
Epidemiological Profile of Meningitis following Pentavalent Vaccination in Iran: Impact of Vaccine Introduction
 , Manoochehr Karami1, 2, *, , Seyed Mohsen Zahraei3, Iraj Sedighi4, Fatemeh Azimian Zavareh3
, Manoochehr Karami1, 2, *, , Seyed Mohsen Zahraei3, Iraj Sedighi4, Fatemeh Azimian Zavareh3- DOI
- 10.2991/jegh.k.210330.001How to use a DOI?
- Keywords
- Haemophilus influenzae; meningitis; vaccines; Iran
- Abstract
Ensuring the effectiveness of the Haemophilus influenza type b (DTwP-Hib-HepB) vaccine in reducing meningitis is an essential approach in evaluating the effectiveness of the vaccine. The study aimed to address the epidemiology of meningitis following pentavalent vaccination in Iran. Data on meningitis patients from 21st March 2011 to 21st July 2018 were extracted from the National Notifiable Diseases Surveillance System. This information was divided into two equal periods before the pentavalent vaccine introduction (21st March 2011 to 17th November 2014) and after the introduction (18th November 2014 to 21st July 2018). The number of patients in the study period was 53,174 cases. More than 55% of patients were under 5 years old. Males (63.34%) were more than females (36.06%). The death rate was reduced to 2.1%; also, the proportion of confirmed cases caused by H. influenzae type b was 6.7% before the pentavalent vaccine introduction. The corresponding value following vaccine introduction equals to 3.6%. The proportion of children under five has decreased from 4.4% to 1.9%. This value indicates a 46.2% decrease in the meningitis of all ages and a 57% decrease in children under five dues to H. influenzae vaccination. The results of the study indicate the effectiveness of the vaccine due to changes in meningitis caused by H. influenzae type b after vaccination compared with no vaccination. Therefore, it is advisable to continue the full immunization coverage with the pentavalent vaccine.
- Copyright
- © 2021 The Authors. Published by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Meningitis is a disease caused by inflammation of the protective lining of the brain and spinal cord called meninges [1]. The disease is often caused by viral, bacterial, and fungal infections and is a life-threatening condition that affects about one and a half million people and kills about 170,000 people annually [2,3]. Untreated meningitis in 50% of cases can lead to severe brain death and injury [4]. The most common symptoms of the disease include nausea and vomiting, ague, neck stiffness, myalgia (muscle pain), the high fever usually between 39° and 41°, and sensitivity to light [1,4].
Bacterial meningitis can be caused by a variety of factors, including S. pneumonia, N. meningitis, and H. influenzae. Failure to receive the H. influenzae vaccine is one of the most important causes of meningitis in children under 5 years of age [5]. Haemophilus influenza annually results in the deaths of more than 370,000 children under the age of 5 in the world. Given the significant burden of disease caused by these agents, the World Health Organization has recommended adding the H. influenza type b, Hib vaccine to the countries’ immunization program. Like many developing countries and to reduce the number of cases of pneumonia and subsequent meningitis, Iran has added the pentavalent (DTwP-Hib-HepB) vaccine to the routine immunization program at 2, 4 and 6 months old age since 18th November 2014 [6–11]. Based on the National Immunization Program, almost all children are currently vaccinated against tuberculosis, hepatitis B, polio, diphtheria, pertussis, tetanus, H. influenzae type b, measles, rubella and mumps. Vaccination schedule for children includes newborns, 2, 4, 6, 12, 18 months and 6 years’ ones. Also, according to the study period, the vast majority of children born on 19th September 2014, the pentavalent vaccine have received. The rate of vaccination coverage in the target groups is 99% [12,13].
Concerning the evaluation of vaccine effectiveness from studies, a case-control study in Uganda and the US on children under 5 years of age reported that the efficacy of the vaccine after injection was more than 93% and 65%, respectively. Another study in Kenya carried out as a cohort, and those receiving the vaccine were considered to have reduced the incidence of meningitis after vaccination from 71% to 8%. Another study in a randomized trial in India found that the vaccine’s effectiveness in protecting meningitis was 94% [14–17].
