
Primary Bone Tumors in North of Jordan
 , Rami A. Jahmani1, Abedallah Al Khateeb1, Faisal Nimri2, , Mohammad A. Al-Ebbini3, Abdel Rhaman M. Ababneh3,
, Rami A. Jahmani1, Abedallah Al Khateeb1, Faisal Nimri2, , Mohammad A. Al-Ebbini3, Abdel Rhaman M. Ababneh3, - DOI
- 10.2991/jegh.k.201102.001How to use a DOI?
- Keywords
- Bone tumor; multiple myeloma; osteochondroma; giant cell tumor
- Abstract
Objective: Primary tumors of bone are relatively uncommon. Little information is available about the etiology, pathophysiology, risk factors and epidemiologic features of bone tumors. In this article, we present the epidemiological data about the primary (benign and malignant) bone tumors in Jordan.
Methods: Retrospectively, we identified and assessed those patients who were diagnosed with primary bone tumor between January 2004 and December 2018 at King Abdullah University Hospital. The following information was obtained: demographics (age, sex), clinical presentation, and location of the tumor. Also, the histopathological results and finding and recurrence of the tumors were retrieved. The included primary bone tumors were those tumors fulfill the World Health Organization classification of soft tissue and bone tumors.
Results: During the study period, four-hundred and thirty-seven cases of the primary bone tumor were diagnosed in our institution. More than half of the cases were males (52.5% males and 47.5% females). In most cases, young adults are affected. The mean age for the diagnosis of giant cell tumor of bone (GCTB) is 34.1 years. The appendicular skeleton was involved in 269 (81.5%) patients while the axial skeleton in 60 patients. The most common encountered pathology is the multiple myeloma with 120 patients. After that, osteochondroma was diagnosed in 110 patients. Females were mostly affected by giant cell tumor while the osteochondroma and chondrosarcoma were seen mostly in males. Multiple myeloma tends to develop in elderly while juvenile ossifying fibroma occurred in young pediatrics and Ewing sarcoma in school-age children and adolescents. Giant cell tumor and osteoid osteoma have the tendency to recur.
Conclusion: The diagnosis of primary bone tumors is of particular important. The reporting of epidemiological studies is essential in order to expand our knowledge regarding this uncommon type of tumors.
- Copyright
- © 2020 The Authors. Published by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
According to the World Health Organization (WHO) classification of soft tissue and bone tumor, the primary bone tumors are classified based on the origin cell of the tumor as cartilaginous tumors, osteogenic tumors, fibrogenic tumors, hematopoietic tumors, and many others [1]. Among the wide array of human neoplasms, primary tumors of bone are relatively uncommon [1,2]. Not only has this contributed to the paucity of meaningful and useful data about the relative frequency and incidence rates of the various subtypes of bone tumors, but it also explains our rudimentary understanding of risk factors.
Little information is available concerning the etiology and epidemiologic features of benign bone tumors since most published statistical studies have dealt with bone sarcomas. The benign lesions will be considered from the epidemiologic and aetiologic standpoint under the individual chapter headings, where they are known [2,3]. In this article, we present and discuss our epidemiological and diagnostic data about the primary (benign and malignant) bone tumors in Jordan.
2. MATERIALS AND METHODS
This study was conducted at King Abdullah University Hospital, a tertiary care center that is affiliated with the Jordan University of Science and Technology, located in Northern Jordan. It is the sole center for pathological diagnosis in Northern Jordan. After obtaining the Institutional Review Board approval, we retrospectively identified and assessed those patients who were diagnosed with primary bone tumor between January 2004 and December 2018. The following information was obtained: demographics (age, sex), clinical presentation, and location of the tumor. Also, the histopathological results and finding and recurrence of the tumors were retrieved.
The primary bone tumors were diagnosed according to the WHO classification of soft tissue and bone tumors.
Data were collected and entered into a spreadsheet and analyzed using appropriate software. Categorical variables were described using the frequency distribution, while continuous variables were described using the mean ± standard error of the mean.
