
Assessment of Knowledge, Perceptions and Perceived Risk Concerning COVID-19 in Pakistan
 , Rafia Mumtaz3, , Farheen Masood4, Hudebia Allah Buksh5, , Amal Ahmed6, Osama Khattak7
, Rafia Mumtaz3, , Farheen Masood4, Hudebia Allah Buksh5, , Amal Ahmed6, Osama Khattak7- DOI
- 10.2991/jegh.k.210109.001How to use a DOI?
- Keywords
- COVID-19; perceptions; knowledge; coronavirus; risk assessment; myths; pandemic
- Abstract
The COVID-19 pandemic is one of unmatched scale and severity. A continued state of crisis has been met with poor public adherence to preventive measures and difficulty implementing public health policy. This study aims to identify and evaluate the factors underlying such a response. Thus, it assesses the knowledge, perceived risk, and trust in the sources of information in relation to the novel coronavirus disease at the outset of the COVID-19 pandemic. An online questionnaire was completed between March 20 and 27, 2020. Knowledge, perceptions, and perceived risk (Likert scale) were assessed for 737 literate participants of a representative sample in an urban setting. We found that respondents’ risk perception for novel coronavirus disease was high. The perceived risk score for both cognitive and affective domains was raised at 2.24 ± 1.3 (eight items) and 3.01 ± 1 (seven items) respectively. Misconceptions and gaps in knowledge regarding COVID-19 were noted. Religious leadership was the least trusted (10%) while health authorities were the most trusted (35%) sources of information. Our findings suggest that there was a deficiency in knowledge and high concern about the pandemic, leading to a higher risk perception, especially in the affective domain. Thus, we recommend comprehensive education programs, planned intensive risk communication, and a concerted effort by all stakeholders to mitigate the spread of disease. The first of its kind in the region, this study will be critical to response efforts against current and future outbreaks.
- Copyright
- © 2021 The Authors. Published by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
The rapid spread of COVID-19 has given rise to a global public health emergency. As cases continue to emerge, the World Health Organization (WHO) has raised the level of this outbreak to a pandemic [1]. After the first announced case of the disease in Wuhan, China, it has affected over 20 million people and 181 countries worldwide [2]. In Pakistan, an outbreak was declared on February 26 and as of April 2, 2020, the number of cases increased to over 2000 [3].
Efforts to contain the virus have resulted in social, political, and economic instability in the world over. Developing countries like Pakistan face the greatest challenges. There, poor healthcare infrastructure, porous borders, and domestic trade policies pose a significant problem [4]. To limit the proliferation of COVID-19, the government has implemented national emergency programs and mass awareness campaigns [5].
In the absence of any definitive treatment or vaccine, the success of these initiatives is inextricably linked to public action. The extent and efficacy of this is linked to citizens’ knowledge and risk perception in relation to COVID-19 [6,7]. Indeed, previous epidemics underscore the value of these factors in limiting the spread of disease [8]. However, COVID-19 is not an epidemic, but a pandemic with no precedent. Thus, the public response to it is bound to be unique, particularly in the developing world.
As our understanding of and attitude towards novel coronavirus evolves, it is subject to conflicting coverage by the media. New guidelines for prevention continue to emerge, as do ambiguities about transmission and contesting claims about potential treatment options. Misinformation and disinformation on social media are an additional source of confusion. It is no surprise that citizens increasingly refuse to adhere to preventative measures or advice [9]. Given the discernible correlation between non-compliance and transmission, this raises questions about their awareness of the novel coronavirus. Under these circumstances, assessing the extent of public understanding about COVID-19 is critical. Indeed, there is evidence that public knowledge plays a critical role in the observation of preventive measures. Information about public perception, on the basis of this, can be instrumental to the formulation of effective policies to curb current and future health disasters [10].
Among other factors influencing people’s conformity to infection control policies is threat appraisal, which can be modulated by knowledge, emotions and trust in information sources [11,12]. This forms a vital component of counter response to COVID-19 globally. Yet, available research models of risk perceptions are predominantly based on populations in the developed world [13]. Accounting for poverty, political instability, and food insecurity, an insight into the perceptions of those from developing countries like Pakistan could be invaluable in developing these models further. This has also been acknowledged by a WHO report on risk [14]. Furthermore, most studies have explored a single dimension of risk, being cognitive or affective, when considering both elements could be much more informative [15]. Exploring multiple risk dimensions and associated factors like knowledge and trust can enable the development of better informed and effective counter strategies against the current crisis [6,15,16]. It could also provide us with an opportunity to prepare for any such future threat, particularly as pandemics are predicted to occur more frequently in the decades to come [17].
To this end, we undertook this study to investigate COVID-19 related knowledge, risk perception, and trust in information sources, among the urban, educated adult population of Pakistan. This was evaluated with the aim of identifying factors which could contribute to coronavirus-related mortality and morbidity. These findings could be instrumental to the modelling and implementation of public health policy in the developing world.
2. MATERIALS AND METHODS
2.1. Study Design and Settings
A descriptive cross-sectional survey was conducted for the period of 1 week from 20th to 27th of March 2020, in the cities of Islamabad, Peshawar, Lahore and Karachi. These are four of the most populated, with comparatively higher literacy rates [18].
