
Morbidity and Mortality Patterns in Children Admitted to Hospital in Thai Binh, Vietnam: A Five-year Descriptive Study with a Focus on Infectious Diseases
 , Van Thuan Hoang1, 2, 3, †, , Thi Loi Dao1, 2, 3, , Xuan Duong Tran1, Duc Long Phi1, Minh Manh To1, Van Nghiem Dang1, Van Khoi Dang1, Thanh Tung Dao4, Nam Thang Nguyen1, Thi Thuy Vu5, Duc Thanh Nguyen1, Duy Cuong Nguyen1, Nang Trong Hoang1, Thanh Liem Vu5, Thi Minh Chinh Nguyen5, Philippe Minodier3, 6, 7, Philippe Gautret2, 3, *,
, Van Thuan Hoang1, 2, 3, †, , Thi Loi Dao1, 2, 3, , Xuan Duong Tran1, Duc Long Phi1, Minh Manh To1, Van Nghiem Dang1, Van Khoi Dang1, Thanh Tung Dao4, Nam Thang Nguyen1, Thi Thuy Vu5, Duc Thanh Nguyen1, Duy Cuong Nguyen1, Nang Trong Hoang1, Thanh Liem Vu5, Thi Minh Chinh Nguyen5, Philippe Minodier3, 6, 7, Philippe Gautret2, 3, *, Equal work.
- DOI
- 10.2991/jegh.k.200723.001How to use a DOI?
- Keywords
- Children; infectious disease; lower respiratory tract infections; gastrointestinal infections; influenza; Thai Binh
- Abstract
The objective of this study was to describe the overall pattern of morbidity and mortality of children seen at the Thai Binh Paediatric Hospital in Vietnam, with a focus on infectious diseases. A retrospective review of hospitalisation records was conducted from 1 January 2015 to 31 December 2019. Data were obtained from a total of 113,999 records. The median age of patients was 18 months, with 84.0% of patients aged <5 years. Infectious diseases accounted for 61.0% of all cases. The most prevalent diseases were lower respiratory tract infections (32.8%), followed by gastrointestinal infections (13.3%) and confirmed influenza (5.4%). Most infections were not microbiologically documented. A total of 81.4% patients received at least one antibiotic. Most patients (97.0%) were hospitalised for less than 15 days. Regarding outcomes, 87.8% patients were discharged home with a favourable outcome. Twelve percent were transferred to the Vietnam National Children’s Hospital because their condition had worsened and 0.1% died. In total, infectious diseases accounted for 40.4% of deaths, followed by neonatal disorders (34.6%). Our data serves a basis for the identification of needs for diagnostic tools and for future evaluation of the effect of the targeted implementation of such facilities. Point-of-care tests, including real-time polymerase chain reaction assays to identify common pathogens should be implemented for more accurate diagnosis and more appropriate antibiotic use.
- Copyright
- © 2020 The Authors. Published by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Across most low-income countries, levels of both child and maternal mortality have dropped over the past three decades. The United Nations International Children’s Emergency Fund Millennium Development Goals succeeded in reducing child mortality by almost half around the world between 1990 and 2018 [1]. This has led to changes in the patterns of diseases which cause mortality in under-fives.
Preventable diseases such as Respiratory Tract Infections (RTIs), diarrhoeal diseases, malaria and Human Immunodeficiency Virus (HIV) infection are major causes of childhood morbidity and mortality world-wide [1]. The World Health Organization estimated that in 2018, 6.2 million children and adolescents under the age of 15 die annually, mostly from preventable causes. Of these deaths, over 5 million occurred in the child’s first 5 years, with almost half of these in the first month of life [1]. These diseases can be prevented, and treatments are accessible and affordable [1]. For children who are five and over, non-communicable diseases were the most common causes of death [2].
In Vietnam, the under-five mortality rate in 2010 was 19.4 per 1000 live births [3]. According to the Institute for Health Metrics and Evaluation, the major causes of child mortality in Vietnam in 2017 were maternal and neonatal disorders (31.3%), congenital birth defects (26.6%), Lower RTI (LRTI) (13.0%), whooping cough (3.0%), encephalitis (2.3%), meningitis (1.3%), diarrhoea (0.7%) and HIV (0.3%) [4]. Antibiotic resistance is now emerging as a risk factor for mortality and prolonged hospital stay among Vietnamese children [5,6].
