
Clinical Characteristics and Outcome of Hospitalized COVID-19 Patients in a MERS-CoV Endemic Area
 , AbdulEllah AlMohaya1, , Ali AlHijji1, , Layan Akkielah1, Abdulaziz AlRajhi1, Fahad Almajid1, Aynaa Alsharidi1, Fatimah S. Al-Shahrani1, Naif H. Alotaibi1, , Awadh Alanazi1, Leen Ghonem2, Abdulkarim Alhetheel3, Sarah Alsubaie4, Ziad A. Memish5, 6, *,
, AbdulEllah AlMohaya1, , Ali AlHijji1, , Layan Akkielah1, Abdulaziz AlRajhi1, Fahad Almajid1, Aynaa Alsharidi1, Fatimah S. Al-Shahrani1, Naif H. Alotaibi1, , Awadh Alanazi1, Leen Ghonem2, Abdulkarim Alhetheel3, Sarah Alsubaie4, Ziad A. Memish5, 6, *, - DOI
- 10.2991/jegh.k.200806.002How to use a DOI?
- Keywords
- COVID-19; SARS-CoV-2; clinical; outcome; Saudi Arabia
- Abstract
Background: The Kingdom of Saudi Arabia (KSA) reported 170,639 cases and 1430 deaths from COVID-19 since the first case emerged in the country on March 2 through June 25, 2020. The objective of this report is to describe the characteristics and outcome observed among 99 hospitalized COVID-19 patients in the largest academic hospital in KSA, and assess co-infection with the Middle East Respiratory Syndrome Coronavirus (MERS-CoV).
Methods: This single-center case series data included select epidemiological, clinical, radiological features and laboratory findings of all confirmed hospitalized cases of COVID-19 in King Saud University Medical City (KSUMC), Riyadh, KSA, from March 22 until May 31, 2020, followed through June 6, 2020. We conducted retrospective analysis of listed data from 99 hospitalized patients and present characteristics and factors associated with severity in percentages and univariate odds ratios. Cases were confirmed using nasopharyngeal or throat swab by real-time Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and MERS-CoV by RT-PCR.
Results: The 99 hospitalized COVID-19 patients included in this analysis constitute 16% of 632 positive SARS-CoV-2 among 6633 persons who were tested at the KSUMC (positivity rate, 9.4%). MERS-CoV PCR was negative in all 99 patients tested. The majority of these 99 hospitalized patients were males (66%), had a mean age of 44 years (range, 19–87), and a quarter (25.3%) were health care workers. Patients with comorbid conditions accounted for 52.5% of patients including the 8.1% who were asymptomatic; diabetes mellitus being the most frequent (31.3%), followed by hypertension (22.2%). The most common presenting symptoms were fever (67.7%), cough (60.6%), dyspnea (43.4%), upper respiratory symptoms (27.3%), fatigue (26.3%), diarrhea (19.2%) and loss of smell (9.1%). The clinical conditions among these 99 patients included upper respiratory tract infection (47.5%), abnormal chest X-ray, lymphopenia, high inflammatory markers a fifth (21%) of patients had moderate pneumonia, while 7% had severe pneumonia with 22.2% requiring admission to the intensive care unit and 12.1% died. Late presentation with severe disease, an abnormal chest X-ray, lymphopenia, high inflammatory markers (C-reactive protein, ferritin, and procalcitonin), and end organ damage (high creatinine or high aspartate aminotransferase) were predictors for admission to critical care unit or died.
Conclusion: We observed no MERS-CoV co-infection in this early cohort of hospitalized COVID-19 patients who were relatively young, more than half had comorbid conditions, presented with fever and/or cough, an abnormal chest X-ray, lymphopenia, and high inflammatory markers. Given MERS-CoV endemicity in the country, co-monitoring of MERS-CoV and SARS-CoV-2 coinfection is critical.
- Copyright
- © 2020 The Authors. Published by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
The Kingdom of Saudi Arabia (KSA) is home to two of the circulating beta coronaviruses, Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and SARS-CoV-2 the causative agent of the COVID-19 pandemic. MERS-CoV was first discovered in KSA in September 2012 [1] and has subsequently spread to 27 countries. Of the global total of the reported 2949 laboratory-confirmed cases through June 1, 2020, 74% (2167) cases including 842 deaths were reported by KSA [2,3]. SARS-Cov-2, first reported in China in December 2019 [4], received pandemic status on March 11, 2020 [5], and since has caused over 10 million cases and over half a million deaths worldwide [6]. In KSA, the first case of COVID-19 was reported on March 2, 2020 [7,8]; three different seeding patterns helped its spread to all areas and municipalities [9]. With 170,639 cases including 1430 deaths [10] by June 25, 2020, KSA is among the top 20 countries with highest total confirmed COVID-19 cases [6]. The overall Case Fatality Rate (CFR) in KSA (0.70%), is much lower than that reported in other countries such as the USA (5.68%) and the UK (14.12%) [6]. Immunity due to past MERS-CoV exposure [11] could be a potential reason. To describe the clinical picture of COVID-19 in KSA and assess potential interaction between MERS-CoV and SARS-CoV-2 infections, we reviewed data from hospitalized patients in the largest academic teaching hospital in KSA that serves also as a referral center for MERS-CoV. We describe the demographic, clinical characteristics and outcome in their 99 hospitalized COVID-19 infected patients and the outcome of MERS-CoV tests.