2.2. Participants
Authors relied on their contacts residing in different provinces of Pakistan. The questionnaire was posted on social media platforms. Those who were willing to participate in the study, able to read and speak English, and aged at least 18 years were selected using random convenience sampling. Participants were informed about the study with an invitation to fill the attached questionnaire.
2.3. Study Instrument
For survey development, an instrument from a previous study was reviewed [19]. A pilot study was conducted on a small sample of 35 participants to determine the suitability of the instrument for the Pakistani public in terms of length and logic. Based on feedback, the questionnaire was shortened and subsequently distributed using an electronic platform through Google documents via a unique URL [20]. The Cronbach’s alpha coefficient for the questionnaire was more than 0.7 for all sections assessing knowledge as well as cognitive and risk perceptions.
Demographic information was collected on gender, age, education and ethnicity. Multiple choice options and trichotomous responses were used to evaluate participants’ understanding of the pandemic (yes/no/don’t know).
In the first section, respondents were asked to rate their knowledge of COVID-19. They were to identify correct definitions, symptoms, routes of transmission, probability of death and effective/ineffective preventive measures.
The second section addressed risk perception and fear. Cognitive and affective dimensions of risk assessment were investigated using a 5-point Likert scale. Response options were strongly disagree/disagree (scored as 1), neutral (scored as 2) and strongly agree/agree (scored as 3). To simplify analysis, categories of strongly agree and agree were merged as were strongly disagree and disagree [21]. Cognitive assessment comprised eight questions, requiring participants to estimate the probability of them contracting the virus and rate the likelihood of the virus causing harm to them and their families. The affective domain was explored in the second part, with 6 questions focusing on concerns regarding COVID-19.
The last section assessed trust in politics, authorities, and sources of information to gauge public leadership preferences during this crisis.
2.4. Ethical Approval
The study was ethically approved by the Institutional Review Board, HITEC-Institute of Medical Sciences, Taxila. Furthermore, the participation of respondents was voluntary, and a high level of confidentiality and anonymity was maintained during the study. Research was carried out in accordance with the Ethical Principles for Medical Research Involving Human Subjects of the (Declaration of Helsinki) World Medical Association.
2.5. Data and Analysis
Online study data was transferred to an excel spreadsheet and descriptive analysis was used to express results in the form of percentages and frequencies. Descriptive analyses were performed to report percentages and frequencies.
3. RESULTS
The inclusion criteria of the participants were considered to be educated adults. For our survey, these were defined as individuals at least 18 years old, with the ability to read and speak English. Convenient random sampling was used to select the participants. The questionnaire was completed by 737 participants (74% response rate). The median age of respondents was 32 ± 8 years. The demographic data of our sample was similar to Pakistan’s population in terms of gender, ethnicity and age. There were 52% females and 48% males in our sample, which is consistent with Pakistan’s demographics of 49% females and 51% males (Table 1). There were 47 % Punjabis, 15% Urdu speaking, 2% Baluch, 11% Sindhi, 19% Pathans and 6% other ethnicities in our sample. This corresponds to the ethnic proportions of the Pakistani population (Table 1). Similarly, the age of the participants of our study was comparable to the percentage distribution of age groups, as documented in the country’s official census [22].
| Total (N = 737) | Pakistan population* | |
|---|---|---|
| n (%) | (%) | |
| Gender | ||
| Female | 385 (52) | 49 |
| Male | 354 (48) | 51 |
| Age (years)** | ||
| 18–25 | 350 (47) | 20 |
| 26–35 | 246 (33) | 13 |
| 36–45 | 79 (11) | 9 |
| 46–55 | 55 (7) | 8 |
| 55+ | 7 (1) | 2 |
| Ethnicity | ||
| Punjabi | 333 (47) | 44 |
| Urdu speaking | 116 (15) | 8 |
| Baluch | 16 (2) | 4 |
| Sindhi | 81 (11) | 14 |
| Pathan | 143 (19) | 15 |
| Others | 48 (6) | 4 |
| Education | ||
| High school | 11 (2) | – |
| College | 326 (44) | – |
| Graduate/professional | 400 (54) | – |
6th population and housing census 2017.
Percentages of the total population above 18 years of age.
Demographic characteristics of study sample compared to Pakistan’s population
The pattern of responses shows that 85% of respondents (n = 630) identified the correct definition of coronavirus disease and 15% (n = 107) incorrectly indicated that the virus is not contagious and can never lead to death. Similarly, 92% of the participants (n = 679) were able to recognize the correct route of transmission while 8% (n = 58) were unable to do so. Noticeably, more than 21% of responses (n = 151) indicated the availability of a curative treatment for COVID-19 and 8% (n = 59) reported the presence of a vaccine.
Respondents’ accuracy in identifying preventive measures against the pandemic for themselves and others is presented in Figure 1. Responses show that hand washing was correctly identified by all the participants (n = 737, 100%). The majority of the participants (91%) considered avoiding contact as an effective preventive strategy and 86% deemed quarantine a preventive strategy. Similarly, 89% of respondents were aware of covering coughs as a precaution to limit disease transmission. More than 88% of respondents reported that wearing masks is effective in preventing the spread of COVID-19. However, only 77% of participants identified the use of disinfectant as a means to do the same.