3. RESULTS
During the study period, four-hundred and thirty-seven cases of the primary bone tumor were diagnosed in our institution. Generally, males were affected more than females (52.5% males and 47.5% females). Mostly, young adults are affected. The mean age for the diagnosis of GCTB is 34.1 years and the median are 26 years. The youngest patient was 1 year and the oldest was 90 years. The appendicular skeleton was involved in 269 (81.5%) patients while the axial skeleton in 60 patients and one patient presented with multiple involvements. The left side of the appendicular skeleton was affected in 116 patients while the right in 100 patients. The most common encountered pathology is the multiple myeloma with 120 patients. After that, osteochondroma was diagnosed in 110 patients. Also, malignant osteosarcoma, chondroblastoma, chondrosarcoma, Ewing sarcoma, fibrosarcoma, and rhabdomyosarcoma were diagnosed in 33, 6, 14, 22, 1, and 1; respectively. The most common presenting symptoms were swelling and pain. The constitutional symptoms as anemia and fatigue were dominant in multiple myeloma cases. Table 1 summarizes the general sample characteristics.
| Bone tumor characteristics | Number | Valid percent (%) |
|---|---|---|
| Mean ± SE | ||
| Sex | ||
| Male | 229 | 52.5 |
| Female | 207 | 47.5 |
| Age at diagnosis (years) | 34.1 ± 1.1 | |
| Clinical presentation | ||
| Pain | 122 | 36.2 |
| Swelling | 146 | 43.3 |
| Incidentally | 4 | 1.2 |
| Neurological deficit | 4 | 1.2 |
| Constitutional symptoms | 46 | 13.6 |
| Deformity | 5 | 1.5 |
| Diastematomyelia | 1 | 0.3 |
| Pathological fracture | 8 | 2.4 |
| Skin rash | 1 | 0.3 |
| Location (Axial or appendicular skeleton) | ||
| Axial | 60 | 18.2 |
| Appendicular | 269 | 81.5 |
| Multiple sites | 1 | 0.3 |
| Location (Upper or lower limb or axial skeleton) | ||
| Upper limb | 66 | 20.0 |
| Lower limb | 203 | 46.5 |
| Axial skeleton | 60 | 18.2 |
| Multiple sites | 1 | 0.3 |
| Site (if the tumor was in the appendicular skeleton) | ||
| Right | 100 | 45.7 |
| Left | 116 | 53.0 |
| Bilateral | 2 | 0.9 |
| Multiple sites | 1 | 0.5 |
| Pathological diagnosis | ||
| Chondroblastoma | 6 | 1.4 |
| Enchondroma | 32 | 7.3 |
| Chondrosarcoma | 14 | 3.2 |
| Ewing sarcoma/PNET | 22 | 5.0 |
| Fibrous dysplasia | 22 | 5.0 |
| Giant cell tumor | 25 | 5.7 |
| Multiple myeloma | 120 | 27.5 |
| Osteochondroma | 110 | 25.2 |
| Osteoid osteoma | 26 | 5.9 |
| Osteosarcoma | 33 | 7.6 |
| Osteofibrous dysplasia | 3 | 0.7 |
| Fibrosarcoma | 1 | 0.2 |
| Cavernous hemangioma | 2 | 0.5 |
| Non-ossifying fibroma | 8 | 1.8 |
| Juvenile ossifying fibroma | 3 | 0.7 |
| Chondromyxoid fibroma | 1 | 0.2 |
| Odontogenic fibromyxoma | 1 | 0.2 |
| Multiple hereditary exostosis | 1 | 0.2 |
| Rhabdomyosarcoma | 1 | 0.2 |
| Synovial osteochondromatosis | 3 | 0.7 |
| Unclassified sarcoma | 3 | 0.7 |
| Recurrence | 15 | 4.1 |
| Time to recurrence (years) | 4.0 ± 1.1 | |
General sample characteristics
Regarding the distribution of sex within different categories, the ratio of male:female is generally equal in most types of tumor. However, females were mostly affected by giant cell tumor while the osteochondroma and chondrosarcoma were seen mostly in males. Figure 1 summarizes the distribution of sex. The mean age for most tumors was below 40. However, multiple myeloma tends to develop in the elderly after 60s as indicated by Figure 2. On the other hand, juvenile ossifying fibroma occurred in young pediatrics and Ewing sarcoma in school-age children and adolescents.