The objective of this study was to describe the overall pattern of morbidity and mortality of patients below the age of 16 and seen at the Thai Binh Paediatric Hospital, a referral hospital in the central province of Thai Binh. In this paper, we focus on Infectious Diseases (ID). These data will help in designing standardised protocols for the proper management of the most common infectious diseases presenting at this hospital. They will also serve for identifying gaps in diagnostic and management tools and for evaluating the future implementation of targeted policies.
2. MATERIALS AND METHODS
2.1. Study Setting
Thai Binh (20°30′N, 106°20′E) is a coastal eastern province in the Red River Delta region of northern Vietnam. It is about 110 km from the capital city, Hanoi (Figure 1). In 2019, this province covers an area of 1542 km2 with 1,860,447 people [7,8], mostly living in rural areas (89.4%) with 15.5% of the population aged 0–9 years and 12.8% aged 10–19 years [8].
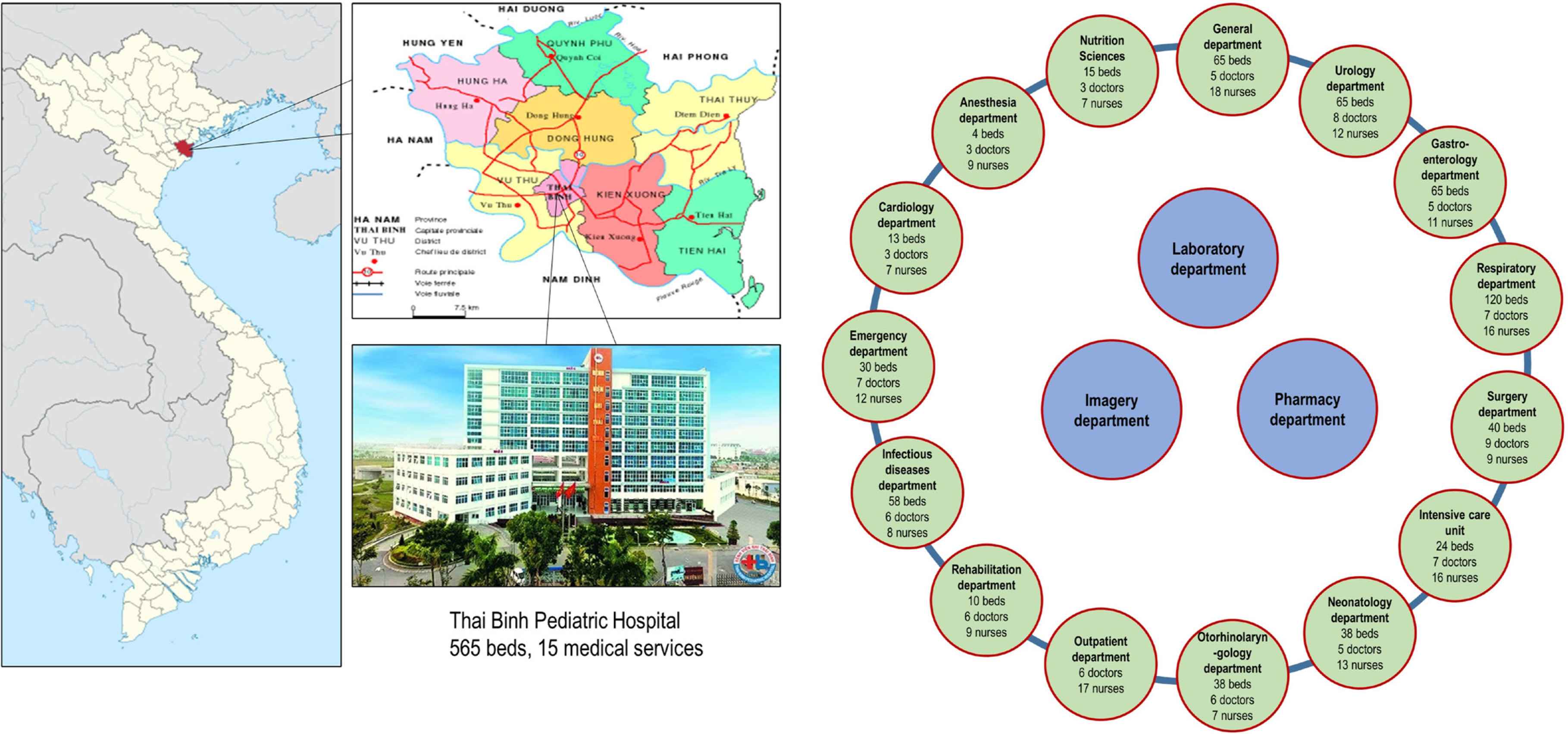
Study setting.