2. MATERIALS AND METHODS
2.1. Patients
We used routinely collected line listed data from patients admitted to King Saud University Medical City (KSUMC) in Riyadh from March 22, 2020, the day the first COVID-19 case was confirmed in the hospital, until May 31, 2020. Hospitalized patients are drawn from SARS-CoV-2 tests done at KSUMC, and only summary data are available on outcome among non-hospitalized patients. We included all consecutive adult individuals aged 18 years or older, who were hospitalized for at least 24 h with confirmed COVID-19 during the study period. Patients who were still hospitalized by end of study period were followed till discharge or death on or before June 6, 2020. All patients underwent SARS-CoV-2 and MERS-CoV Polymerase Chain Reaction (PCR) testing upon admission.
All patients were admitted to single rooms under droplet and contact precautions as per hospital policy, but they were placed in airborne infection isolation rooms with 6–12 air-changes per hour, or, when not available, in a single room with high efficiency particulate air filter, if aerosol generating medical procedure were required with the use of fit-tested N95 masks.
This analysis received ethical approval from KSUMC Institutional Review Board bearing project number E20-4979. Oral informed consent was obtained for data use from all study participants.
2.2. Laboratory Tests
All hospitalized patients underwent a nasopharyngeal and/or throat swab upon admission, when obtained, it was sent in viral transport medium (Copan, Brescia, Italy). We defined confirmed COVID-19 as a positive result for both SARS-CoV-2 E and S genes using the RealStar® SARS-CoV-2 real-time Reverse Transcriptase PCR (RT-PCR) kit (Altona®-Diagnostics, Hamburg, Germany) and Rotor-gene Q system (Qiagen®, Santa Clarita, CA, USA) in our institute’s molecular laboratory. We confirmed a sample with Cycle Threshold (Ct) value ≤29 for both SARS-CoV-2 E and S genes as positive case, whereas a sample with a single gene detection or Ct value ≥29 is confirmed by repeating the test on Xpert® Xpress SARS-CoV-2 kit and GeneXpert XVI system (Cepheid®, Sunnyvale, CA, USA) which detect SARS-CoV-2 E and N genes. We used the same nasopharyngeal/throat swab samples to test for MERS-CoV RNA in which, after extraction, the RNA was reverse transcribed to cDNA which then amplified and screened for the detection of MERS-CoV upE and orf1a genes using the specific primers and probes of the RealStar® MERS-CoV RT-PCR kit (Altona®-Diagnostics) on the Rotorgene Q instrument (Qiagen®).
2.3. Data Collection
Patient data maintained in the individual electronic health care records of all confirmed COVID-19. Information recorded in health care records include demographic data, medical history, epidemiological exposure, underlying comorbidities, symptoms, signs, laboratory results, coinfection with MERS-CoV, bacterial cultures results, chest X-rays and Computed Tomographic (CT) scans, treatment measures (i.e., antiviral therapy, corticosteroid therapy, monoclonal antibody treatment, supportive care), in-hospital complications, need of Intensive Care Unit (ICU), and clinical outcome. The Sequential Organ Failure Assessment (SOFA) was determined on the day of ICU admission.
We classified disease severity based on the Saudi Ministry of Health severity definitions [12] into asymptomatic, upper respiratory tract illness, mild to moderate pneumonia, severe pneumonia (in which invasive or non-invasive ventilation was needed), and critical cases (in which acute respiratory distress syndrome (ARDS), overt sepsis, or multiorgan dysfunction were documented).
2.4. Statistical Analysis
Continuous measurements are presented as mean (SD) if they are normally distributed or median [Interquartile range (IQR)] if they are not, and categorical variables as count in percentages. For laboratory results, we assessed whether the measurements were outside the normal range. We used SPSS software (version-23, IBM Corp., Armonk, NY, USA) for statistical analysis including a univariate analysis to obtain odds ratio (OR) and 95% confidence interval (CI) on association of the study variables with poor outcome. Due to small sample size, we did not conduct a multivariate analysis.