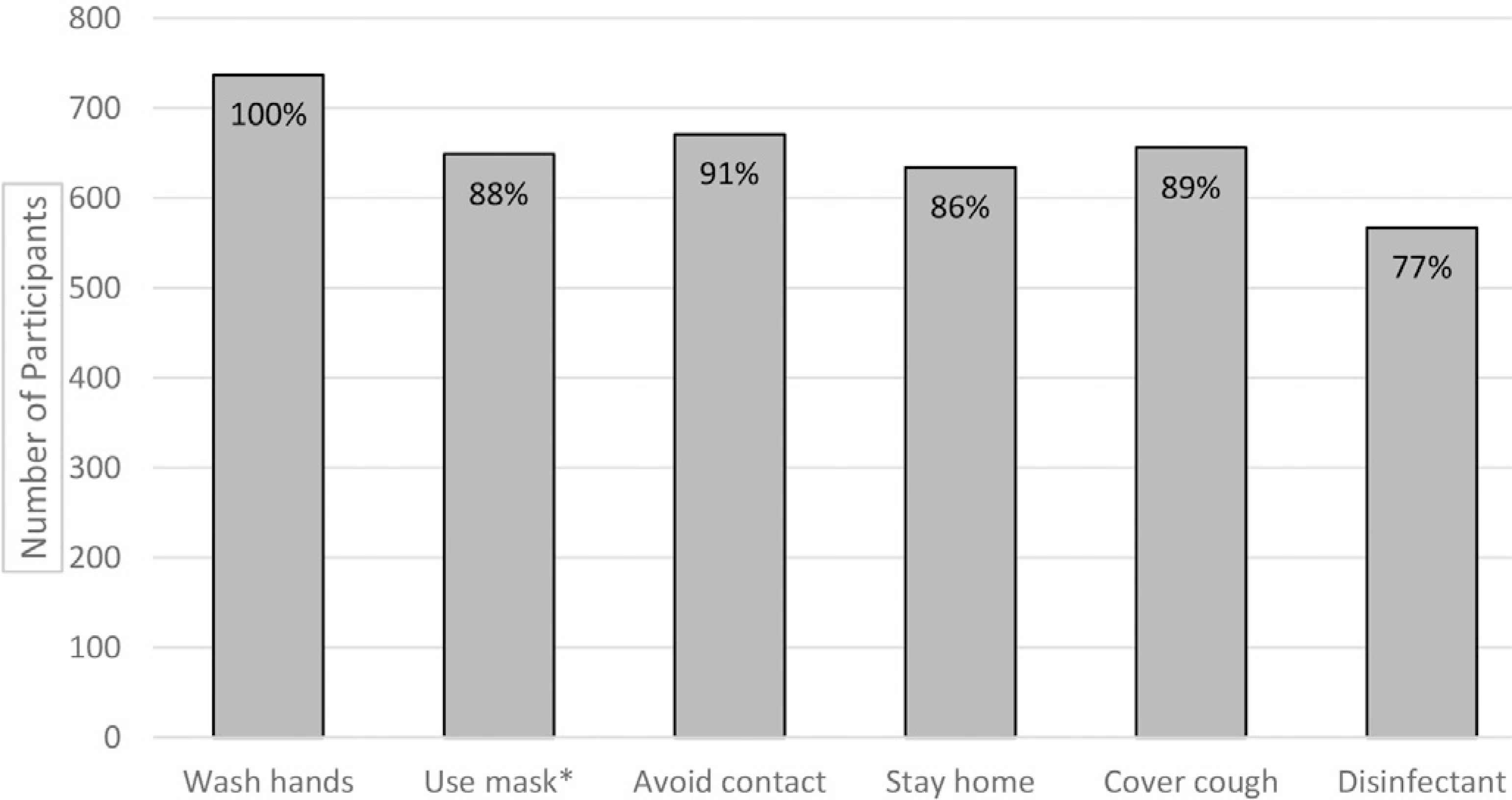
Measures identified by the participants as effective against COVID-19. *Preventive measure according to updated WHO guidelines.
Perceptions regarding the preventative role of non-biomedical supplements are given in Figure 2. The number of respondents expecting the novel virus to disappear in hot weather was 434 (59%). Hot lemon water and garlic/ginger were identified as protective against COVID-19 by 421 (57%) and 236 (32%) of respondents respectively. The percentage of participants considering herbal supplements as such was 38% (n = 280), while 29% (214) reported that raw onion had preventative qualities.