The Thai Binh Paediatric Hospital is a first-class hospital in the central province of Thai Binh (Figure 1). In 2019, this hospital had 565 beds spread across 15 different medical departments. In The number of beds in this hospital hardly meets the number of hospitalized patients. With the exception of the neonatal department, most other departments have an overload of patients compared to the number of existing beds. Eighty-six paediatricians and 171 nurses are currently working in the facility (Figure 1). Microbiological identification in the hospital laboratory uses common bacteriological cultures, serological assays and real-time Polymerase Chain Reaction (PCR) for a limited number of pathogens. Ill children under the age of 16 are directly admitted from home (through outpatient or emergency departments) or referred from eight district hospitals in the province of Thai Binh. Children with severe diseases who do not improve, are referred to the Vietnam National Children’s Hospital in Hanoi (VNCH). The medical records of patients have been digitally available only since June 2019, through a computerised system.
In Vietnam, all children under the age of 6 have free health insurance. Parents of children over the age of 6 then have to take out school-age health insurance. According to the expanded immunisation programme in Vietnam [9], tuberculosis vaccine is recommended as soon as possible within 30 days of birth. Three doses of pentavalent vaccine [diphtheria, tetanus, pertussis, hepatitis B and Haemophilus influenzae type B (Hib)] and oral polio vaccine are recommended between the ages of 2 and 4 months. The measles vaccine is recommended at 9–11 and 18 months. Three doses of Japanese encephalitis are recommended at 12 months, 2 weeks after the first dose and 1 year after the second dose. These vaccines are provided free of charge by the Vietnamese government. Vaccines against rotavirus and invasive pneumococcal diseases are optional, expensive and are not free of charge.
2.2. Study Design and Population
This is a retrospective review of consecutive morbidity and mortality occurring in children aged 0–16 years admitted to the Thai Binh Paediatric Hospital from 1 January 2015 to 31 December 2019.
Ethical approval was obtained from the Ethics Committee of Thai Binh Paediatric Hospital (No. 2019-12.1).
2.3. Data Collection Methods and Instruments
All medical records of eligible subjects were collected from central computer of the hospital and analysed by a team of 12 medical doctors. The eligibility criteria were hospitalisation at the Thai Binh Paediatric Hospital, documentation of the date and month of admission, age, gender, diagnosis, treatment and outcome (defined as discharged home, transferred to the VNCH, discharged against medical advice, or died).
Diagnoses at discharge were used for classification and categorised according to the International Classification of Diseases (ICD10 criteria) [10]. For concurrent diagnosis, children with more than one disease were grouped together depending on the doctor’s primary and secondary diagnoses.
Data obtained were analysed using STATA software version 14.2 (Copyright 1985-2015 StataCorp LLC, http://www.stata.com). Continuous variables were analysed and expressed as median and Interquartile (IQR). Categorical variables were presented as percentages.
3. RESULTS
3.1. Characteristics of the Study Population
Data were obtained from a total of 113,999 hospitalisation records over the 5-year study period. The median age of patients was 18 months (interquartile range 6–42 months, min = 0, max = 16 years) with 84.0% (95,737/113,999) of patients aged <5 years. In total, 60.5% (69,016/113,999) individuals were male with a sex ratio M/F of 1.5. The age-gender pyramid is shown in Figure 2. 75.7% (86,319/113,999) of patients lived in rural areas.