3. RESULTS
During the study period, 9.4% (632) of the 6633 patients tested at KSUMC for COVID-19 by RT-PCR were positive. Of these 632 patients, 99 (16%) were hospitalized and met the criteria for inclusion in our analysis. Among the 99 hospitalized patients, the median age was 44 years (range, 19–87), the majority were men (66%), aged 65 years or younger (90%), and Saudi nationals (54%). One-fourth of cases (25%) were healthcare workers. Patients with comorbid illnesses represented 53%; body mass index >30 kg/m2 (37%), diabetes mellitus (31%), hypertension (22%), cardiovascular disease (12%), lung disease (COPD, asthma) (7%), dyslipidemic (6%), kidney disease (2%) and others (23%). Medication history included the use of ACE inhibitors (14%) and statins (17%). Median duration of symptoms was 4 days with the majority (80%) presenting within 7 days of symptoms onset. The three most common symptoms included fever (68%), cough (61%), and dyspnea (43%) (Figure 1).
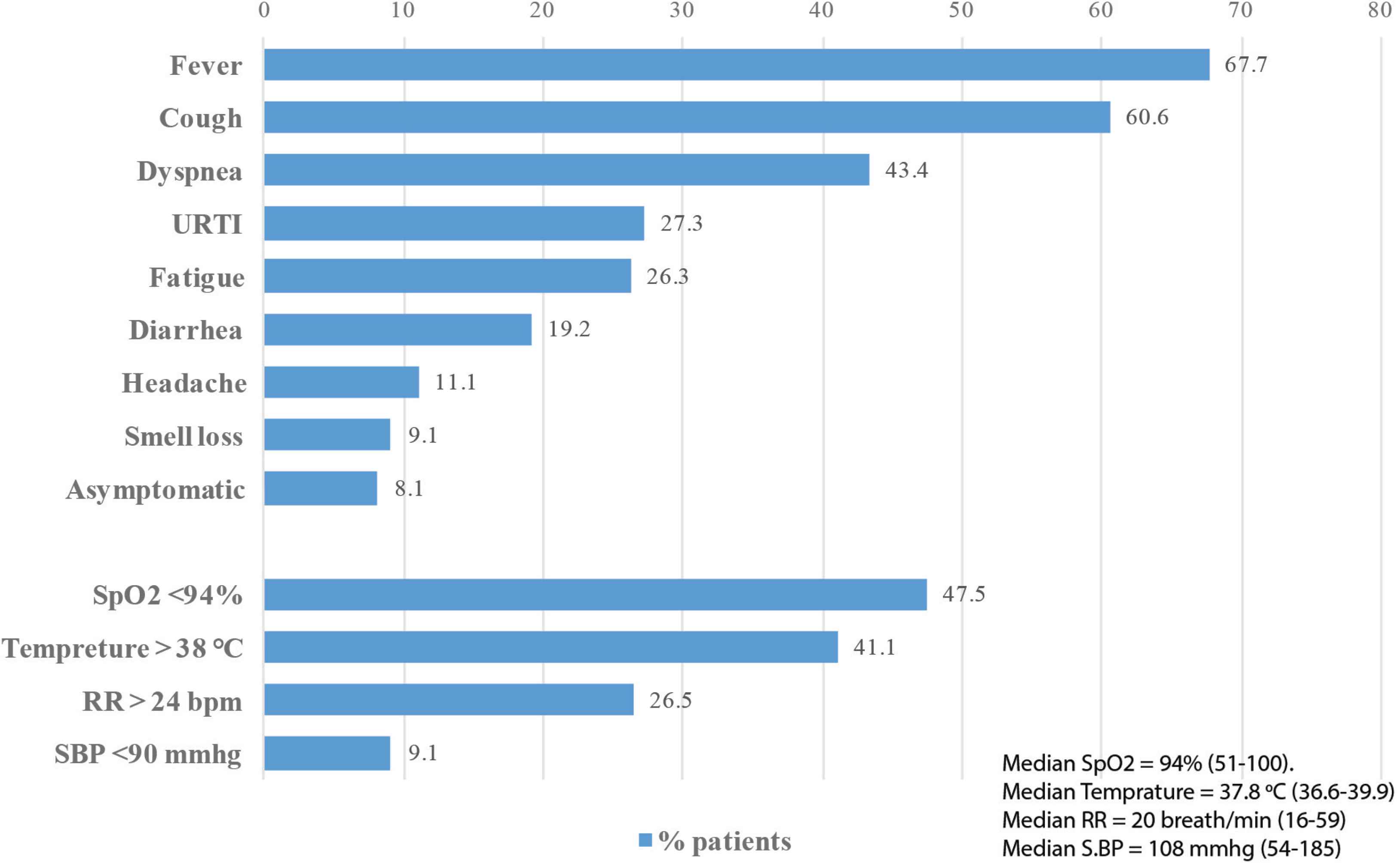
Clinical presentation* of hospitalized COVID-19 patients, King Saud University Medical City, Saudi Arabia. *Median duration of symptoms = 4 (range 1–28) days. SpO2, pulse oximetry; RR, respiratory rate; bpm, breath per minute; SBP, systolic blood pressure.
