
Narrative Review of Infection Control Knowledge and Attitude among Healthcare Workers
Research Center, Almoosa Specialist Hospital, Saudi Arabia
- DOI
- 10.2991/jegh.k.201101.001How to use a DOI?
- Keywords
- Infection; knowledge and awareness; staff attitudes; healthcare workers; sharps injuries
- Abstract
Background: Infection is one of the major threats to Healthcare Workers (HCW) worldwide. It exposes HCW to more than 20 kinds of blood-borne pathogen infections, especially the most severe cases, namely Hepatitis B Virus (HBV), Hepatitis C Virus (HCV), and Human Immunodeficiency Virus (HIV). The impact of infection about HCWs’ health, clinical burden, national economic burden, and humanistic burden suggests the importance of further investigation and discussion on this topic.
Aims: This paper aimed to discuss literature on infection control knowledge and attitudes among HCWs and potential factors contributing to infection control.
Method: For this narrative review Proquest, Medline, and Up To Date have been utilized to search articles about infection control knowledge and attitudes among healthcare workers and potential factors contributing to infection control. The search was narrowed to article between 2000 and 2018. A total of 400 materials were initially identified to be potentially relevant for the review. A total of 28 articles were included, and they were found to match the inclusion criteria.
Results: Results from the reviewed studies showed that there was a high-level knowledge in terms of precautionary measures and compliance with needle safety precautions while staff attitude achieved above average. Weak positive correlation was found between staff attitude and precautionary measures, while moderate positive correlation was found between precautionary measures and compliance with needle safety precautions. Only precautionary measures were found to significantly influence compliance with needle safety precautions, in which higher precautionary measures, resulted in higher compliance with needle safety precautions.
- Copyright
- © 2020 Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Hospital injury posed a risk of getting Hepatitis B Virus (HBV), Hepatitis C Virus (HCV) and Human Immunodeficiency Virus (HIV) infection [1] by contact with infected blood, which has an estimated infection rate of 30.0%, 0.5%, and 0.3%, respectively [2]. World Health Organisation estimated that a total of 3 million out of 35 million Healthcare Workers (HCW) worldwide experienced percutaneous exposure to blood-borne pathogens each year, in which 2 million to HBV, 0.9 million to HCV, and 0.17 million to HIV [2]. Further, these infections can lead to low a quality of life, or even worse reduce life expectancy of the infected person, as well as incurring substantial costs in the long run [3]. Beyond the health risk, some studies highlighted the national economic burden caused by infection [4,5]. Also, a study by Hanmore et al. [4] listed the type of cost for infection post-exposure management which encompassed (a) infection test on injured HCWs and, if known, trace the source to patient, (b) post-exposure prophylaxis to prevent and manage potential blood-borne-virus transmission, (c) short- and long-term treatment if HCWs were infected by chronic blood-borne virus, (d) staff absence and replacement, (e) counselling for injured workers, and (f) legal cost including litigation and compensation claims. A systematic review conducted by Wright [6] on eight data-driven studies and six modelling studies showed that infection generate significant potential, intangible direct and indirect, costs, and possibly increasing over time. Apart from that, infection was also found to be contributing to serious humanistic or mental burden if not well managed, as discovered by many studies. Some studies [4,7] highlighted the major psychological effects experienced by HCWs after infection incidents, namely depressive symptoms, increasing tension in families, crying spells, adjustment disorder, anxiety and panic attacks, and stress such as post-traumatic stress disorder and excessive worry. Further, Gershon et al. [8] and Lee et al. [9] conducted a study on HCWs’ psychology after infection incident [8] found that as high as 66.4% of HCWs experience infection claimed to have mild to moderate anxiety, and 13.8% claimed to have persistent anxiety. Similarly, Lee et al. [9] revealed that a high percentage (53%) of HCWs reported anxiety due to their recent exposure to infection. Besides, it was reported by Lee et al. [10] that the humanistic and psychological burden of infection had led to HCWs lost productivity and work time in the US and Europe. The study had 110 US nurses reported a total of 77 days of lost time after infection, in which 13% of days were used to seek medical attention and treatment, 8% of days were used for HIV prophylactic medication, and 79% of days were due to anxiety following infection and emotional distress. Given the potential negative impacts brought to HCW, clinical burden and national economy as mentioned, it is important to review and assess the current prevalence of infection among healthcare workers. Furthermore, this paper will also focus on reviewing factors contributing to the infection so that some suggestions can be made to improve the quality of life among global HCW.