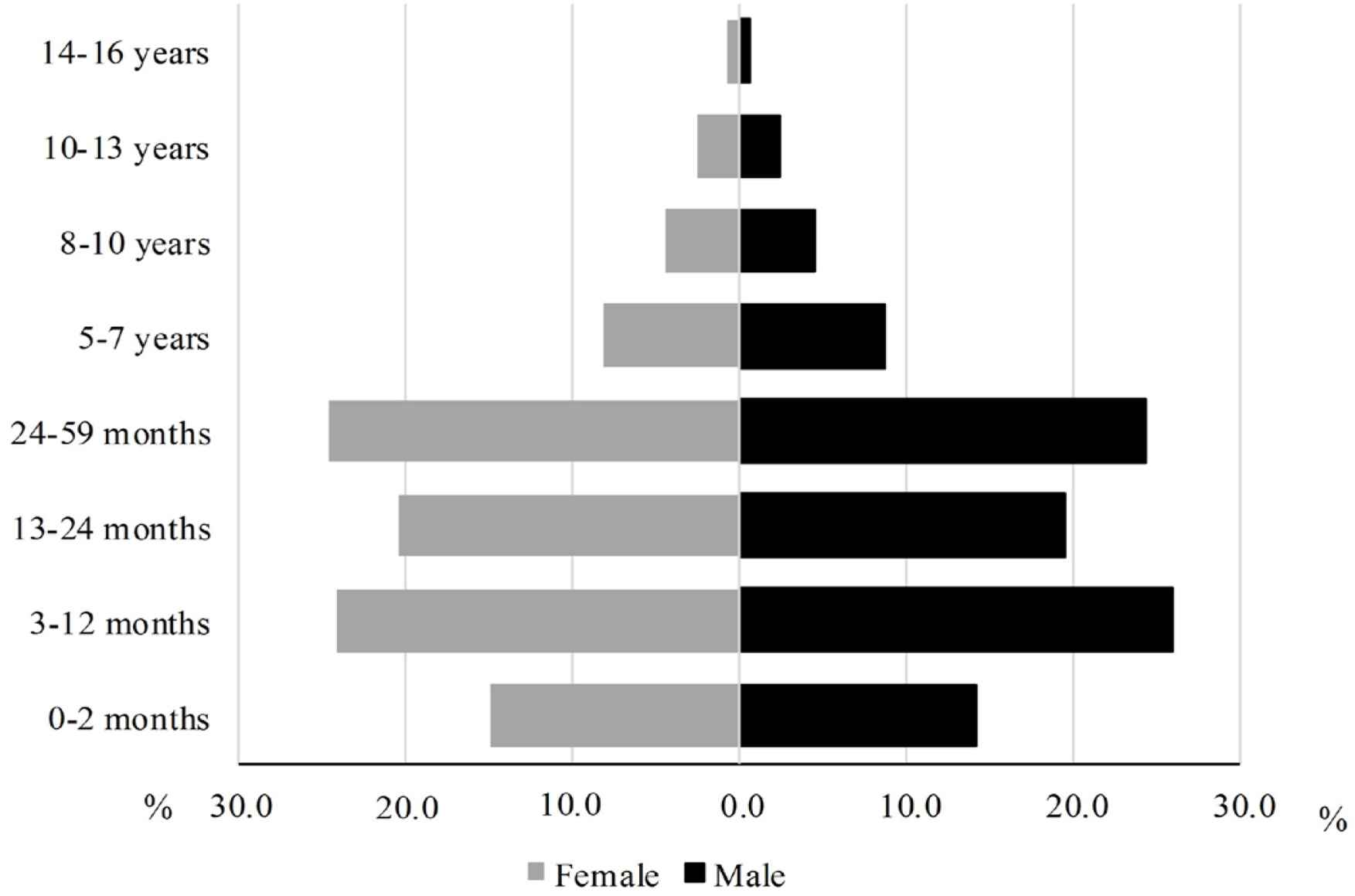
Age-gender pyramid of hospitalised patients.
3.2. Morbidity Patterns
Table 1 shows the distribution of diseases by syndromes during the 5-year study period. Overall, ID accounted for 61.0% of all cases. The most prevalent diseases were LRTI (32.8%), gastrointestinal infections (13.3%), and confirmed influenza (5.4%). Other IDs included fever of unknown origin (3.7%), skin infections (3.4%), hand, foot and mouth disease (1.8%), sepsis (1.3%), viral hepatitis (0.5%), meningitis/encephalitis (0.2%), HIV or tuberculosis (0.04%). Other infections represented 2.3% of the admissions. No cases of malaria were reported.