Exposure history revealed that 46% of COVID-19 patients were unable to provide their exposure history, 30% had close contact with a confirmed case in KSA, 1% was acquired overseas, and 23% were hospital acquired.
Twenty-one patients acquired infections from a single hospitalized index case that was unrecognized at the time of admission due to neurological presentation and COVID-19 was suspected only when the patient developed fever during hospital stay. Among the 25 health care workers with COVID-19 infections, 8% were community acquired, and 88% (23) were hospital acquired. Of the 23 hospital acquired cases, seven were physicians (30%), and 16 were nurses (70%). Of the two additional infected nurses were secondary transmission from a single nurse.
On admission, 22% of patients required ICU admission, and more than half of those (54%) were direct admission to the ICU (Table 1). Overall, 41% of patients had fever above 38°C, about one half (48%) had evidence of hypoxia (SpO2 < 94%) and a quarter (27%) had tachypnea (respiratory rate > 24 breaths per minute). MERS-CoV PCR was negative in all 99 patients tested. Most common laboratory abnormalities within 24 h of hospitalization were high
| Variables | Count (%) | Death in ICU n = 11 (50%) |
|---|---|---|
| Initial admission | ||
| Ward | 10 (45.5) | 2 (20) |
| ICU | 12 (54.5) | 9 (75) |
| Temperature, highest pre-ICU admission (°C) | ||
| ≥38 | 16 (72.7) | 10 (62.5) |
| <38 | 6 (27.3) | 1 (16.7) |
| SOFA score* | ||
| ≥4 | 11 (50) | 8 (72.7) |
| <4 | 11 (50) | 3 (33.3) |
| PF ratio** | ||
| ≤100 | 13 (59.1) | 10 (76.9) |
| >100 | 9 (40.9) | 1 (11.1) |
| Need for vasopressors | ||
| Yes | 14 (63.6) | 11 (78.6) |
| No | 8 (36.4) | 0 (0) |
| Respiratory support | ||
| Facemask (FM) | 1 (4.5) | 0 (0) |
| High Flow Nasal Cannula (HFNC) | 8 (36.4) | 0 (0) |
| Mechanical Ventilation (MV) | 13 (59.1) | 11 (84.6) |
| Duration of MV (median) | 5 days | |
The Sepsis-related Organ Failure Assessment (SOFA).
Horowitz index (P/F ratio), mmHg, PaO2/FiO2.
Clinical characteristics for 22 patients in Intensive Care Unit (ICU), King Saud University Medical City, Saudi Arabia
| Study variables | Number of patients | Median (IQR) | Abnormal | |
|---|---|---|---|---|
| Cutoff | n (%) | |||
| Basic investigations | ||||
| White blood cells (×109/L) | 99 | 5.6 (4.4) | <4 | 23 (23.2) |
| Lymphocytes (×109/L) | 94 | 1.1 (0.35) | <1 | 34 (37.4) |
| |
88 | 0.6 (0.65) | >0.45 | 60 (68.2) |
| ALT (units/L) | 88 | 37 (58.75) | >61 | 17 (19.1) |
| AST (units/L) | 61 | 28 (59) | >37 | 23 (37.7) |
| Serum creatinine (μmol/L) | 95 | 76 (38) | >115 | 8 (8.1) |
| Random Blood Sugar (RBS) (μmol/L) | 96 | 6 (4.1) | >5.83 | 53 (55.2) |
| <4.07 | 1 (1.1) | |||
| Inflammatory markers | ||||
| Lactate (mmol/L) | 29 | 1.4 (0.9) | >2 | 6 (20.7) |
| Ferritin (mcg/L) | 83 | 309 (1246) | >400 | 40 (48.2) |
| C-reactive Protein (CRP) (mg/L) | 63 | 40.50 (61.3) | >20 | 43 (68.3) |
| Procalcitonin (PCT) (ng/mL) | 25 | 0.11 (0.44) | >0.5 | 4 (16) |
| Interleukin-6 (IL-6) (pg/mL) | 16 | 70.18 | >7 | 15 (93.8) |
| Troponin (ng/L) | 50 | 7.50 (185) | >100 | 2 (4) |
| Creatinine Kinase (CK) (units/L) | 32 | 160.50 | >308 | 12 (37.5) |
| ECG: QT interval (ms) | 16 | 445 (1109) | >440 | 12 (80) |
| Microbiology | ||||
| MERS-CoV RT-PCR | 99 | Positive | 0 (0) | |
| HIV Ag/Ab | 45 | Positive | 0 (0) | |
| Hepatitis BsAg | 51 | Positive | 0 (0) | |
| TB QuantiFERON Gold Plus | 29 | Positive | 1 (3.4) | |
| Sputum culture | 17 | Positive | 2 (11.8) | |
| Blood culture | 43 | Positive | 7 (16.3) | |
| Imaging | ||||
| Chest X-ray | 89 | Normal | 54 (60.7) | |
| Infiltration | 35 (39.3) | |||
| Unilateral | 7 (20) | |||
| Bilateral | 28 (80) | |||
| CT chest | 6 | Normal | 2 (33.3) | |
| GGO | 3 (50) | |||
| Infiltration | 1 (16.7) | |||
CT, computed tomography; GGO, ground glass opacity; ECG, electrocardiogram; HIV, human immunodeficiency virus; TB, tuberculosis; IQR, interquartile range; MERS-CoV, middle east respiratory syndrome coronavirus; RT-PCR, reverse transcription polymerase chain reaction; ALT, alanine aminotransferase; AST, aspartate aminotransferase.