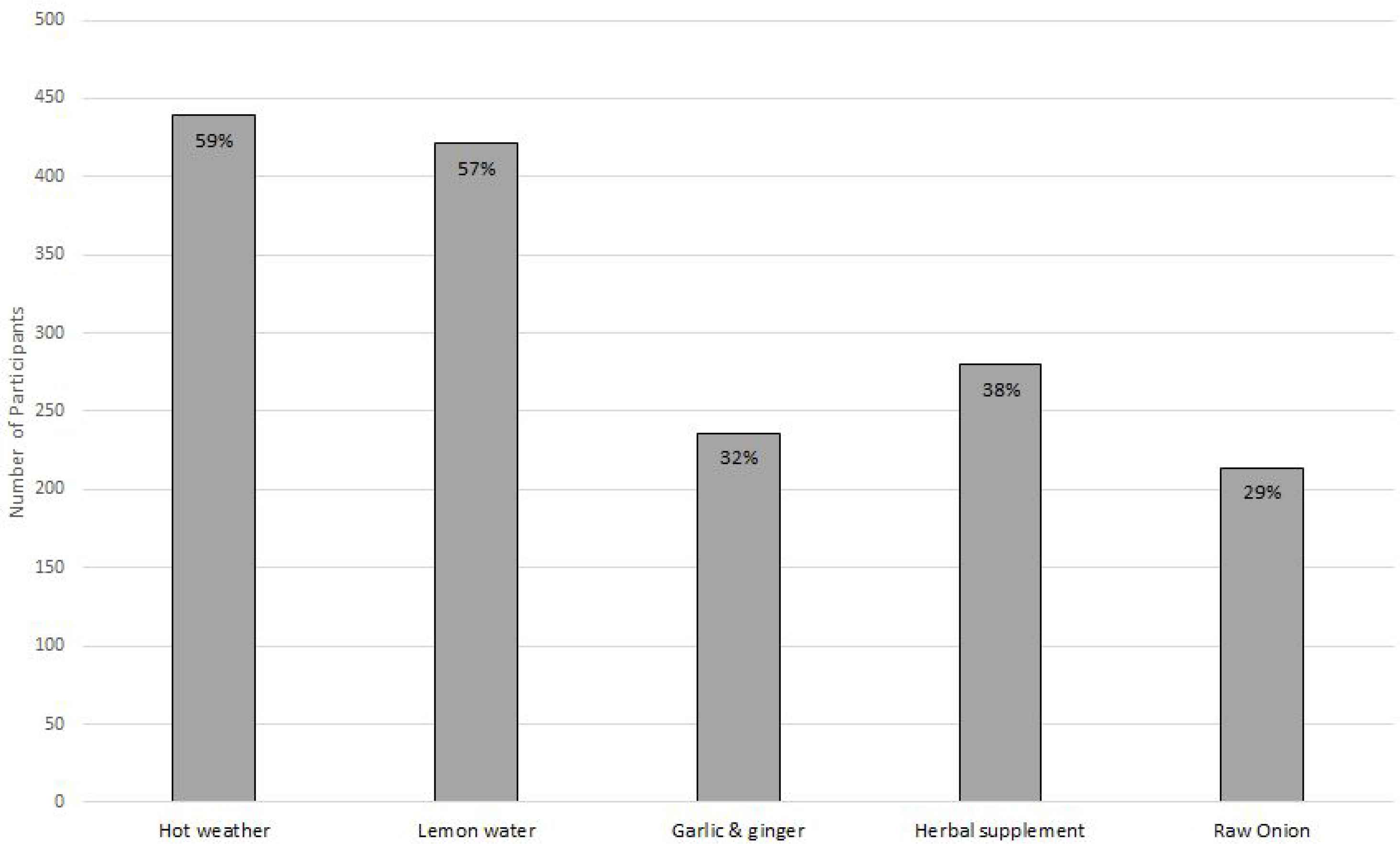
Participants perception of preventive measures based on myths.
An assessment of the cognitive (section I) and affective (section II) dimensions of risk perception via Likert scale is displayed in Tables 2 and 3 respectively. The midline value for perceived risk was 2. The results show that for section I cognitive domain, it was raised to 2.24 ± 1.34 (a total of eight items). The mean score assessing the affective domain was significantly higher at 3.01 ± 1 (a total of seven items). More than 65% (n = 479) thought that the risk of outbreak is greater than being communicated and 63% (463) did not trust the government to handle the situation alone. The percentage of neutral responses in cognitive assessment (24%) was higher than that of the affective one (15%). Of the respondents, 82% were very concerned about the outbreak. Most of the responses favoured strict measures including the closing borders (n = 555, 75%), placing all international travellers under quarantine (n = 615, 83%) closing all educational institutes (n = 611, 83%).
| Statements | Responses* | n (%)** | M ± SD*** |
|---|---|---|---|
| Section - 1: Cognitive risk perception associated with novel Coronavirus outbreak | |||
| My health will be severely damaged If I contract Coronavirus | A | 423 (57) | 2.37 ± 0.94 |
| N | 166 (23) | ||
| D | 148 (20) | ||
| I think Coronavirus is more severe than flu | A | 518 (70) | 2.53 ± 0.98 |
| N | 97 (13) | ||
| D | 122 (17) | ||
| Even if fall ill with another disease, I will not go to hospital because of risk of getting Coronavirus in hospital | A | 253 (34) | 1.85 ± 1.56 |
| N | 126 (17) | ||
| D | 358 (49) | ||
| Novel coronavirus will inflict serious damage in my community | A | 505 (69) | 2.53 ± 0.99 |
| N | 123 (17) | ||
| D | 109 (15) | ||
| Novel coronavirus will spread widely in Pakistan | A | 425 (58) | 2.39 ± 1.45 |
| N | 181 (25) | ||
| D | 131 (18) | ||
| I am more likely to get coronavirus than other people | A | 138 (19) | 1.69 ± 1.33 |
| N | 239 (32) | ||
| D | 360 (50) | ||
| I believe I can protect myself against the coronavirus | A | 384 (52) | 2.32 ± 1.54 |
| N | 205 (28) | ||
| D | 148 (20) | ||
| I believe I can protect myself against the novel coronavirus better than other people | A | 326 (44) | 2.26 ± 1.23 |
| N | 282 (38) | ||
| D | 129 (18) | ||
Note: 5-point Likert scale (Strongly agree/Agree = 3, Neutral = 2, Strongly disagree/Disagree = 1) N = 737.