| Syndromes | n | Percentage (%) |
|---|---|---|
| Lower respiratory tract infections* | 37,439 | 32.84 |
| Gastrointestinal infections* | 15,175 | 13.31 |
| Influenza* | 6132 | 5.38 |
| Non-communicable gastrointestinal diseases | 5261 | 4.61 |
| Other non-communicable diseases | 4471 | 3.92 |
| Fever of unknown origin* | 4196 | 3.68 |
| Skin infection* | 3875 | 3.38 |
| Neonatal disorders | 3063 | 2.69 |
| Other infections* | 2631 | 2.31 |
| Unintentional injuries | 2089 | 1.83 |
| Hand, foot and mouth diseases* | 2011 | 1.76 |
| Haemoglobinopathies and haemolytic anaemia | 1618 | 1.42 |
| Sepsis* | 1444 | 1.27 |
| Congenital birth defects | 1414 | 1.24 |
| Convulsion and epilepsy | 1095 | 0.96 |
| Cardiovascular diseases | 969 | 0.85 |
| Neurological disorders | 852 | 0.75 |
| Diabetes and chronic kidney diseases | 785 | 0.69 |
| Headaches | 782 | 0.69 |
| Asthma and other chronic respiratory diseases | 658 | 0.58 |
| Mental disorders | 655 | 0.57 |
| Viral hepatitis*,¥ | 508 | 0.45 |
| Nutritional deficiencies | 418 | 0.37 |
| Food or drug poisoning | 318 | 0.28 |
| Meningitis and encephalitis* | 250 | 0.22 |
| Cirrhosis and other chronic liver diseases | 168 | 0.15 |
| Leukaemia | 114 | 0.10 |
| HIV and tuberculosis* | 45 | 0.04 |
| At least one infectious disease | 69,536 | 60.99 |
Infectious diseases.
Hepatitis B, C or cytomegalovirus.
Relative proportion of diseases (diagnosis at discharge) according to syndromic classification and etiologic diagnoses according to available laboratory tests, in 113,999 hospitalisation records of children hospitalised at the Thai Binh Pediatric Hospital between 2015 and 2019
Figure 3 shows the changes in morbidity patterns in hospitalised children in 2019 as compared to 2015. LRTI was consistently the most frequent cause of morbidity in hospitalised children. However, in 2019, influenza ranked as the second cause of hospitalisation, compared to ranking 25th in 2015. Gastrointestinal infections remained one of the most frequent causes of admission after respiratory infections over the study period.
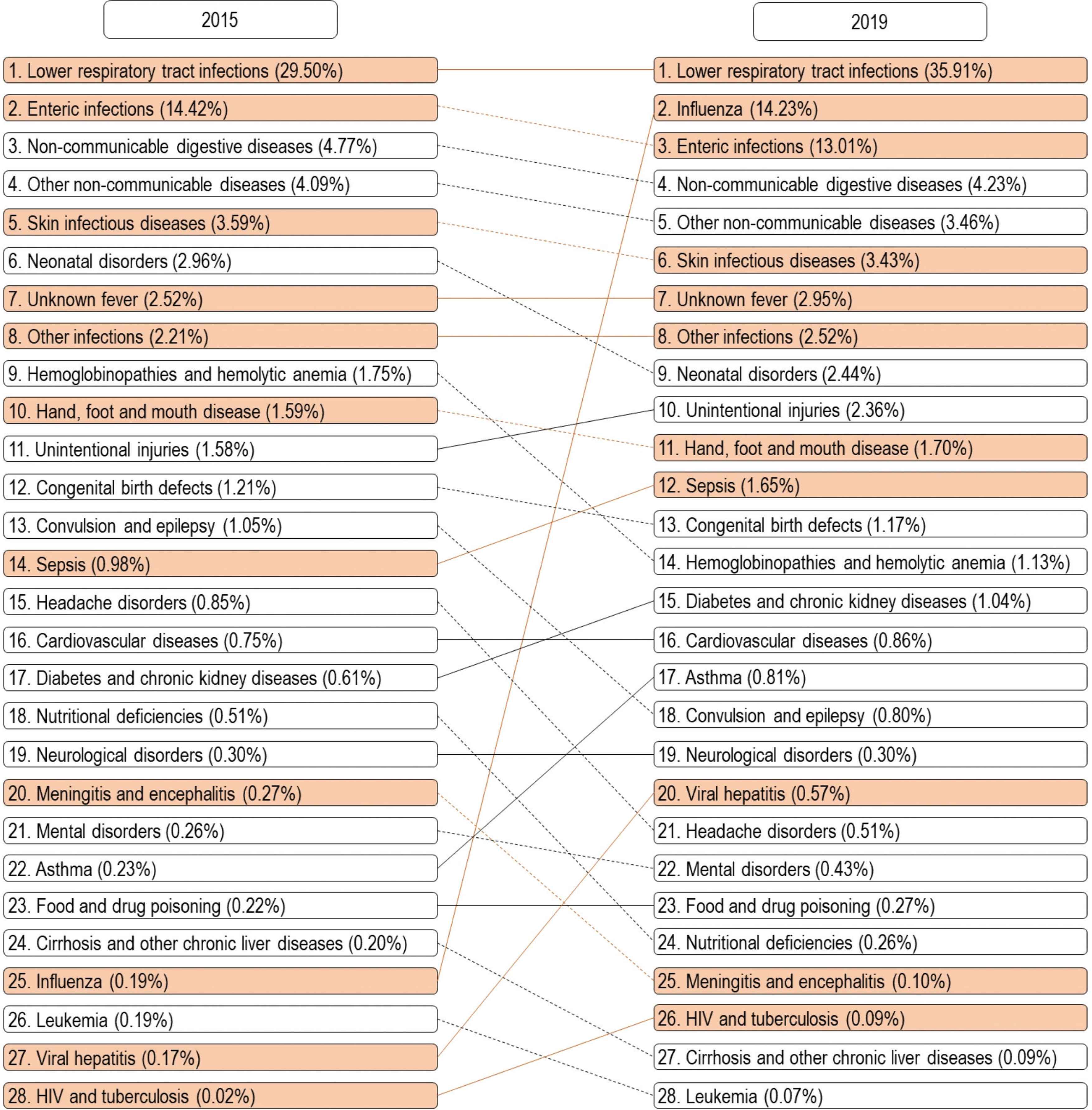