Laboratory and radiological findings among COVID-19 cases, King Saud University Medical City, Saudi Arabia
Of the four pregnant women with COVID-19, three were asymptomatic and were detected from routine testing as per obstetric care policy. Two women delivered vaginally, the other two underwent cesarean sections, and all four babies were healthy and tested negative for COVID-19.
Non-ICU need for oxygenation was documented in 39 patients, with a median oxygenation duration of 3 days. Most patients received only supportive therapy, but 13 of the 99 cohort (13%) received at least one of the following agents: Hydroxychloroquine (HCQ), lopinavir/ritonavir, steroids, and/or tocilizumab (Table 3).
| Study variables | n (%) | Death, n = 12 (%) | Survived, n = 87 (%) |
|---|---|---|---|
| Diagnosis stratified based on experimental therapy | |||
| Asymptomatic | 8 (8.1) | 0 (0) | 8 (100) |
| - Hydroxychloroquine | 1 | 0 (0) | 1 (100) |
| Upper respiratory tract infection | 47 (47.5) | 0 (0) | 47 (100) |
| - Hydroxychloroquine | 3 | 0 (0) | 3 (100) |
| Mild/Moderate pneumonia | 21 (21.2) | 0 (0) | 21 (100) |
| - Hydroxychloroquine | 2 | 0 (0) | 2 (100) |
| - Lopinavir/ritonavir | 1 | 0 (0) | 1 (100) |
| - Supportive/Usual care | 18 | 0 (0) | 18 (100) |
| Severe pneumonia | 7 (7.1) | 1 (14.3) | 6 (85.7) |
| - Hydroxychloroquine, median = 5 days (IQR = 3.75) | 1 | 0 (0) | 1 (100) |
| - Steroids, median = 2 days (IQR = 11.5) | 1 | 1 (100) | 0 (0) |
| - Supportive/Usual care | 5 | 0 (0) | 5 (100) |
| Critical | 16 (16.2) | 11 (68.8) | 5 (31.3) |
| - Tocilizumab + HCQ + Steroids | 2 | 0 (0) | 2 (100) |
| - Tocilizumab + Steroids | 1 | 1 (100) | 0 (0) |
| - Tocilizumab alone | 1 | 0 (0) | 1 (100) |
| - Steroids alone | 4 | 4 (100) | 0 (0) |
| - Supportive/Usual care | 8 | 6 (75) | 2 (25) |
| Median duration | |||
| Hydroxychloroquine, median = 4 days (IQR = 3.75) | |||
| Other treatment | |||
| Antibacterial, median = 4 days (IQR = 5) | 53 (53.5) | ||
| Anticoagulant, median = 5 days (IQR = 8) | 94 (94.9) | ||
| - Deep venous thrombosis prophylaxis* | 87 (92.6) | ||
| - On anticoagulant already before COVID diagnosis | 4 (4.3) | ||
| - Therapeutic anticoagulants (ACS or suspected PE) | 3 (3.2) | ||
| - Anticoagulant related complications | 1 | ||
| - Anticoagulation related intracranial bleeding | 1 | ||
| Outcome | |||
| Death, median = 3 days | 12 (12.1) | ||
| Time to recovery, median (range) in days (n = 47) | 3 (1–32) | ||
| Time to discharge, median (range) in days (n = 87) | 5 (1–32) | ||
| Time to death, median (range) in days (n = 12) | 5.5 (1–28) | ||
| Discharged home/quarantine building, median = 5 days | |||
| - Interval until recovery, median = 3 days | 87 (87.9) | ||
IQR, interquartile range; ACS, acute coronary syndrome; PE, pulmonary embolism; HCQ, hydroxychloroquine.