The constituents of the pentavalent vaccine include H. influenzae type b, hepatitis B, diphtheria, tetanus, and pertussis. The age of vaccination is 2, 3, and 6 months [18–20]. Given the recent implementation of the pentavalent vaccination program in the country and the recommendations of the World Health Organization on the periodic evaluation of vaccine effectiveness and despite extensive studies on the efficacy of this vaccine, so far, no studies have been conducted in Iran. There were no studies to evaluate the burden of the disease and the impact of the vaccine on meningitis.
For this reason, an epidemiological study of meningitis from 3 years and 8 months before and 3 years and 8 months after vaccination and comparing the two was one of the critical approaches in evaluating the effectiveness of the pentavalent vaccine. This study aimed to determine the epidemiological profile of meningitis following the pentavalent vaccine was added in Iran.
2. MATERIALS AND METHODS
This descriptive study was used to describe the epidemiological profile of meningitis in the number of cases from 21st March 2011 to 21st July 2018. All meningitis patient’s information including demographic information (age, sex, and occupation), date of disease incidence, geographic area and laboratory information such as biochemical tests, microbiology (culture, gram staining) and serology (latex), final diagnosis, vaccination status, symptoms, and outcome were extracted from the National Notifiable Diseases Surveillance System [21,22].
In this study, patient information was divided into two equal periods before (21st March 2011 to 17th November 2014), and after vaccination (18th November 2014 to 21st July 2018) and from suspicion aspects, patients were divided into three groups as suspected, probable and confirmed according to the following criteria [23,24].
2.1. Suspected
Anyone at any age with a fever above 38.5°C and one of the symptoms of neck stiffness, decreased consciousness, meningeal symptoms (headache, vomiting, and any sudden neurological complications), pediatric bulged fontanel suspected case was considered as meningitis case.
2.2. Probable
Any suspected case that his cerebrospinal fluid test shows at least one of the following:
- •
Turbid or purulent appearance.
- •
Increased white blood cells more than 100 cells/mm3.
- •
Increased white blood cells 10–100 cells/mm3 plus protein increased above 100 mm/dl or reduced glucose to <40 mg/dl.
- •
One of the following results in gram staining:
- 1.
Gram-negative bacilli (suggestive of H. influenzae).
- 2.
Gram-negative diplococci (suggested by N. meningitis).
- 3.
Gram-positive diplococci (suggestive of S. pneumonia).
- 1.
2.3. Confirmed
Cases of positive culture or pathogenic mass antigen found in the cerebrospinal fluid or blood of a person with clinical symptoms. After extracting data from the National Notifiable Meningitis Surveillance System, data were entered into Excel software.
Descriptive statistics indices, including mean, frequency, percentages, tables, and graphs were used to describe the study population, and data were analyzed using Stata 14 software. ArcGIS ver 9.3 software was also used to plot the disease status in different parts of the country. The geographical distribution of the confirmed and probable cases of meningitis before and after the pentavalent vaccination was used to obtain data on the population of the country reported on the official website of the Iranian Statistical Center.
The present study has been registered and approved by the Ethics Committee of Hamadan University of Medical Sciences (IR.UMSHA.REC.1397.737).
3. RESULTS
During the study, 53,174 cases from 1-day to 110-year-old patients with meningitis were enrolled, which 28,471 were pre-vaccinated with the H. influenzae type b vaccine, and 24,703 cases were after vaccination implementation. Also, 40,785 (76.7%) were suspected, 10,574 (19.8%) probable and 1815 (3.4%) were confirmed.