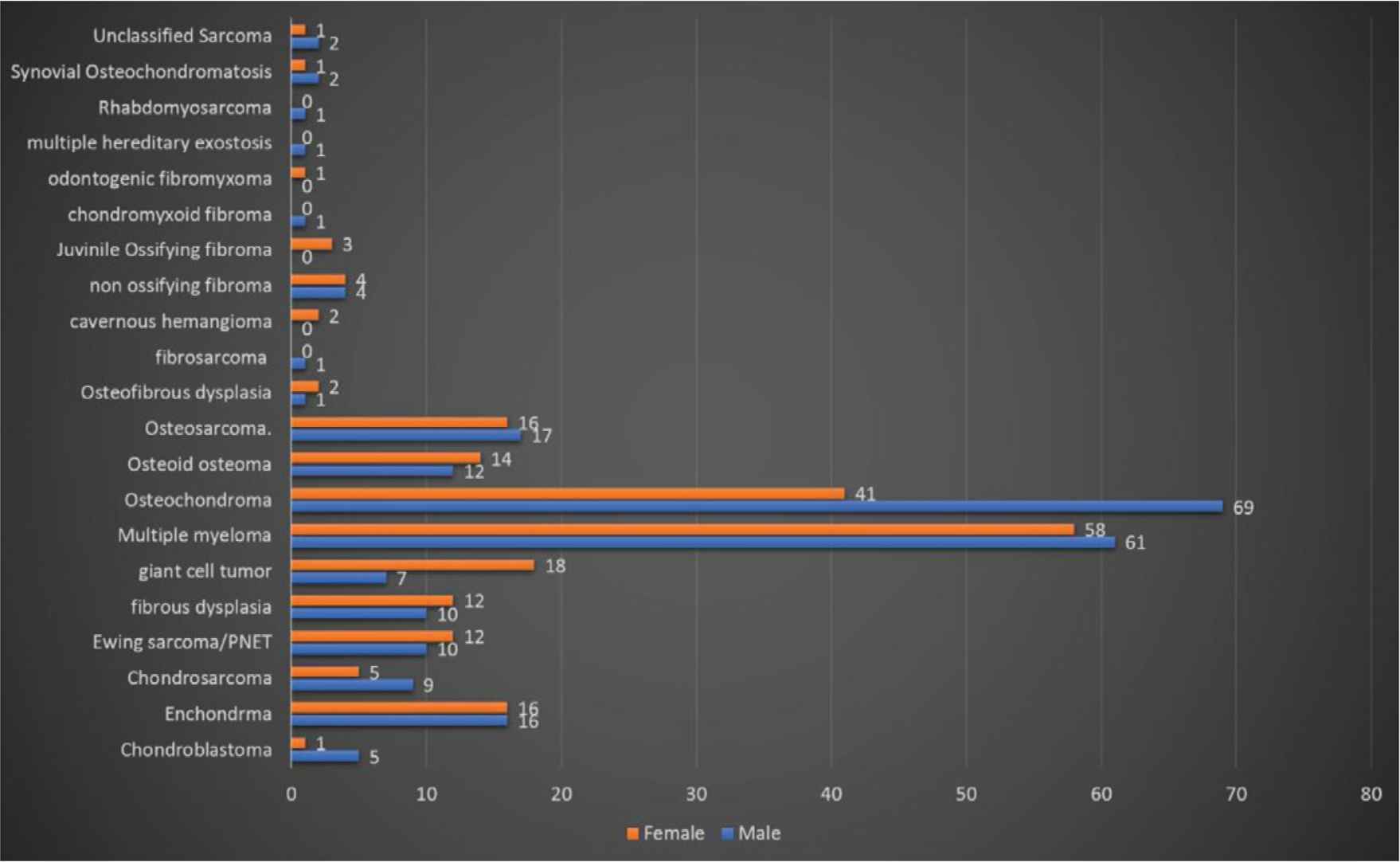
The distribution of sex within different pathologies.