Diagnosis, treatment, and outcome among hospitalized COVID-19 patients, King Saud University Medical City, Saudi Arabia
Case fatality rate among the 99 patients (12% overall) increased with ICU admission (50%). Poor outcome was highest among those with the SOFA score above four (8/11, 72.2%) and in patients requiring mechanical ventilation (11/13, 84.6%) (Table 3).
In the univariate analysis, intensive care unit admission and mortality were significantly associated with lymphopenia, high
| Study variables | ICU admission | Outcome | ||||||
|---|---|---|---|---|---|---|---|---|
| ICU, n = 22 (22.2) | No, n = 78 (77.8) | p | Univariate ratio (95% CI) (for ICU) | Death, n = 12 (12.1) | Survive, n = 87 (87.9) | p | Univariate ratio (95% CI) (for death) | |
| Age (years) | ||||||||
| ≥65 | 2 (9.1) | 8 (10.4) | 0.895 | – | 1 (8.3) | 9 (10.3) | 0.828 | – |
| <65 | 20 (90.9) | 69 (89.6) | – | 11 (91.7) | 78 (89.7) | |||
| Sex | ||||||||
| Female | 9 (40.9) | 25 (32.5) | 0.462 | – | 4 (33.3) | 30 (34.5) | 0.937 | – |
| Male | 13 (59.1) | 52 (67.5) | – | 8 (66.7) | 57 (65.5) | – | ||
| BMI | ||||||||
| ≤30 | 13 (61.9) | 48 (64.9) | 0.300 | – | 7 (58.3) | 54 (65.1) | 0.442 | – |
| 31–40 | 8 (38.1) | 20 (27) | – | 5 (41.7) | 23 (27.7) | – | ||
| >40 | 0 (0) | 6 (8.1) | – | 0 (0) | 6 (7.2) | – | ||
| HCW | ||||||||
| HCW | 1 (4.5) | 24 (31.2) | 0.011 | 0.105 (0.1–0.83) | 1 (8.3) | 24 (27.6) | 0.15 | – |
| Non-HCW | 21 (95.5) | 53 (68.8) | Ref | 11 (91.7) | 63 (72.4) | – | ||
| Medical history | ||||||||
| Medically free | 11 (50) | 36 (46.8) | 0.788 | – | 5 (41.7) | 42 (48.3) | 0.667 | – |
| Comorbidities | 11 (50) | 41 (53.2) | – | 7 (58.3) | 45 (51.7) | – | ||
| PCR Ct | ||||||||
| Ct value ≤24 | 10 (50) | 40 (56.3) | 0.615 | – | 7 (58.3) | 43 (54.4) | 0.8 | – |
| Ct value >24 | 10 (50) | 31 (43.7) | – | 5 (41.7) | 36 (45.6) | – | ||
| Epi link | ||||||||
| Close contact | 4 (18.2) | 26 (33.8) | 0.161 | – | 2 (16.7) | 28 (32.2) | 0.273 | – |
| Other/unknown | 18 (81.8) | 51 (66.2) | – | 10 (83.3) | 59 (67.8) | – | ||
| WBC | ||||||||
| Leukopenia | 2 (9.1) | 21 (27.3) | 0.075 | – | 1 (8.3) | 22 (25.3) | 0.192 | – |
| No | 20 (90.9) | 56 (72.7) | – | 11 (91.7) | 65 (74.7) | – | ||
| Lymphocytes | ||||||||
| Lymphopenia | 16 (76.2) | 18 (25.7) | <0.001 | 9.24 (2.96–28.86) | 10 (83.3) | 24 (30.4) | <0.001 | 11.458 (2.33–56.31) |
| No | 5 (23.8) | 52 (74.3) | Ref | 2 (16.7) | 55 (69.6) | Ref | ||
| High | 18 (90) | 42 (61.8) | 0.017 | 5.571 (1.19–26.0) | 10 (83.3) | 50 (65.8) | 0.225 | – |
| Normal | 2 (10) | 26 (38.2) | Ref | 2 (16.7) | 26 (34.2) | – | ||
| AST | ||||||||
| High | 12 (70.6) | 10 (23.3) | 0.001 | 7.92 (2.25–27.94) | 7 (70) | 15 (30) | 0.017 | 5.44 (1.24–23.96) |
| No | 5 (29.4) | 33 (76.7) | Ref | 3 (30) | 35 (70) | Ref | ||
| Creatinine | ||||||||
| High | 5 (22.7) | 3 (4.1) | 0.006 | 6.86 (1.49–31.68) | 5 (41.7) | 3 (3.6) | <0.001 | 19.048 (3.75–96.88) |
| No | 17 (77.3) | 70 (95.9) | Ref | 7 (58.3) | 80 (96.4) | Ref | ||
| RBS | ||||||||
| High | 16 (72.7) | 37 (50) | 0.06 | – | 11 (91.7) | 42 (50) | 0.007 | 11.0 (1.36–89.05) |
| No | 6 (27.3) | 37 (50) | – | 1 (8.3) | 42 (50) | Ref | ||
| Lactate | ||||||||
| High | 4 (23.5) | 2 (16.7) | 0.065 | – | 5 (50) | 1 (5.3) | 0.005 | 18.0 (1.69–191.52) |
| No | 13 (76.5) | 10 (83.3) | – | 5 (50) | 18 (94.7) | Ref | ||
| Ferritin | ||||||||
| High | 15 (83.3) | 25 (38.5) | 0.001 | 8.0 (2.1–30.45) | 10 (90.9) | 30 (41.7) | 0.002 | 14 (1.7–115.28) |
| No | 3 (16.7) | 40 (61.5) | Ref | 1 (9.1) | 42 (58.3) | Ref | ||
| CRP | ||||||||