As Table 1 shows, given the equal number of months before and after immunization, we see a 3768 decrease in the meningitis cases after vaccination. The number of suspects decreased from 21,541 cases before implementation to 19,244 after implementation. The probable cases decreased from 5969 to 4605, and the number of confirmed cases from 961 before the vaccination to 854 after that. Of all probable and confirmed cases of meningitis, 4468 (36.06%) were female and 7848 (63.34%) were male and 73 (0.6%) were unknown. The meningitis rate was higher in male cases than females before and after the vaccination program.
| Variables | Categories of variable | Before vaccine integration, N (%) | After vaccine integration, N (%) |
|---|---|---|---|
| Classification of meningitis cases | Suspected | 21541 (75.6) | 19244 (77.9) |
| Probable | 5969 (21.0) | 4605 (18.6) | |
| Confirm | 961 (3.4) | 854 (3.5) | |
| Sex (probable and confirm) | Male | 4376 (63.1) | 3472 (63.6) |
| Female | 2500 (36.0) | 1968 (36.1) | |
| Unknown | 54 (0.8) | 19 (0.3) | |
| Location (probable and confirm) | Urban | 5241 (75.6) | 4285 (78.5) |
| Rural | 1605 (23.2) | 1138 (20.8) | |
| Others | 34 (0.5) | 17 (0.3) | |
| Unknown | 50 (0.7) | 19 (0.4) | |
| Factor (confirm) | Haemophilus influenza (People over 5 years) | 22 (2.3) | 14 (1.6) |
| Streptococcus pneumonia | 172 (17.9) | 114 (13.3) | |
| Neisseria meningitis | 49 (5.1) | 79 (9.3) | |
| Viral | 137 (14.2) | 132 (15.5) | |
| Other things | 539 (56.1) | 498 (58.3) | |
| Haemophilus influenza (children under 5 years) | 42 (4.4) | 17 (1.9) | |
| Occupation (probable and confirm) | Child | 3035 (43.8) | 2221 (40.7) |
| Baby | 875 (12.6) | 735 (13.5) | |
| Housewife | 702 (10.1) | 646 (11.8) | |
| Student | 741 (10.7) | 497 (9.1) | |
| Self employed | 596 (8.6) | 527 (9.7) | |
| Unemployed | 210 (3.0) | 127 (2.3) | |
| Retired | 188 (2.7) | 205 (3.8) | |
| Manual worker | 143 (2.1) | 91 (1.7) | |
| Others | 440 (6.3) | 410 (7.4) | |
| Outcome of the disease | Death | 590 (2.7) | 461 (2.1) |
| Recovery, treatment | 20851 (97.3) | 20894 (97.9) |
Basic features of meningitis cases from 21 March 2011 to 22 July 2018
Findings showed that out of 12,389 confirmed and probable meningitis cases, 76.89% were in urban areas, 22.26% in rural areas, and 0.41% in nomads and other regions, and information was also 0.5% missed. The proportion of patients in urban areas increased from 75.6% to 78.5% after vaccination, but the ratio of the rural regions decreased.
Occupational findings show that 55.43% of patients were children under 5 years and infants, 10.88% housewives, 3.17% retirees, 2.72% unemployed, and the rest were other occupations.
The proportion of meningitis in children under 5 years before vaccination was 43.8%, which decreased to 40.7% after vaccination, but increased from 12.6% to 13.5% in infants.