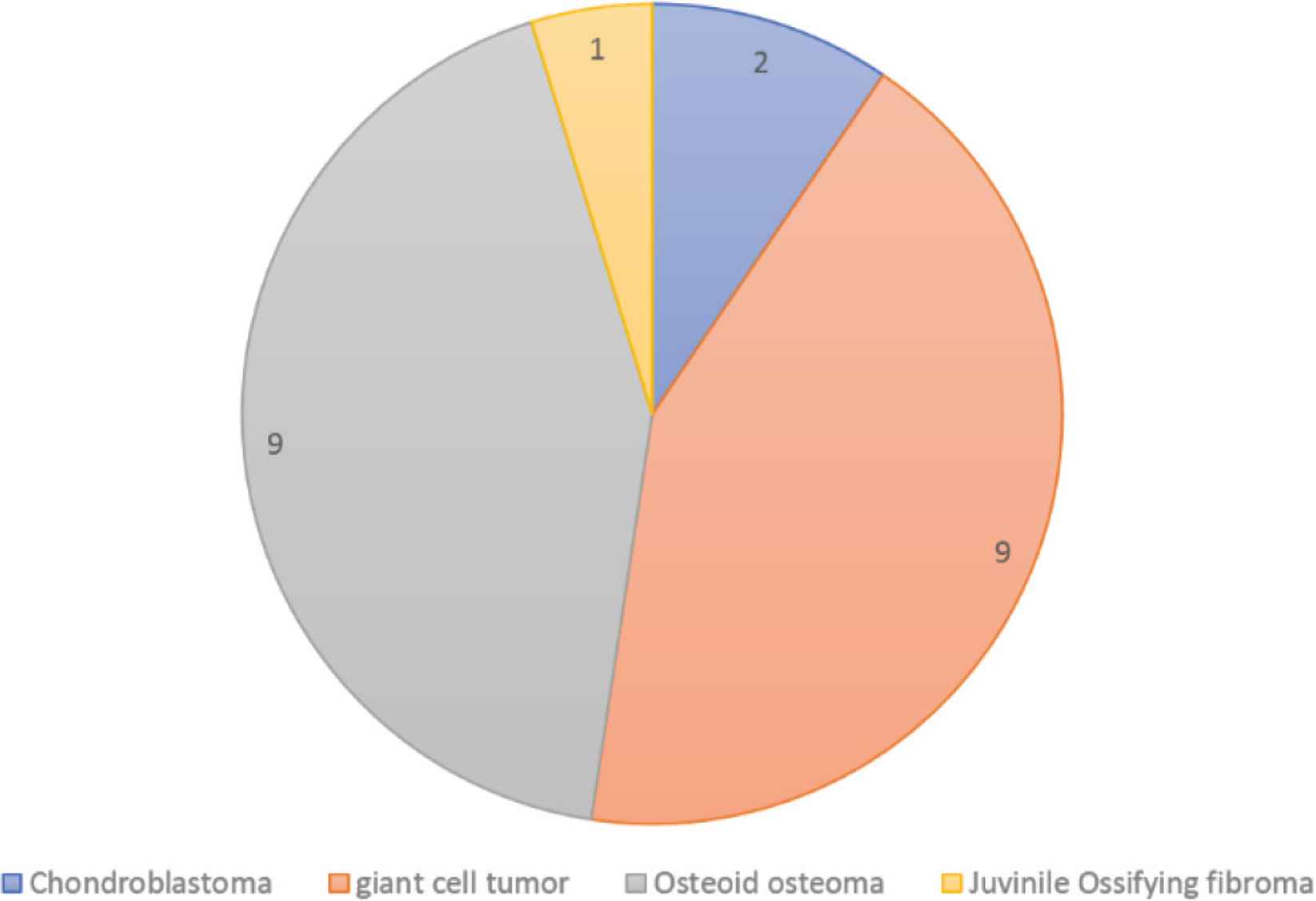
Number of recurrences.