| High | 14 (100) | 29 (58) | 0.03 | 21.14 (1.19–374) | 7 (100) | 36 (63.2) | 0.143 | – |
| No | 0 (0) | 21 (42) | Ref | 0 (0) | 21 (36.8) | – | ||
| PCT | ||||||||
| High | 4 (36.4) | 0 (0) | 0.06 | – | 3 (50) | 1 (5.3) | 0.027 | 18 (1.38–235.69) |
| No | 7 (63.6) | 14 (100) | – | 3 (50) | 18 (94.7) | ref | ||
| IL-6 | ||||||||
| High | 10 (90.9) | 5 (100) | 0.486 | – | 5 (83.3) | 10 (100) | 0.182 | – |
| No | 1 (9.1) | 0 (0) | – | 1 (16.7) | 0 (0) | – | ||
| CXR on arrival | ||||||||
| Infiltration | 17 (77.3) | 18 (26.9) | <0.001 | 9.26 (2.98–28.77) | 9 (75) | 26 (33.8) | 0.007 | 5.88 (1.47–23.61) |
| Normal | 5 (22.7) | 49 (73.1) | Ref | 3 (25) | 51 (66.2) | Ref | ||
| ICU admission | ||||||||
| Yes | – | – | – | – | 11 (91.7) | 11 (12.6) | <0.001 | 76.0 (8.92–647.60) |
| No | – | – | – | – | 1 (8.3) | 76 (87.4) | Ref | |
| Severity | ||||||||
| Severe/critical | – | – | – | – | 12 (100) | 11 (13.8) | <0.001 | 151 (8.36–2731) |
| Mild/moderate | – | – | – | – | 0 (0) | 69 (86.3) | Ref | |
Leucopenia (<4), lymphopenia (<1), high
RBS, random blood sugar; Epi, epidemiology; OR, odds ratio; CI, confidence interval; HCW, health-care worker; ICU, intensive care unit; CXR, chest X-ray; Ref, reference value; IL-6, interleukin-6; PCT, procalcitonin.
Factors associated with intensive care unit admission and outcome among COVID-19 patients, King Saud University Medical City, Saudi Arabia*
4. DISCUSSION
This first detailed COVID-19 case series in KSA revealed that one-tenth of COVID-19 tests were positive and 16% required hospitalization. Of the hospitalized patients, 22% required ICU care. COVID-19 case fatality rate was 0.2% among all those who tested positive at this hospital, 12% among the hospitalized, and 50% among those admitted to the ICU. The hospitalized COVID-19 patients had no coinfection with MERS-CoV.
Clinical presentation of patients with COVID-19 is variable between country reports. Compared to the high percentage of fever reported early from China (90%) during their peak of the epidemic, our cohort had a lower percentage of fever similar to the observation of 31% in New York, USA and 45% in Europe [13]. This difference is likely due to increasing awareness about other symptoms which lead to early diagnosis. Similar to SARS [14] and MERS [15], patient’s age, comorbid conditions and certain laboratory abnormalities were associated with poor in-hospital outcomes in COVID-19 patients [16]. Underlying chronic medical conditions are commonly reported in hospitalized COVID-19 patients with variable proportions between studies probably due to variable hospitalization criteria (94% in USA, 77% in UK, 23% in China, 20% in KSA) [17–19]. COVID-19 fatality rate among the hospitalized cases in this cohort is within the reported 12–15% range [20,21]. The mortality among our critically ill cases (50%) was similar to case series from Seattle, USA (50%) [22] and from Wuhan, China (52%) [23] but was higher than in New York, USA (39%) [24]. Low COVID-19 mortality both overall and among the hospitalized patients may be due to relatively younger age of the Saudi population (≥65 years, 3%); and in our cohort one fourth of patients were young health care workers, asymptomatic for COVID-19, in which infection was detected through contact tracing, and are less likely to have co-morbidities. Potential benefit from past exposure to MERS-CoV cannot be ruled out. With a 50% genomic similarity between these two beta-coronaviruses, MERS-CoV exposure may provide partial immunity against severe disease [25].