Morbidities (diagnosis at discharge) among hospitalised children at the Thai Binh Hospital in 2019 compared to 2015 (orange: infectious diseases, white: non-communicable diseases, solid line: stability or increase overtime, dashed line: decrease overtime).
A total of 81.4% (92,742/113,999) patients received at least one antibiotic, regardless of their diagnosis. Of them, 22.4% (20, 744/92, 742) were treated with an antibiotic combination. Among all patients, the most frequent antibiotic used was cephalosporin (65.6%), followed by penicillin (17.7%), aminoglycoside (11.3%), imidazole (3.8%), macrolide (2.0%), carbapenem (1.5%) and quinolone (1.0%). Other antibiotics were prescribed in 1.2% patients (data not shown).
Overall, the mean length of hospital stay was 6.0 ± 5.2 days (IQR = 3–7 days). Three percent of patients were hospitalised for more than 15 days.
3.3. Outcomes and Mortality Pattern
At total of 87.8% (100,043/113,999) patients were discharged home with a favourable outcome, 12% (13,680/113,999) were transferred to the VNCH because their condition had worsened, 0.1% (120/113,999) were discharged against medical advice and 0.1% (156/113,999) died. Deaths mainly occurred in children under the age of 5 (94.2% (147/156)) and in residents from rural areas (93.0% (145/156)). Table 2 shows the cause of death. ID accounted for 40.4% of cause of deaths and neonatal disorders accounted for 34.6%. LRTI and sepsis were responsible for 16.0% and 11.5% of deaths, respectively. Most patients who died resided in rural areas.
| Mortality | n | Percentage (%) |
|---|---|---|
| Under five years old | 147 | 94.2 |
| Male gender | 101 | 64.7 |
| Residence in rural area | 145 | 93.0 |
| Cause of death (diagnosis at discharge) | ||
| Neonatal disorders | 54 | 34.6 |
| Lower respiratory tract infections* | 25 | 16.0 |
| Cardiovascular diseases | 23 | 14.7 |
| Sepsis* | 18 | 11.5 |
| Fever of unknown origin* | 18 | 11.5 |
| Asthma and other chronic respiratory diseases | 7 | 4.5 |
| Congenital birth defects | 3 | 1.9 |
| Gastrointestinal infections* | 2 | 1.3 |
| Other non-communicable diseases | 2 | 1.3 |
| Cirrhosis and other chronic liver diseases | 1 | 0.64 |
| Leukaemia | 1 | 0.64 |
| Non-communicable gastrointestinal diseases | 1 | 0.64 |
| Unintentional injuries | 1 | 0.64 |
Infectious diseases.