Table 2 summarizes the location distribution of each tumor. Enchondroma had a tendency to develop in the upper limb bones. The chondrosarcoma developed in the axial and lower limb along with the Ewing sarcoma. In contrast, multiple myeloma developed mostly in the axial skeleton. The osteochondroma and osteosarcoma had an exclusive tendency for the lower limb bones.
| Diagnosis | Upper limb (% from the diagnosis) | Lower limb (% from the diagnosis) | Axial (% from the diagnosis) | Multiple (% from the diagnosis) |
|---|---|---|---|---|
| Chondroblastoma | 1 (16.7) | 5 (83.3) | 0 (0.0) | 0 |
| Enchondroma | 22 (71.0) | 9 (29.0) | 0 | 0 |
| Chondrosarcoma | 0 | 7 (58.3) | 5 (41.7) | 0 |
| Ewing sarcoma/PNET | 1 (4.5) | 13 (59.1) | 8 (36.4) | 0 |
| Fibrous dysplasia | 3 (14.3) | 14 (66.7) | 4 (19.0) | 0 |
| Giant cell tumor | 5 (20.0) | 15 (60.0) | 5 (20.0) | 0 |
| Multiple myeloma | 0 | 5 (26.3) | 14 (73.7) | 0 |
| Osteochondroma | 20 (18.2) | 84 (76.4) | 5 (4.5) | 1 (0.9) |
| Osteoid osteoma | 9 (34.6) | 10 (38.5) | 7 (26.9) | 0 |
| Osteosarcoma | 1 (3.1) | 28 (87.5) | 3 (9.4) | 0 |
| Osteofibrous dysplasia | 0 | 0 | 3 (100.0) | 0 |
| Fibrosarcoma | 0 | 0 | 1 (100.0) | 0 |
| Cavernous hemangioma | 0 | 0 | 1 (100.0) | 0 |
| Non-ossifying fibroma | 2 (25.0) | 6 (75.0) | 0 | 0 |
| Juvenile Ossifying fibroma | 0 | 0 | 3 (100.0) | 0 |
| Chondromyxoid fibroma | 1 (100.0) | 0 | 0 | 0 |
| Odontogenic fibromyxoma | 0 | 0 | 1 (100.0) | 0 |
| Multiple hereditary exostosis | 0 | 1 (100.0) | 0 | 0 |
| Rhabdomyosarcoma | 1 (100.0) | 0 | 0 | 0 |
| Synovial osteochondromatosis | 0 | 3 (100.0) | 0 | 0 |
| Unclassified sarcoma | 0 | 3 (100.0) | 0 | 0 |
Comparison of different types of bone tumor in term of location
Twenty-one cases of recurrence were found after complete remission of the tumor. The mean time for recurrence was 4 years after the diagnosis of the primary tumor. Figure 3 indicates the distribution of recurrences cases. Osteoid osteoma and giant cell tumors were the most common tumors to recur after the treatment.
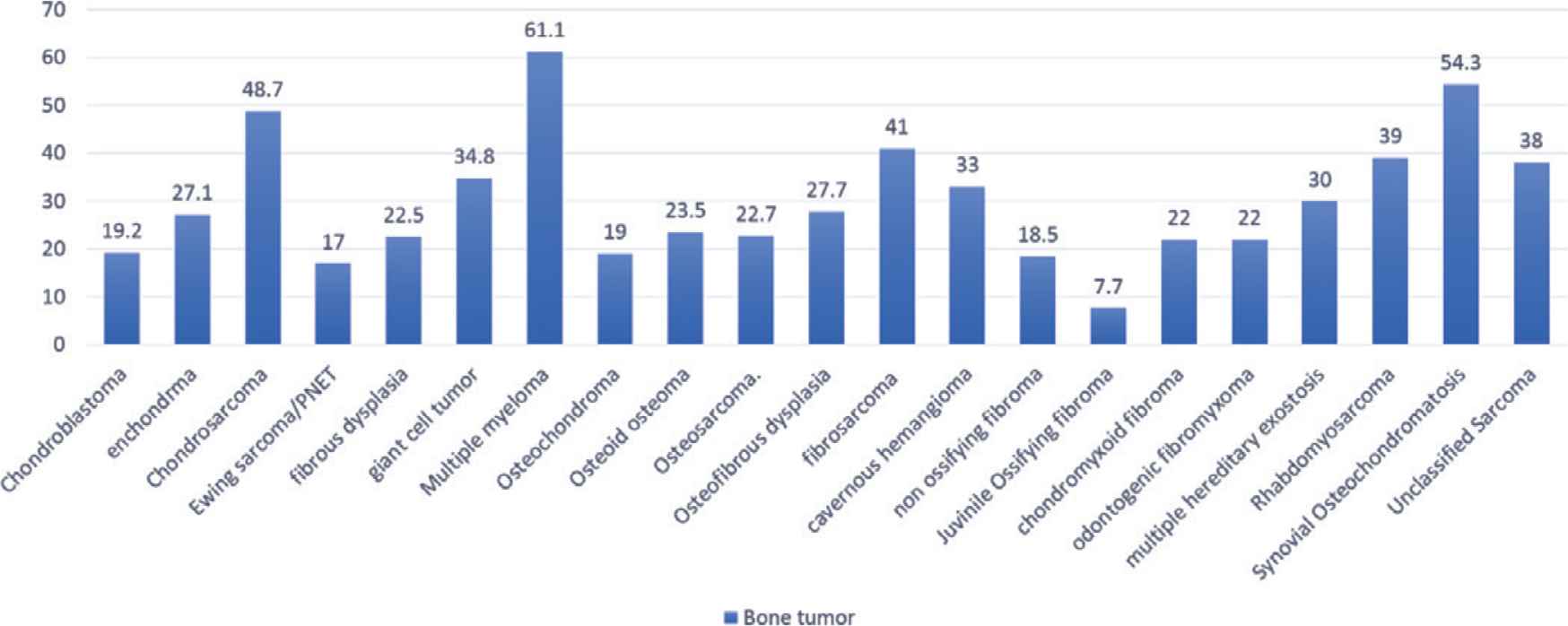
The mean age for each tumor.
4. DISCUSSION
This article is a recent epidemiological study about the primary bone tumor diagnosed at King Abdullah University Hospital in Northern Jordan over 14 years and represents the population of about 2.8 million residing in this area. An old study from 1998 studied the Demographic analysis of Primary bone Tumors of Jordan University Hospital and showed almost the same epidemiological Trend with some variation representing the increasing number of population and improved