2. MATERIALS AND METHODS
This review is intended to discuss the relevant literature that has studied infection control knowledge and attitudes among HCWs and potential factors contributing to infection control. The literature was searched for on ProQuest, Medline, and Up To Date. The search was narrowed to articles between 2000 and 2018. The search terms were “infection control knowledge”, “attitudes of healthcare providers toward infection control” and “potential factors contributing to infection control” which showed 400 results. After adding the inclusion criteria, the total text was 221. Exactly 108 were included after reading the titles. Then, a total of 71 studies were included after reading the abstract. Eventually, after reading the full texts 28 articles were included based on the quality of the studies. Quality appraisal developed by DiCenso et al. [11] was utilized to evaluate the quality of the studies. Questions were on research problems, literature review research design, study sample, data collection, results, and limitation. The review was aimed to find answers to the following questions. What is the infection control knowledge and attitudes among HCWs? And what are the potential factors contributing to infection control?
3. FINDINGS
It is evident that the practice of preventing and eliminating infection is not a practice biased for a nation-specific effort, but rather a standard requirement globally. Infection presents an urgent drive to healthcare providers globally, particularly because of the hazards they imply as well as the impact of such hazards. While research indicates that such hazards can be easily prevented, reduced and even eliminated, the hazards are still becoming increasingly frequent and significant. The recent review has showed that contemporary knowledge on infection among healthcare providers is inadequate and even ignorant. This gap in knowledge needs to be filled with reliable and generalizable empirical findings, thus predisposing the proposed research undertaking. To date, there is a lack of such studies where most of the published studies focus on prevalence and under-reporting of infection, and risk factors associated with infection and prevention through education program [12]. The review on infection knowledge and attitude among HCWs has been divided as follows: safety measures of HCWs, lack of knowledge of HCWs, attitudes of HCWs toward infection control, precautionary measures, and compliance of needle stick and sharps injury safety.
3.1. Safety Measures
Several studies have been conducted on infection control safety measures of HCWs (Table 1). In a study [13] which investigated the occupational risk factors that emerged from infection among Ethiopian HCWs at Hawassa City, and highlighted how the injuries presented a significant problem in Ethiopian healthcare systems due to the associated risk of acquiring hepatitis C, hepatitis B, and HIV infections. It also highlighted the need of safety measures for HCWs who face the risk of infection, based on reliable research findings. Similarly occurrence, frequency, significance and impact of infection among HCWs have been acknowledged as an urgent problem across the globe that can and should be reduced, eliminated and even prevented [14]. Adoption of safety measures has deemed to be essential, since infection portend safety-threatening hazards that can jeopardize the working realities of healthcare personnel. Besides the adoption of protective equipment and positive attitude/awareness of healthcare, another effective safety measure identified and supported by previous empirical research is the use of safe devices (needles and sharps) [10,15].
| Authors | Sample | Methodology | Findings |
|---|---|---|---|
| Siddique et al. [19] | Ethiopian HCW | Questionnaire Survey | The needle stick injury rate in the study area was (#) 35.8%. |
| Khraisat et al. [21] | 226 Germany HCW | Self-reporting questionnaire | 31.4% of participant HCWs had sustained at least one needle stick injury in the last 12 months, ranging from (#) 46.9%. |
| Shiao et al. [23] | 168 registered active nurses | Cross-sectional study | Study finds out that facilities such as engineered safe devices are effective for prevention of NSI incidents among nurses. |
| Makary et al. [24] | 111 clinical nurses | Quantitative | More than half nurses have no experience about how to handle needle stick injuries. |
| Azadi et al. [25] | 434 dentist | Quantitative | High rate of NSSI and low rate of compliance. |
NSI, Needlestick injuries; NSSI, Needlestick and sharps injuries.