Demographics and etiology among 156 children who died at the Thai Binh Paediatric Hospital between 2015 and 2019
4. DISCUSSION
This descriptive study was conducted at a provincial paediatric hospital which has limited diagnostic tools. Our main results are as follows: (i) 84% of hospitalised children were aged under the age of 5; (ii) 61% of them were diagnosed with an infection, with the four most prevalent conditions being LRTI, influenza, gastrointestinal infections and fever of unknown origin; (iii) 81% of children were prescribed antibiotics during their stay, whatever the diagnosis; (iv) the mortality rate was about 0.1% with ID as the leading cause of death.
The high percentage of infants and young children may be explained by the vulnerability of this age group. The anatomical characteristics and immunological immaturity of younger children put them at a higher risk of getting ill in general and of presenting severe forms of ID [11]. Several studies conducted in other countries also reported that the majority of hospitalisations in paediatrics were in children in this age group [11–15], with prevalence ranging from 73% to 90%. Children below the age of 5 also presented with a higher incidence of neonatal disorders and ID [11,12]. IDs are a leading cause of morbidity and mortality in young children [16]. An estimated 6.2 million children under the age of 15 died in 2018, mostly from preventable causes, and most of whom lived in middle- and low-income countries [1]. In Vietnam, an 8-year retrospective study (2007–2014) among 212,216 hospitalised children under the age of 17 in Hanoi [17] showed that ID was responsible for the majority hospitalisations with RTIs accounting for 37.7% of cases, other bacterial and parasitic infections for 19.8%, and gastrointestinal disorders for 10.2%.
We observed a high rate of LRTI and influenza in hospitalised children. Previous studies in Vietnam showed that respiratory syncytial virus, enterovirus/rhinovirus, parainfluenza virus and adenovirus were frequently associated with LRTI [18–23]. Bacteria classically described to cause community-acquired pneumonia in Vietnamese children include Streptococcus pneumoniae, Hib and Staphylococcus aureus [24]. The conjugated Hib vaccine was introduced in the expanded immunisation programme in 2006 and the prevalence of Hib has subsequently declined dramatically [24]. Vaccination against invasive pneumococcal diseases, by contrast, is not covered by social security health insurance in Vietnam. In our study, the prevalence of atypical pneumonia was not available. A previous study on 722 hospitalised Vietnamese children [25], showed that atypical pathogens were identified in 29.8% of cases, mainly Mycoplasma pneumoniae (26.3%). Viral and virus-bacteria co-infections were frequently detected in children with LRTI [18–21,25].
The decrease in newly diagnosed cases of tuberculosis may reflect a decline in tuberculosis incidence in Vietnam, as a result of several programmatic improvements that have been made, such as vaccination. The significant increase in the prevalence of influenza seen in 2019 may be due to annual variation in influenza incidence but is most likely related to a better availability of influenza-specific PCR. This suggests that laboratory facilities not only play an important role in the definitive and differential diagnosis of ID, but also helps in identifying the true pattern of diseases on which to base priorities in terms of therapeutic needs in the hospital.
In diarrhoeal Vietnamese children, rotavirus was the pathogen most commonly detected with a prevalence of 50.0% [26–28]. The cost of the rotavirus vaccine is not covered by Vietnamese government. It is expensive and access is difficult for children living in rural areas. Furthermore, norovirus, diarrhoeagenic Escherichia coli, Salmonella spp. and Shigella spp. were also frequently associated with diarrhoea in Vietnamese children [26–28]. Risk factors for diarrhoea in Vietnamese children include, as in many settings, male gender, under the age of 2, and poor socioeconomic indicators such as household overcrowding and poor hygienic conditions [27]. Improvements in sanitation, in food and water quality are likely to alter the incidence of rotavirus diarrhoea in small children. Moreover, the rotavirus vaccine is targeted for introduction into the expanded immunisation programme to prevent disease [29].