There were 1815 cases of confirmed meningitis, of which 95 (5.2%) were pathogenic H. influenzae type b, 286 (15.7%) were Streptococcus pneumonia, 128 (7%) were due to N. meningitis, 269 cases (14.8%) were due to viral causes, and 1.037 cases (57.1%) were due to other microorganisms. The number of confirmed cases of meningitis due to H. influenzae type b before the pentavalent vaccine was 64, indicating a 6.7% proportion of this factor compared to the total cases before vaccination, 31 after vaccination. The case has declined to 3.6% of all cases following vaccination. This represents a 46.2% decrease in cases of H. influenzae type b meningitis at all ages compared to before and after vaccine inoculation. Of the 95 cases that were caused by H. influenzae type b, 59 were children under the age of 5, in other words, 56% of patients with H. influenzae were children under 5 years. The reduction in the number of cases in children under 5 years of age was 57% compared to pre- and post-vaccination, decreasing from 42 to 17, and the proportion of the disease in these children compared to all patients before and after vaccination 4.4–1.9%. The results of the study show that the effect of the vaccine in the population under 5 years old was greater than the population over 5 years old. It is because of the high coverage of vaccinations in this age group. On the other hand given that, meningitis is one of the most important diseases in childhood, the higher vaccination coverage in the target group, the lower the possibility of infecting children. Also, this disease is one of the contagious diseases, so with the high coverage of the vaccination in the target group, the transmission of the disease from person to person will be reduced and will prevent the infection of sensitive people in the community who have not yet received the vaccine. This is due to the creation of Herd immunity at the community level.
The number of cases of S. pneumonia decreased from 172 to 114 but increased due to N. meningitis (49–79). The number of deaths before meningitis was 590 (2.7%) but decreased to 461 (1.2%) after the program.
Comparison of meningitis cases before the vaccination program and after the implementation in the provinces of Iran shows that the number of cases in 26 out of the 31 provinces has decreased.