Prior literatures on safety measures of Healthcare Workers (HCWs)
3.2. Lack of Knowledge of Healthcare Workers
The lack of knowledge and awareness of infection control among HCWs in the literature has been linked to the worsening of the healthcare delivery outcomes [16]. A mini-systematic literature review on infection control argued that the hazards occurred in Saudi Arabia and across the globe was due to the lack of knowledge on how to prevent infection during healthcare delivery (Table 2). This inadequacy of contemporary knowledge on the hazards in Saudi Arabia was established by many researchers [16,17]. Immunization, healthcare providers’ education, and engineering control measures are all recommended examples of infection prevention and control [17]. HCWs often fail to report injuries to hospital administration to seek appropriate treatment. Studies also showed that HCWs often fail to report needle stick and sharps injuries because of the lack of knowledge on the efficacy of Post-Exposure Prophylaxis for prevention; other HCWs lack follow-up and have careless attitudes [18]. Such attitudes by HCWs trigger the frequency and occurrence of injuries have been linked in the literature to their lack of adequate knowledge on the risks, consequences, and prevention of infection. Because of this study, HCWs were deficient in knowledge on the nature, consequences, and prevention of infection. Thus required consistent awareness, training and education of HCWs to actively report and prevent needle stick injuries. Additionally, a previous research has indicated that the risk level of HCWs to increase, ignore and inadequately respond to needle stick and sharps injuries is primarily determined by their knowledge, competence and experience [18]. This knowledge incorporates knowing how to properly use the right equipment in the right occasions, understanding the policy protocols of the healthcare facility when preventing or responding to such injuries, knowing institution guidelines/requirements on where the equipment is used and how to dispose protocols and procedures of the used equipment.
| Authors | Sample | Methodology | Findings |
|---|---|---|---|
| Makary et al. [24] | 17 medical centre, 699 respondents | Survey | 99% of residents had a needle stick injury; 53% of injury involved high-risk patient due to lack of knowledge. |
| Siddique et al. [19] | Holy Family Hospital, Rawalpindi | Quantitative | Knowledge among HCWs regarding risks and hazards associated with NSI is inadequate. |
| Wilburn et al. [29] | Healthcare Workplace | Review paper | Reasons that HCWs do not report injuries include: lack of knowledge, careless, self-blame for their own injuries, lacks of follow-up and workers’ compensation. |
| Poznansky et al. [27] | (2007–2011) | Review paper | No knowledge about the reporting procedure. |
| Fashafsheh et al. [20] | 2014–2015 | Cross-sectional study | Nurses had fair knowledge level despite having good practice level regarding infection control. |
| 271 nurses |
Prior literatures on lack of knowledge of Healthcare Workers (HCWs)
3.3. Attitudes of Healthcare Workers toward Infection Control
Several research studies have linked staff attitudes to the occurrence, frequency and impact of infection among HCWs of a facility (Table 3). The study by Hashmi et al. [18] directly blamed the carefree and careless attitude of HCWs for infection prevention and post-injury intervention of needle stick injuries. In a recent study, Hashmi et al. [18] argued that carefree and ignorant staff attitudes are partially blamed for the prevalence of needle stick injuries and sharps injuries among HCWs who are currently working at Najran, Saudi Arabia. HCWs and hospital staff face higher risks due to their limited experience of clinical practices. Knowledge about needle sticks hazards and good practices are necessary for medical staff because they have to serve in the future. Therefore, it is important for them to learn how to protect themselves from occupational hazards, most importantly, infection. Infection is very common among hospital staff; therefore, acquiring knowledge and adopting professional attitude can make life safer [19]. Interestingly, this attitude is not only detectible among practicing HCWs. In another study, this carefree and ignorant attitude was also traced in training nurses. According to Fashafsheh et al. [20], the needle stick and sharps injury hazards are not merely significant among practicing healthcare personnel only, but it also starts from the very beginning of their training. Fashafsheh et al. [20] contend that an ignorant carefree attitude among HCWs causes an increase in the frequency and incidence of needle stick and sharps injuries, regardless of the significant risks and consequences the injuries often provoke. Ultimately, the ignorant and carefree attitude is among the “factors affecting career aspirations of medical students in Mangalore, India”, is questionable as that may be [5].