Responses (A = Agree, N = Neutral, D = Disagree).
Values are n, number of responses (with percentages in parenthesis).
M = Mean, SD = Standard deviation.
Cognitive risk perception associated with novel coronavirus outbreak
| Statements | Responses* | n (%)** | M ± SD*** |
|---|---|---|---|
| I am very concerned about this outbreak | A | 608 (82) | 2.74 ± 0.99 |
| N | 72 (10) | ||
| D | 57 (8) | ||
| I believe the Govt is downplaying the risk | A | 479 (65) | 2.50 ± 1.08 |
| N | 120 (16) | ||
| D | 138 (19) | ||
| I do not trust that Govt officials can handle | A | 463 (63) | 2.4 ± 1.22 |
| N | 107 (14) | ||
| D | 167 (23) | ||
| I expect outbreak to get larger | A | 441 (60) | 2.4 ± 1.88 |
| N | 140 (19) | ||
| D | 156 (21) | ||
| All borders should be closed | A | 555 (75) | 2.5 ± 1.02 |
| N | 76 (10) | ||
| D | 106 (14) | ||
| All international travellers should be quarantined | A | 615 (83) | 2.77 ± 0.56 |
| N | 78 (11) | ||
| D | 44 (6) | ||
| All educational institutions should be closed | A | 611 (83) | 2.75 ± 0.55 |
| N | 66 (9) | ||
| D | 60 (8) |
Note: 5-point Likert scale (Strongly agree/Agree = 3, Neutral = 2, Strongly disagree/Disagree = 1) N = 737.
Responses (A = Agree, N = Neutral, D = Disagree).
Values are n, number of responses (with percentages in parenthesis).
M = Mean, SD = Standard deviation.
Affective risk perception of the participants on handling of COVID-19
Responses indicate that most of the participants (n = 617, 84%) learned about the outbreak through the media. Health officials were the source of this information for 13% (n = 94) and only 4% (n = 26) were informed about the outbreak by their family and friends.
The summary of respondents’ perceived trust in sources of information on disease is presented in Figure 3. Most respondents (n = 236, 32%) trusted health care professionals for information about the pandemic. The health officials were the next-most trusted, followed by (133, 18%), television (n = 117, 16%), family (n = 96, 13%) and newspapers (n = 86, 11%). Only 9% of respondents trusted social media for reliable information (n = 69, 9%) (Figure 3).
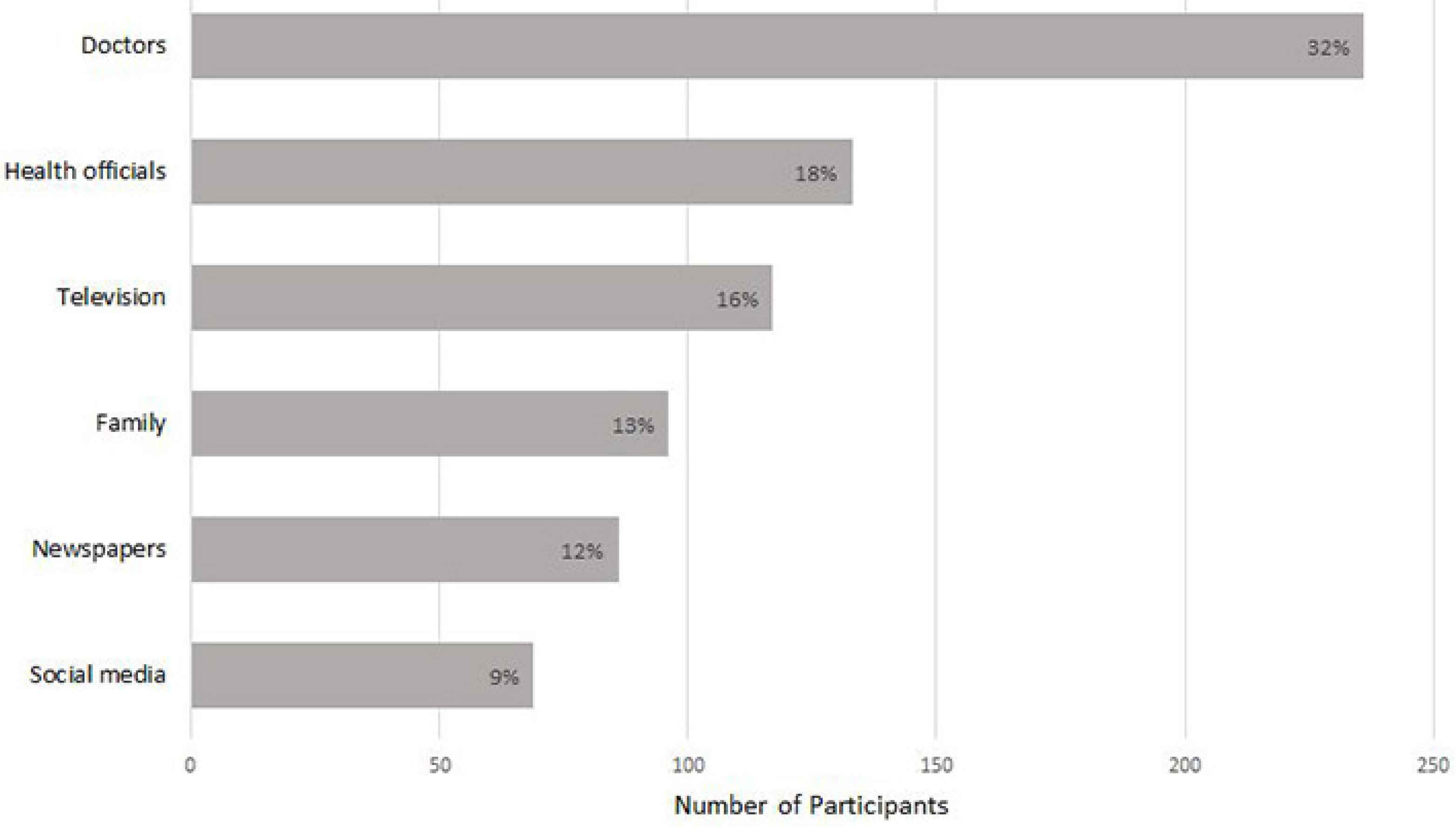
Participants rating based on trust in sources of information.