Results of the study showed that 5697 cases (47.09%) were under 5 years of age, and 1305 cases (10.79%) were in the age range of 5–10 years. Other cases were older, indicating the importance of attention being paid to children under 5. Comparing the number of meningitis cases under 5 before and after the vaccination program showed a decrease from 3075 to 2622 cases, which is also true in people aged 5–15 years.
The results of this study show that out of 95 confirm patients diagnosed with H. influenzae type b, 91 cases (95.8%) did not receive the H. influenza vaccine, and only four cases (4.2%) received the vaccine.
According to Table 2, 90.7% of patients showed a fever, 57.9% vomiting, 53.8% headache, and 26.3% neck stiffness. Also, Figure 1 shows the number of cases of meningitis due to H. influenza type b has declined significantly in the years following the vaccine.
| Variables | Variable levels | N (%) |
|---|---|---|
| Fever | Yes | 3081 (90.7) |
| No | 195 (5.7) | |
| Unknown | 123 (3.6) | |
| Neck stiffness | Yes | 893 (26.3) |
| No | 2114 (62.2) | |
| Unknown | 392 (11.5) | |
| Decreased consciousness | Yes | 915 (26.9) |
| No | 2092 (61.6) | |
| Unknown | 392 (11.5) | |
| Headache | Yes | 1828 (53.8) |
| No | 1137 (33.4) | |
| Unknown | 434 (12.8) | |
| Vomit | Yes | 1967 (57.9) |
| No | 1243 (36.6) | |
| Unknown | 189 (5.5) | |
| Outstanding branding | Yes | 141 (4.1) |
| No | 2848 (83.8) | |
| Unknown | 410 (12.1) | |
| Seizure | Yes | 778 (22.9) |
| No | 2343 (68.9) | |
| Unknown | 278 (8.2) | |
| Kernick | Yes | 147 (4.3) |
| No | 2463 (72.5) | |
| Unknown | 789 (23.2) | |
| Brodzynski | Yes | 114 (3.4) |
| No | 2459 (72.3) | |
| Unknown | 826 (24.3) |
Clinical symptoms of meningitis in Iran from 20 March 2016 to 22 July 2018
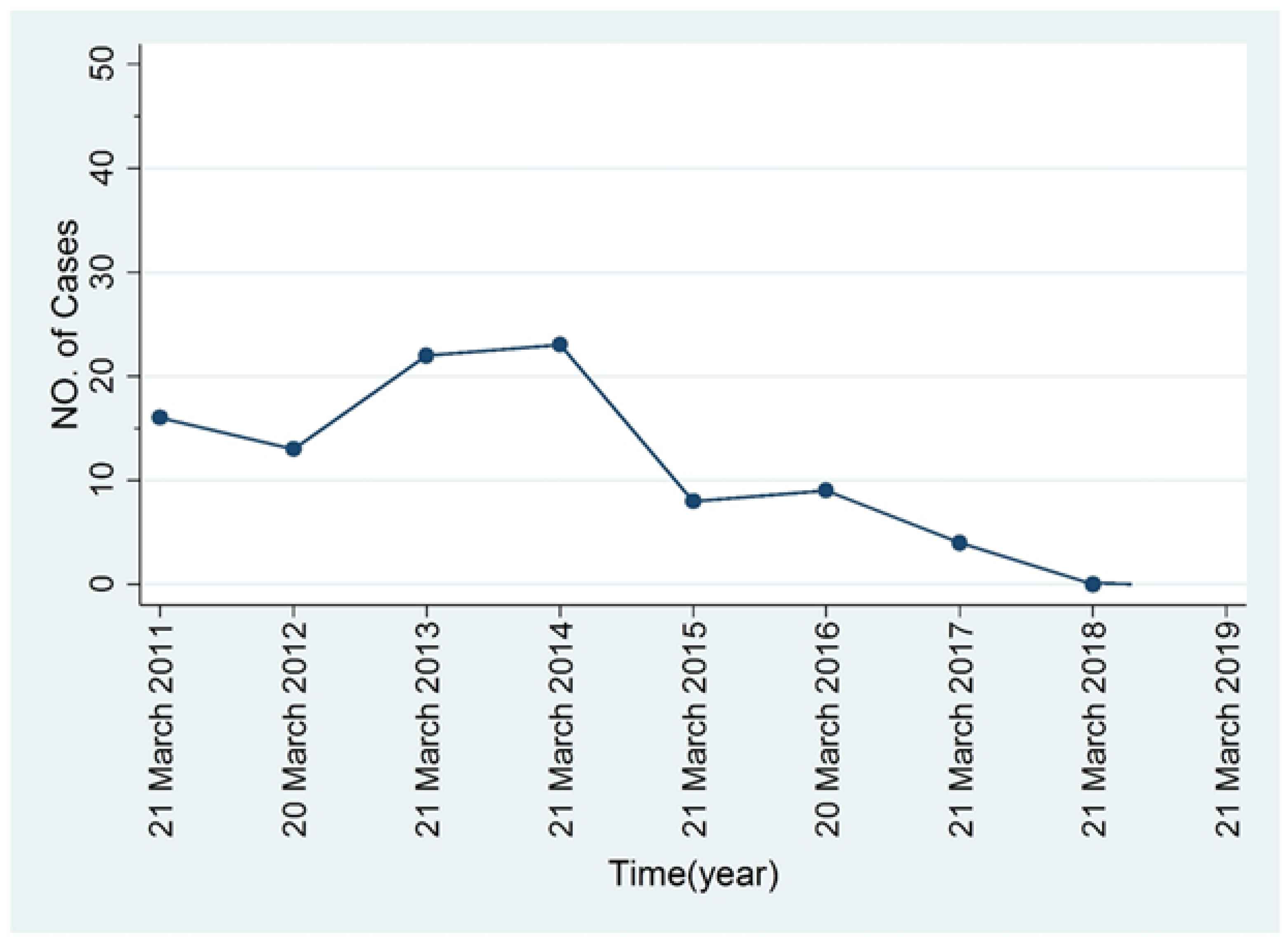
Time trend of the number of confirm cases of meningitis caused by Haemophilus influenzae type b.
According to Figures 2 and 3, the geographical distribution of confirmed and probable meningitis cases before and after the pentavalent vaccination indicates a significant reduction in meningitis cases based on Geographical Information System (GIS) software. All of depicted maps in the manuscript are own source.