| Authors | Sample | Methodology | Findings |
|---|---|---|---|
| Rampal et al. [31] | 287 HCWs Serdang Hospital Malaysia | Quantitative | Majority were aware about universal precautions guidelines (96.5%) and that needle stick and sharps injuries need to be reported (99.1%). Thus, the study shows a positive attitude. |
| Swe et al. [12] | 316 medical students in Malaysia | Quantitative | Results reveal that student’s attitudes toward needle stick injuries, preventive measures and application on their practical training was poor. |
| Muralidhar et al. [30] | 428 HCWs of various categories | Quantitative | Issues requiring attention include disposal of sharps, establishing a staff/student health service and inculcating responsible attitude among HCWs. |
| Gurubacharya et al. [32] | Nurses and paramedical staffs from Kathmandu Hospital | Quantitative | Attitude and Knowledge of HCWs about the risk associated with needle stick injuries and implementation of preventive measures were inadequate. |
| Hashmi et al. [18] | 750 HCWs of Maternity and Children’s Hospital | Quantitative | 64.5% of injuries occurred during the use of device shows negative attitude of HCWs. |
Prior literatures on staff attitudes for Healthcare Workers (HCWs)
3.4. Precautionary Measures
According to Fashafsheh et al. [20], if the data on injuries of needle and sharps in hospitals is assessed to determine the distribution of HCWs disease burden; the category is distributed by ward or by activity, and it would allow prevention methods to be more specifically targeted (Table 4). As such, ideal precautionary measures should be developed and melded to capture the unique realities of a specific healthcare facility. Khraisat et al. [21] developed an evidence-based module to guide practicing nurses on needle stick safety and prevention. Literature explored several practical approaches to create a safe culture at workplace, during which the process they identified the primary causes of serious injuries as illustrated in Figure 1.
| Authors | Sample | Methodology | Findings |
|---|---|---|---|
| Siddique et al. [19] | 14 geographical regions | Quantitative | Occupational exposures to percutaneous injuries are significant source of infections among HCW. |
| Amoran et al. [33] | 421 HCWs in Nigeria | Quantitative | Institution of a surveillance system for hospital acquired infection to improve consistent use of standard precautions among HCW is recommended in Nigeria and other low income countries in Africa. |