the health care quality and diagnostic modalities in Jordan. According to the WHO classification of soft tissue and bone tumors, primary bone tumors are uncommon if compared with other types of tumors that affect the human. Primary bone tumors are classified based on the origin cell of the tumor as cartilaginous tumors, osteogenic tumors, fibrogenic tumors, hematopoietic tumors, and many others. Bone sarcoma constitutes only 0.2% of all tumors [1].
The most common subtype of primary malignant bone tumors is osteosarcoma, which constitute around 35% of all cases, followed by chondrosarcoma and then Ewing sarcoma, which make 25% and 16% respectively [1–4]. In our study, osteosarcoma constitute 7.6% of all primary bone tumors followed by Ewing sarcoma with 5% and osteochondroma with 3.2%, this make Ewing sarcoma the second most common malignant tumor and chondrosarcoma the third one, so our study showed different results than the above-mentioned distribution. These results are consistent with Rao et al. [5] in India and with Shah et al. [6] results. On the other hand, the results in western countries are different than our distribution in which the osteochondroma is more common than Ewing sarcoma [7,8]. Osteosarcoma occurred in males (51.51%) more than females (48.48%). Besides, it had more appendicular (90.6%) than axial (9.4%) involvement, and there were more cases with lower limbs (87.5%) involvement compared to upper limbs (3.1%). The mean age of diagnosis is 34.1 years. According to a study about osteosarcoma in US, males were more affected than females at all age groups and all ages [9]. Also, appendicular skeleton was involved more than axial skeleton with an obvious preference for lower limbs (74.5%) in comparison with upper limbs (11%). The incidence peaks in males at the ages of 16 and 79, whereas the peak incidence in females was at the age of 12 and 77 [9].
The incidence of primary benign bone tumors is likely underestimated because benign lesions are usually asymptomatic. Nevertheless, they are much more common than primary malignant tumors [2–4]. According to our data, osteochondroma occurred in men (62.72%) more than women (37.27%), and it has more appendicular (94.6%) than axial (4.5%) involvement. Also, there was more cases with lower limbs (76.4%) involvement compared to upper limbs (18.2%). The mean age of diagnosis is 34.1 years. A study conducted in South China showed similar results [10]. In that study, more males (67.51%) were affected. 250 cases out of 431 had knee involvement. The mean age of diagnosis was 20.63 years [10].