Inflammatory markers, which have been widely used in diagnosing infections and predict disease progression [26], were investigated in several reports since the beginning of the COVID-19 pandemic. CRP, which is a protein produced by the liver, was found to be a relatively good predictor for the development of pneumonia in MERS-CoV infections [27] and has recently been found to be a valuable marker to anticipate the possibility of aggravation of non-severe adult COVID-19 patients, with an optimal threshold value of 26.9 mg/L [28]. This association is also replicated in our cohort, in which we found an above-normal CRP is associated with severe disease requiring ICU admission (OR = 21.1, 95% CI: 1.19–374) but was not associated with mortality (p-value = 0.143). Other markers were reported to be helpful in predicting COVID-19 disease progression, namely, high
Similar to MERS-CoV, no high-quality evidence nor consensus agreement on directed therapy against COVID-19 has been established. Experimental therapies including HCQ, remdesivir, triple therapy (interferon-β 1b, lopinavir/ritonavir, and ribavirin) and favipiravir, which showed a potential in-vitro activity against SARS-CoV-2 with some anecdotal low/medium quality evidence in clinical trials [32–34]. The best current approach is with source control of infection, proper use of personal protective equipment, early diagnosis and isolation of cases, with rapid contact tracing and quarantine, with supportive care for patients. Although from the 99 patients only nine had positive bacterial cultures; two from sputum and seven from blood with only one of those blood cultures considered a true pathogen; 53 (53.5%) patients received antibacterial therapy for a median of 4 days.
In summary, despite the limitation of the small sample size and data emerging from a single center, this case series describing clinical characteristics and outcome of hospitalized COVID-19 patients in a MERS-CoV endemic country. In this relatively young cohort, the most common presenting symptoms were fever and/or cough, while diabetes and hypertension were the most common comorbid conditions. Severe disease, abnormal chest X-ray on admission, lymphopenia, raised inflammatory markers (CRP, ferritin, and procalcitonin), and end organ damage (high creatinine or high AST) were associated with poor prognosis. Large sample case series will help us confirm the generalizability of these findings.
Limited published data has emerged from MERS-CoV endemic areas, larger scale prospective studies with serological testing of MERS-CoV for COVID-19 infected individuals is needed to help determine the role of past exposure to the former coronavirus with COVID-19 disease progression and severity.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
MB contributed in idea, concept, proposal, data interpretation, manuscript writing, final approval. AbdulEllah A contributed in idea, concept, proposal, data collection, data entry, data analysis, manuscript writing, final approval. Ali A contributed in idea, concept, proposal, data collection, manuscript writing, final approval. FA contributed in idea, concept, manuscript editing, final approval. Aynaa A contributed in idea, concept, manuscript editing, final approval. FSA contributed in idea, concept, manuscript editing, final approval. NHA contributed in idea, concept, manuscript editing, final approval. Awadh A contributed in idea, concept, manuscript editing, final approval. LG contributed in idea, concept, manuscript editing, final approval. Abdulkarim A contributed in sample selection, microbiology diagnostics, manuscript writing and final approval. SA contributed in idea, concept, manuscript editing, final approval. ZAM contributed in idea, concept, data interpretation, manuscript writing, final approval.
FUNDING
No financial support was provided.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Mazin Barry AU - AbdulEllah AlMohaya AU - Ali AlHijji AU - Layan Akkielah AU - Abdulaziz AlRajhi AU - Fahad Almajid AU - Aynaa Alsharidi AU - Fatimah S. Al-Shahrani AU - Naif H. Alotaibi AU - Awadh Alanazi AU - Leen Ghonem AU - Abdulkarim Alhetheel AU - Sarah Alsubaie AU - Ziad A. Memish PY - 2020 DA - 2020/08/21 TI - Clinical Characteristics and Outcome of Hospitalized COVID-19 Patients in a MERS-CoV Endemic Area JO - Journal of Epidemiology and Global Health SP - 214 EP - 221 VL - 10 IS - 3 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.200806.002 DO - 10.2991/jegh.k.200806.002 ID - Barry2020 ER -