World-wide, malaria is one of the most frequent IDs in children [30]. In our study, no case of malaria was reported over the 5-year period of inclusion. In Vietnam, malaria incidence dramatically decreased by 94.9% from 1992 to 2014 thanks to the widespread use of artemisinin derivatives and impregnated mosquito nets [31]. No cases of malaria were identified in Thai Binh in 2014 [31].
Antibiotic overuse is an important contributor to the development of antibiotic resistance world-wide. In low-income countries or poor settings, antibiotic prescription is particularly high, because of the fear of bacterial systemic infections when faced with non-specific febrile signs [32]. In a systematic review, Donà et al. [33] showed that between 20% and 50% of antibiotic prescriptions in children are potentially unnecessary or inappropriate. Many children still receive broad-spectrum antibiotics for viral infections or antibiotic courses that are significantly longer than needed [33,34]. Hoa et al. conducted a study about knowledge of antibiotics and reported the practices of 96 healthcare providers regarding antibiotic use for respiratory infections among children. Only 19% had overall knowledge in line with recommended guidelines, and antibiotics were often prescribed or dispensed to treat common colds [35].
The overall hospital mortality rate was lower than reported in other Vietnamese studies. A retrospective survey of 12,389 paediatric emergency visits showed that mortality was 1.1% [17]. An 8.6% mortality rate was reported in neonates [36]. The lower mortality rate observed at the Thai Binh Paediatric Hospital may be explained by the referral of more severe cases to the National Hospital of Paediatrics, in Hanoi (12.0%). Moreover, due to cultural habits, some Vietnamese people do not want their family members to die at the hospital but at home, some parents of seriously ill children (0.1%) applied for hospital discharge against medical advice. Mortality data for these patients were not available. Furthermore, most children who died came from rural areas, suggesting that they may not have had easy and early access to hospital treatment.
Our study has some limitations. The study was retrospective and lack microbiological documentation in most cases of infections. The study did not capture information about socioeconomic conditions, environmental factors and living conditions at home. Furthermore, the time between onset of symptoms and hospitalisation was not available. Finally, no distinction was made between initial visits and readmission of the same patients. Nevertheless, this data serves as a basis for the identification of needs for diagnostic tools and for future evaluation of the effect of targeted implementations of such facilities. The data also helps in designing standardised protocols for the proper management of the most common diseases presenting in this hospital and to strategically provide the necessary equipment for child healthcare in economically limited conditions. Further studies aimed at identifying the pathogens frequently responsible for infections in children hospitalised at the Thai Binh hospital should be conducted. Based on these results, point-of-care tests, including real-time PCR assays to identify common pathogens should be implemented for more accurate diagnosis and more appropriate antibiotic use.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
TDP, VTH, TLD and PG contributed to the experimental design. TDP, VTH, TLD, XDT, DLP, MMT, VND, VKD, TTD, NTN, TTV, TLV and TMCN collected the data. TDP, VTH, TLD, XDT, DLP, MMT, VND, VKD, TTD, TTV, TLV and TMCN analysed the data. TDP, VTH, TLD, PM and PG contributed to interpretation and writing. DTN, NTN, DCN, NTH, TLV, TMCN and PM contributed to critically reviewing the manuscript. TDP and VTH contributed equal work PG coordinated the work.
FUNDING
No financial support was provided.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Thi Dung Pham AU - Van Thuan Hoang AU - Thi Loi Dao AU - Xuan Duong Tran AU - Duc Long Phi AU - Minh Manh To AU - Van Nghiem Dang AU - Van Khoi Dang AU - Thanh Tung Dao AU - Nam Thang Nguyen AU - Thi Thuy Vu AU - Duc Thanh Nguyen AU - Duy Cuong Nguyen AU - Nang Trong Hoang AU - Thanh Liem Vu AU - Thi Minh Chinh Nguyen AU - Philippe Minodier AU - Philippe Gautret PY - 2020 DA - 2020/07/29 TI - Morbidity and Mortality Patterns in Children Admitted to Hospital in Thai Binh, Vietnam: A Five-year Descriptive Study with a Focus on Infectious Diseases JO - Journal of Epidemiology and Global Health SP - 69 EP - 75 VL - 11 IS - 1 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.200723.001 DO - 10.2991/jegh.k.200723.001 ID - Pham2020 ER -