The study suggests that respondents would most prefer health authorities to be at the forefront of the response to this outbreak (n = 255, 35%). Participants then expressed a preference for the armed forces (n = 211, 29%), the government (n = 196, 26%) and religious leaders 10% (n = 75) (Figure 4).
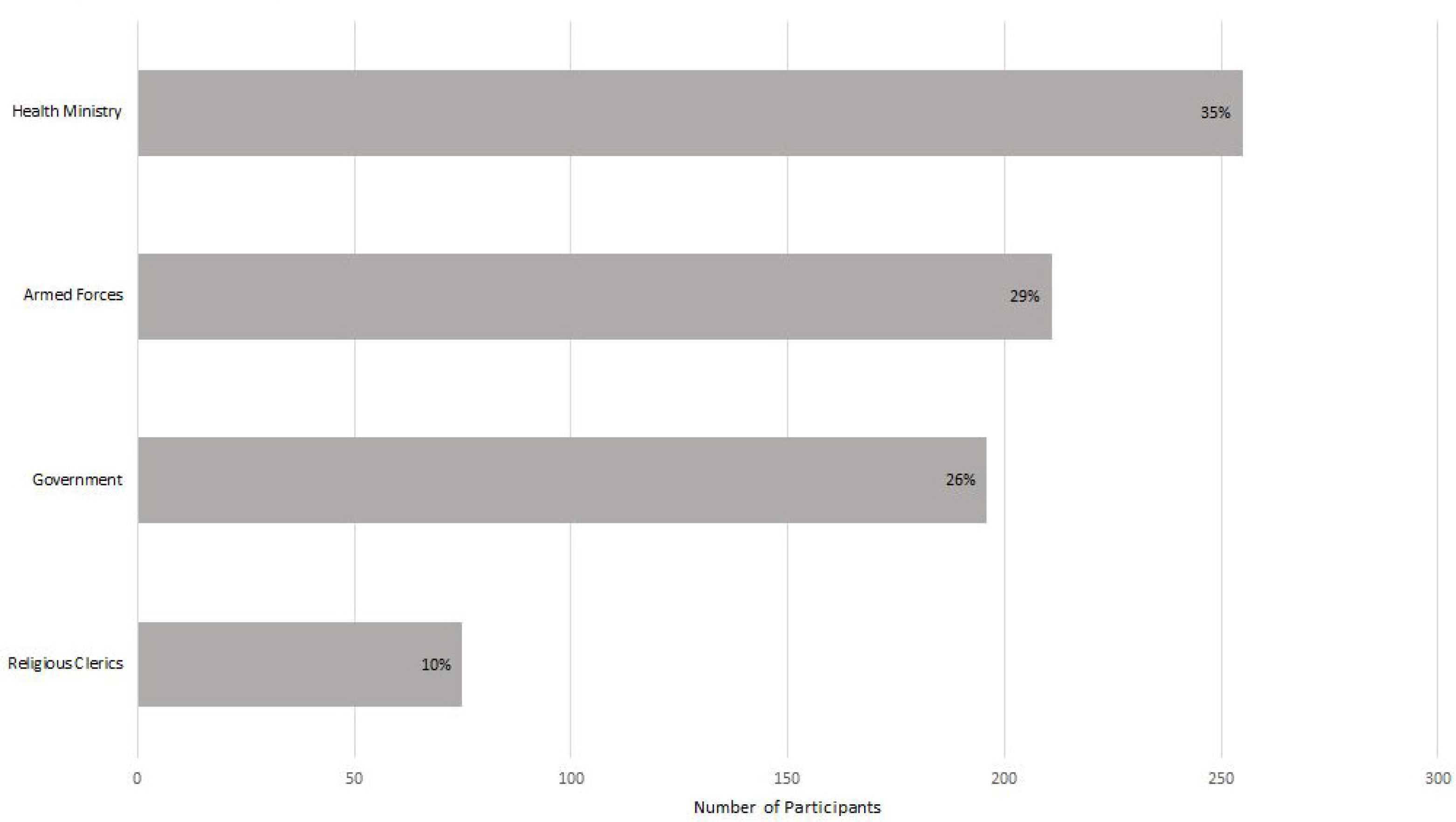
Participants choice for who should lead Pakistan’s response to COVID-19 outbreak.
