and UQ contributed in writing–original draft. UQ, AL and SA contributed in writing–review and editing.
FUNDING
This study is conducted as a student thesis for acquiring master degree in Public Health. No funds or grants were availed for conducting it.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Mohamed Ali Mohamud AU - Umair Qazi AU - Abdul Latif AU - Iftikhar Uddin Khan AU - Saeed Anwar PY - 2019 DA - 2019/12/31 TI - Dengue Outbreak Response and Control in Khyber Pakhtunkhwa, Pakistan: A Mixed Methods Study JO - Journal of Epidemiology and Global Health SP - 74 EP - 81 VL - 10 IS - 1 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.191125.001 DO - 10.2991/jegh.k.191125.001 ID - Mohamud2019 ER -