The frequency of bone tumors concerning age shows a bimodal distribution, with the first peak being at the second decade. While the second peak does not occur until the sixth decade [1]. Osteosarcoma occurs predominantly in patients younger than age 20, and in this group 80% occur in long bones of the extremities [11–15]. Different types of tumors have different preferences regarding the distribution. For example, although Ewing sarcoma and osteosarcoma have similar epidemiological features, osteosarcoma occurs at the metaphysis of long bones, whereas Ewing sarcoma usually arise at the diaphysis [16–19]. Besides, age affects the primary location of bone tumors. For example, axial primary lesions were reported to be more frequent in older than in younger patients [11–19]. In the United States and Europe, giant cell tumor accounts for approximately 5% of all primary bone tumors and 21% of all benign bone tumors [20]. In China, GCTB represents 20% of all primary bone tumors [21]. GCTB occur most commonly in females in the third decade of life, between the age of 20 and 40.3 [20]. Giant cell tumor typically affects the ends of long bones, especially the distal femur, proximal tibia and fibula, and distal radius [22]. In Jordan, a study was conducted about GCTB and they found that GCTB is more common in females. Most common location is the epiphyseal/metaphyseal area around the knee. Multicentric GCTB and pulmonary metastasis were more common. Most patients were treated with intralesional curettage with or without adjuvant. Recurrence rate is 45%. Most patients showed late recurrence. Complex anatomical locations, younger age, male gender, and Campanacci grade III tumors were associated with high risk of recurrence. Some patients showed resolution of pulmonary nodules during follow-up. Denosumab was used for patients with multicentric tumors, pulmonary nodules, and recurrence. Late malignant transformation was detected in one patient with fatal outcome which warrants prolonged follow-up of GCTB [23].
Multiple myeloma is a plasma-cell disorder that is characterized by clonal proliferation of post-germinal-center B cells (malignant plasma cells) in bone marrow with the presence of monoclonal protein in the blood or urine and is accompanied with end organ dysfunction [24,25]. According to the WHO classification of soft tissue and bone tumors, multiple myeloma is considered one of the primary bone tumors [1]. To be diagnosed, multiple myeloma requires the presence of at least 10% of clonal bone marrow plasma cells, in association with the presence of monoclonal protein in blood or urine [24]. If the presence of plasmacytoma is confirmed by biopsy, the diagnosis of non-secretory myeloma can be made [26]. If symptomatic, multiple myeloma often presents with hypercalcemia, renal insufficiency, anemia, and bone disease (such as pathological fractures) [26–28]. Immediate management depends on the presence of symptoms, because studies revealed that early treatment without symptoms has no benefits [29,30].
5. CONCLUSION
Our study revealed that primary bone tumors are more common in males than females. Also, there was a significant difference between the axial and appendicular skeleton, as more tumors originated from appendicular skeleton. To be more specific, tumors originated from the lower limbs more than the upper. Furthermore, left sided tumors were more frequent than right ones. The most common complaint was feeling of a mass, that was painful in most of the cases. The most frequent histological diagnosis was multiple myeloma followed by osteochondroma.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
All authors contributed significantly and in agreement with the content of the article. All authors were involved in project design, data collection, analysis, statistical analysis, data interpretation and writing the manuscript. All authors presented substantial contributions to the article and participated of correction and final approval of the version to be submitted.
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
ETHICAL STATEMENT
This study was approved by the Institutional Review Board at the Jordan University of Science and Technology and Kind Abdulla University Hospital.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Khaldoon M. Bashaireh AU - Mohammed Alorjani AU - Rami A. Jahmani AU - Abedallah Al Khateeb AU - Faisal Nimri AU - Mohammad A. Al-Ebbini AU - Abdel Rhaman M. Ababneh PY - 2020 DA - 2020/11/11 TI - Primary Bone Tumors in North of Jordan JO - Journal of Epidemiology and Global Health SP - 132 EP - 136 VL - 11 IS - 1 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.201102.001 DO - 10.2991/jegh.k.201102.001 ID - Bashaireh2020 ER -