4. DISCUSSION
The results of this study account for the initial period of the pandemic in Pakistan - March 20–27, 2020, just before extensive communal transmission of coronavirus [23]. For the first time in the region, it provides an insight into public knowledge and their risk perceptions about COVID-19. It also delineates citizens’ trust in local authority figures and information sources.
Overall, responses show that there are gaps in knowledge and misinformation regarding the transmission, course, and available treatment for COVID-19. However, public awareness of preventive strategies was fairly accurate. Findings show a high prevalence of risk perceptions. We also report that doctors and health professionals are deemed the most trusted sources of information, in contrast to social media. The findings of this study convey public concerns and deficiencies in knowledge about coronavirus, with important implications for policymakers.
Respondents had misconceptions about, and misplaced confidence in, non-bio-medical treatment regarding COVID-19 (Figure 2). Approximately 30% of the participants in our study were of the opinion that onions, garlic, and ginger are beneficial for treating COVID-19. This belief in the protective role of herbs is emerging as a pattern worldwide [24]. Although most of these alternative herbal therapies have been shown to boost the immune system, very little clinical research is available on their efficacy [24]. Moreover, there is insufficient information on the dosage and form necessary to achieve a particular medicinal outcome. Thus, further research is required before the therapeutic or preventive efficacy of these non-biomedical alternatives can be confirmed. Additionally, using these substances can give a false sense of protection against disease, making people less cautious. Indeed, while some natural remedies and herbs might be useful in preventing disease by boosting immunity, other substances can be fatal [25]. Colloidal silver is an example of the latter. A non-biomedical material believed to protect against coronavirus, the United States Food and Drug Administration has warned against its use by the general public. This is due to serious side effects like Argyria [26]. Despite their potential to be hazardous, such substances continue to gain popularity [27]. To better inform the public, a section on myth-busters was added to the WHO’s official site [28]. Similar initiatives should be undertaken in Pakistan. Mass media campaigns including radio, television, newspapers, magazines, articles, books, pamphlets, posters, seminars, and workshops could be employed to raise awareness of, and combat dangerous myths surrounding, COVID-19.
A large majority of our respondents (59%) believed that the pandemic would end with the arrival of warm weather (Figure 2). This assumption may be based on the course of other types of seasonal flu. However, recent research suggests that cases of COVID-19 are not likely to decline in the spring or summer [29]. This should be integrated into campaigns to ensure continued compliance with guidelines, and drive down the risk of transmission, as the weather changes.
The participants responses show that they were sufficiently knowledgeable about preventive measures against COVID-19 (Figure 1). All respondents identified hand washing as an effective measure to prevent novel coronavirus transmission. Similarly, a majority of the participants were able to identify social-distancing and covering their cough as preventive strategies. This could be the result of extensive countrywide campaigns focussing on strategies to prevent against the pandemic [30].
Most respondents identified masks as an effective preventive measure (Figure 1). This is in accordance with recently updated WHO guidance [31]. Evidence suggests that high viral load in the early stages of disease frequently causes transmission from asymptomatic cases [32]. Using masks might promote hygiene and awareness [33]. Furthermore, in a populous country like Pakistan, its use might intercept the droplets spreading from visibly healthy carriers. The campaigns must continue to propagate the use of masks in order to curtail the pandemic. Knowledge about the protective function of disinfectant was less widespread than that of other precautions against the spread of COVID-19. More emphasis must be placed on its use during mass campaigns through the media.
Our results revealed higher mean risk perception in relation to COVID-19. Unprecedented in spread and scale, this pandemic has led to collective anxiety and fear [34,35]. Negative emotions, like these, have been shown to amplify risk perception [36,37]. Additionally, during past disasters, citizens’ understanding of the gravity of the situation, is also influenced by awareness, knowledge, past experiences, their sense of control [38].
Heightened risk perceptions in our sample were probably a result of fear of susceptibility to novel coronavirus, lack of disease associated information and anticipation of a possible future threat of infection [35].
Although risk perception was found to be higher in both cognitive and affective domains, the mean value of perceived risk in the affective domain was significantly higher than that in the cognitive domain. Higher affective perceived risk has been observed in past health disasters [39–42]. An affective reaction can be described as an immediate, intuitive, and associative response that modulates thought processing and judgment [43]. Contrastingly, a cognitive response is based on facts and rational thinking [44]. Worry and high levels of concern can be categorized as emotional constructs and have been correlated more strongly with affective responses than cognitive responses [44]. Unsurprisingly, the higher affective risk perception in our study reflects the emotional unrest during a health disaster of the present magnitude.
Our findings show that neutral responses were higher in cognitive items as compared to those in the affective domain. This could be because participants were more certain about their feelings as compared to their comprehension of facts relating to COVID-19. Previous studies complement these findings, associating lower uncertainty with affective risk perceived items versus cognitive items [40]. When risk is based on intuition, and feelings act as a cue for judgements, decisions are processed faster and there is less ambiguity than in rational thought processes [44]. This might also be the reason that the respondents were certain to implement aggressive measures; quarantine for all international passengers, strict travel restrictions, and the closure of all educational institutions. Such heightened sensitivity has been seen previously when fear influences judgement [45].