| Al-Ghamdi et al. [22] | KSA during Hajj season | Quantitative | The HCWs have difficulties in some precautionary measures, especially among those with less years of experience, and those who did not read the written guidelines, which highlights the importance of training before Hajj season. |
Prior literatures on precautionary measures for Healthcare Workers (HCWs)
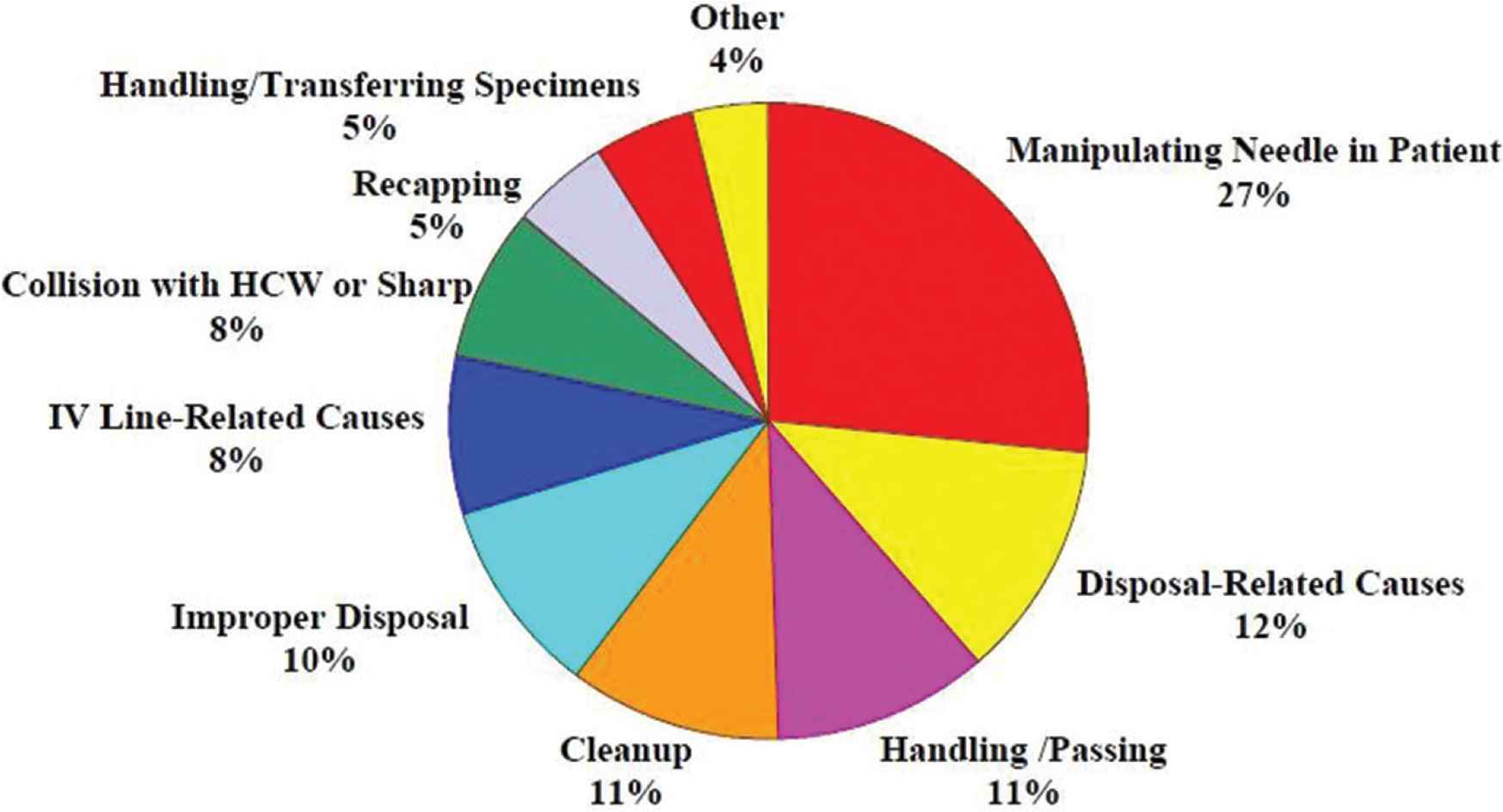
Causes of percutaneous injuries with hollow-bore needles in CDC surveillance hospitals [16].
A study was conducted by Al-Ghamdi and Kabbash [22] in Saudi Arabia hospitals during Hajj season and figured out that it is difficult to maintain the precautionary measures because HCWs had less experience and no proper precautions’ guidelines. Derivatively, therefore, Nawafleh et al. [15] recommended that these causes define the precautionary measures that HCWs (particularly practicing nurses) should adopt to prevent needles and sharps injuries. The scholars proposed the Hierarchy of Controls that can help prevent and adequately respond to such injuries, incorporating five distinct levels of control from the most effective to the least effective, namely:
- •
Elimination of hazards: Through substituting unnecessary injections with alternatives such as administering the medications through inhalers, tablets, and patches, or by eliminating the use of needles and sharps with patients during intervention.
- •
Engineering controls: Using strategic devices and needles that are effective and ideal for accuracy by design, such as retract needles, sheathed instruments and blunt devices.
- •
Administrative controls: Creating, implementing and enforcing policies that limit the exposure to hazards, proper allocation of resources, observing the safety of healthcare workers, instituting a needle stick prevention committee, having an operational exposure control plan, and supporting, facilitating and mandating consistent training and awareness.
- •
Work practice controls: Adopting proper and appropriate working protocols such as avoiding re-capping, adopting ideal disposal protocols, placing the needles and sharp containers at an arm-reach and eye-level locations, mandating strategic safe handling of all clinical devices, etc.
- •
Personal protective equipment control: Ensuring that workers are supplied with adequate equipment to act as preventatives, barriers, and filters of injuries such as gowns, eye goggles, gloves, face shields, and masks.