The coronavirus pandemic has led to an infodemic. Studies suggest that excessive media coverage of disaster might also induce anxiety and increase risk perceptions [46]. Furthermore, it has been suggested that perceived risk may be affected by the way information is presented [46,47]. In past health disasters, high anxiety and perceived risk have been associated with misinformation about, and misinformation of, disease [15,16]. The expertise and credibility of the authorities imparting information has also been shown to significantly impact perceived risk during past epidemics [48,49].
The trustworthiness of the sources of information may therefore shape public perceptions [50,51]. Considering our results, doctors and health professionals were deemed to be the most trusted sources of information, in contrast to social media (Figure 3). Yet, the potential for the latter to spread misinformation and create mass hysteria is indisputable. This has invariably undermined disease control in the past. To avert this, efforts should be made to separate fact from fiction. These may decrease apprehension, increase compliance with control measures, and improve outcomes [52]. Mass awareness campaigns should be launched to provide reliable and accurate information. Certainly, a lack of information leads to the prevalence of misconceptions and myths which cause people to over or underestimate the gravity of the crisis. Updated, simplified data, and developmental progress should be communicated effectively through reliable media. Moreover, the uncertainty of circumstances has led to negativity which needs to be addressed. Focussed efforts are also required to develop diagnostic and effective treatment strategies. This may involve calling all scientific and healthcare professionals within the country to collaborate to help model low cost ventilators and sanitizers. Involving the local community in volunteering and awareness campaigns could allow the public to regain a sense of control and help decrease the anxiety associated with inaction.
Our results clearly show that people would like the health authorities to control the disaster, in lieu of the government (Figure 4). Respondents most likely favoured the former for their greater perceived expertise in the field of healthcare. The trust in the religious establishment is also at an all-time low. This is probably the result of recent reports of mismanagement and long-standing epidemics in the region due to the irrational approach of religious factions [53]. Presently, extremist clerics are rejecting social distancing recommendations and refusing to limit congregational prayers [53]. Our results underscore educated respondents’ distrust of clerics. However, this is in stark contrast to the inclinations of the conservative rural majority. This religious and social divide subverts collective action against coronavirus. This is a vulnerability which needs to be addressed. Efforts should focus on bringing the change from within to build trust on, and promote cooperation from, both sides.
Present findings can help health authorities to construct risk communication planning and implementation [30]. In our sample, higher risk perception depicts stress which could give rise to mental health problems. Psychological counselling through media, and over a hotline, should be available to allow people to cope better with their fears. Social workers should assist the most vulnerable in society. With decreased anxiety and increased rational thinking, social disruption can also be minimized.
Risk communication and community engagement is an essential component of health policy for effective action plans [46,47]. Doctors and other health professionals have been identified by our representative sample as the most trusted sources. Hence, two-way risk communication between health professionals and at-risk populations will facilitate the implementation of precautionary plans. Communicating with the public in a regular and proactive manner can further public confidence and social cohesion. This might lead to circumstances which limit the spread of disease. Involving the local community in volunteering and awareness campaigns by health professionals could also allow the public to regain a sense of control, helping decrease the anxiety associated with inaction.
5. LIMITATIONS
Although we provide timely and relevant data, there are certain limitations to this study. Our survey was administered online and therefore subject to selection bias, as the availability of a computer, tablet, or smartphone was a prerequisite to participate. Moreover, our sample predominantly comprised educated individuals residing in urban areas and did not include the uneducated rural population.
6. CONCLUSION
Our findings are pivotal and may play a role in mobilizing stakeholders to employ data-driven interventions in the management of the pandemic. The study reveals that there are significant gaps in public knowledge about COVID-19. To address this, we recommend consistent messaging and more comprehensive education programs with a focus on dispelling myths and fact-checking conflicting information. The results of the survey also suggest a higher risk perception, especially in the affective domain. This should be addressed by more effective and structured risk communication. For instance, clinicians and scientists can communicate directly with the public through media platforms to counsel and convey realistic risk. Their expert advice may lend greater credibility to government advice. This will not only motivate the public to take appropriate action but will also help mitigate widespread anxiety arising from a disproportionately high-risk perception. Health officials, government authorities, and religious leaders should make a concerted, cohesive effort to handle this crisis effectively.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
AH contributed in conception and design of the study, visualization and supervision. AH, SM, RM, FM and HAB contributed in acquisition of data. AH, SM, RM, FM, HAB, AA and OK contributed in analysis and interpretation of data. AH, SM, RM, FM, HAB, AA and OK contributed in drafting the article or revising it critically for important intellectual content. AH, SM and AA contributed in final approval of the version to be submitted.
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial, or non-for-profit sectors.
ACKNOWLEDGMENTS
The authors would like to express their gratitude to our participants who shared their valuable time to complete the survey.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Ayesha Haque AU - Sadaf Mumtaz AU - Rafia Mumtaz AU - Farheen Masood AU - Hudebia Allah Buksh AU - Amal Ahmed AU - Osama Khattak PY - 2021 DA - 2021/01/20 TI - Assessment of Knowledge, Perceptions and Perceived Risk Concerning COVID-19 in Pakistan JO - Journal of Epidemiology and Global Health SP - 186 EP - 193 VL - 11 IS - 2 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.210109.001 DO - 10.2991/jegh.k.210109.001 ID - Haque2021 ER -