3.5. Compliance of Needle Stick and Sharps Injury Safety
In their WHO-funded study, Prüss‐Üstün et al. [14] likened the hazards of needle and sharps injuries to an increasing and nearly catastrophic disease burden among HCWs globally, specifically highlighting diseases as HBV, HCV, and HIV. As mentioned above, according to Shiao et al. [23], not only is a needle stick injury characterized by the trauma itself, but also by the percutaneous exposure to a patient’s blood and body fluids, which may communicate infectious diseases (Table 5). Consequently, Makary et al. [24] among many other scholars identify ill health, acute and chronic diseases infection, and probability of death (fatality) as the most predictable hazards that accrue from needle stick and sharps injuries. Also, it argued that based on the clinical severity, health complications and fatality of needle stick and sharps injuries among HCWs are the most debilitating diseases. The blood-borne pathogens are HBV, HCV and HIV, where HBV, HCV and HIV, Hepatitis B, Hepatitis C and HIV/Aids virus. The foregoing findings concur with the findings published by WHO and Azadi et al. [25]. According to Prüss‐Üstün et al. [14], sharps injuries among HCWs have reached to 1000 HIV, 16,000 Hepatitis C, and 66,000 Hepatitis B. Among HCWs, with a rate of HCV (39%), HBV (37%), and HIV (4.4%). It is important to note that needle stick and sharps injuries trigger hazards which threaten the safety of HCWs, ranging from infections to fatal consequences [26]. Such hazards have been confirmed globally. At the start of the last decade, Poznansky et al. [27] conducted an empirical study to characterize the risk of blood-borne pathogens to HCWs after needle stick injuries in Taiwan. In their research study, authors highlighted the hazards that result from the transmission of blood-borne pathogens after needle stick injuries. Given this hazard, researchers advocated for a new strategic measure to reduce HIV infections among healthcare providers across Britain [27]. According to the Commission, aspects of the Law Relating to AIDS [12], after an empirical survey of the highest HIV preference in Africa at that time, the commission advocated that the country should review its legal framework to address the rising risk of AIDS infections among healthcare service providers. To the commission, the effects of needle stick and sharps injuries in South Africa were triggering HIV infections hazards among HCWs. In Germany similar findings were reported by Wicker et al. [28] about needle stick injuries among HCWs in university hospital, Wicker et al. [28] confirmed that blood-borne pathogens that trigger Hepatitis B, Hepatitis C and HIV infections were the main hazards of needle stick and sharps injuries alongside stab, scratch, cut, or other bloody injuries. Like many other developed states, Germany is facing the needle stick and sharps injury hazards with an increasing cause for concern as the rate became even more critical, as established previously.
| Authors | Sample | Methodology | Findings |
|---|---|---|---|
| Rampal et al. [31] | 287 | Quantitative | The overall prevalence of needle stick injuries was 23.5%. Nurses had the highest prevalence (27.9%). The causes of infection in 58% of cases were hypodermic needle and 27.2% cases were recapping. Medical ward reported the highest infection rate (51.9%). |
| Swe et al. [12] | 316 medical students | Cross-sectional study | Study states that noncompliance or failure to adhere to guidelines can become critical determinate of needle stick injuries. |
| Ng et al. [34] | 136 Malaysian HCW | Quantitative | HCWs are at risk of needle stick injury while performing procedures on patients. Therefore compliance control strategies are not applied effectively to reduce the risk of infection. |
| Azadi et al. [25] | 434 dentists | Quantitative | High rate of infection and low rate of compliance. |
Prior literature on compliance of infection
This narrative review has several limitations which may impact on the findings generalizability. The review reported mainly observational cross-sectional studies of assessment of HCWs knowledge and attitudes toward infection control practice. Additionally, this review is prone to social desirability bias which could lead to over/underestimation of the study findings. Compliance to infection control measures must be a top priority in healthcare. HCWs should have high degree of knowledge and compliance to hand hygiene to minimize the spread of infection. Staff’s continuing education and training are essential to improve HCWs infection knowledge and prevention practices. Future researches should consider stronger interventional and non-interventional designs to report healthcare providers’ knowledge and attitudes toward infection control and the actual prevalence of needle stick injuries and hospital acquired infection as a result of poor infection prevention.
4. CONCLUSION
This review intended to discuss literature on infection control knowledge and attitudes among HCWs and potential factors contributing to infection control. It has also discussed the precautionary measures and compliance with infection control precautions among HCWs. The current study has found significant correlation between staff attitude and precautionary measures, where precautionary measures were found to influence staff compliance with needle safety precautions. The level of knowledge showed significant differences for the interaction of HCWs’ based on the existing findings of staff knowledge, attitude, precautionary measures and compliance with needle safety. It is highly suggested that engineering and eliminating or substituting controls will be very sufficiently effective in infection control and prevention.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
A. AlJohani contributed in conception, proposal, data collection and analysis, and manuscript preparation. KK contributed in manuscript preparation. A. Al Mutairi contributed in data collection and analysis and manuscript preparation. A. Al Mutair contributed in conception, and manuscript preparation.
ACKNOWLEDGMENT
This research was supported financially by
REFERENCES
Cite this article
TY - JOUR AU - Abdurahman AlJohani AU - Karmegam Karuppiah AU - Alya Al Mutairi AU - Abbas Al Mutair PY - 2020 DA - 2020/11/09 TI - Narrative Review of Infection Control Knowledge and Attitude among Healthcare Workers JO - Journal of Epidemiology and Global Health SP - 20 EP - 25 VL - 11 IS - 1 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.201101.001 DO - 10.2991/jegh.k.201101.001 ID - AlJohani2020 ER -