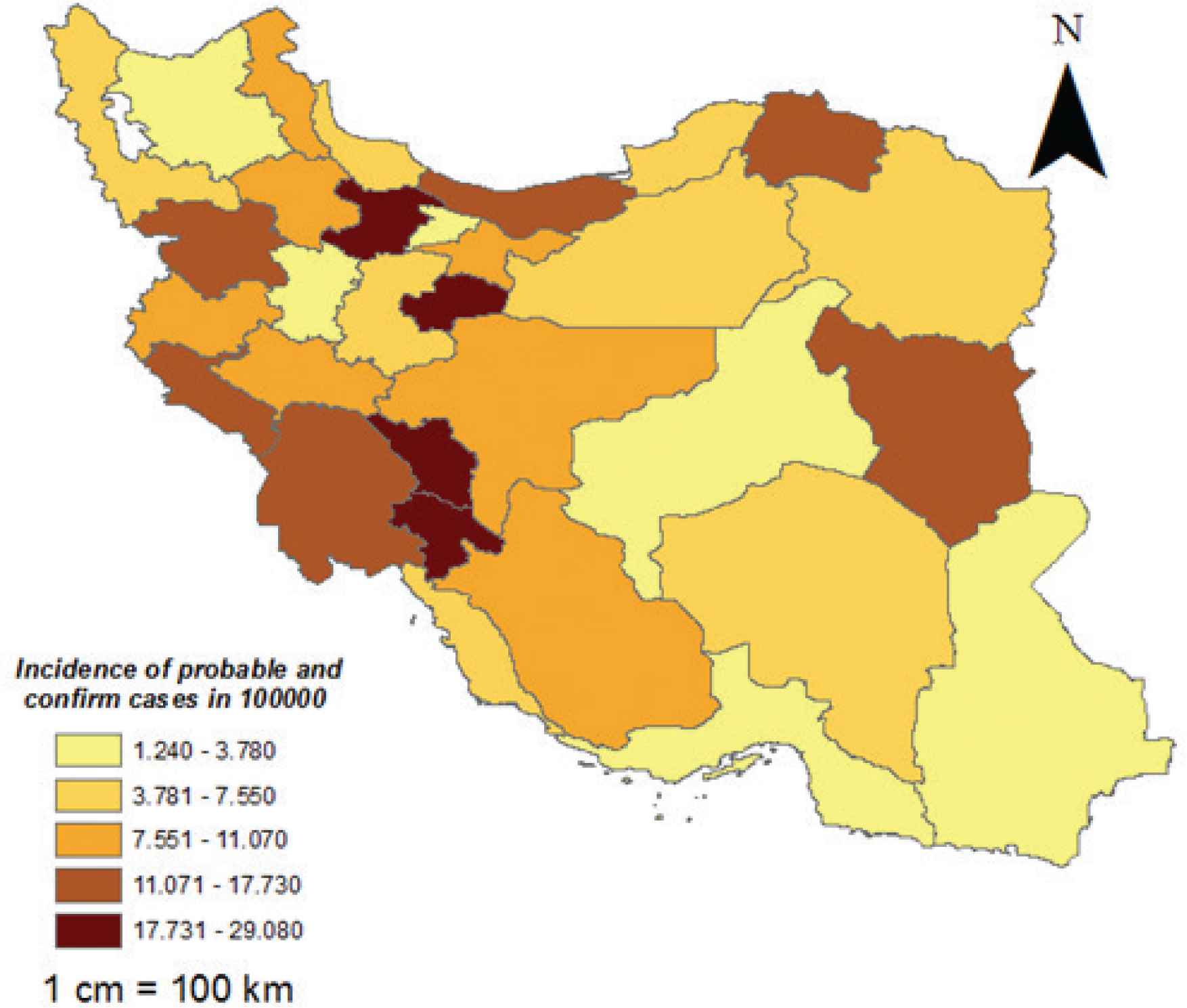
Geographical distribution of probable and confirm incidence of meningitis by incidence (in a population of 100,000) prior to pentavalent vaccine administration.
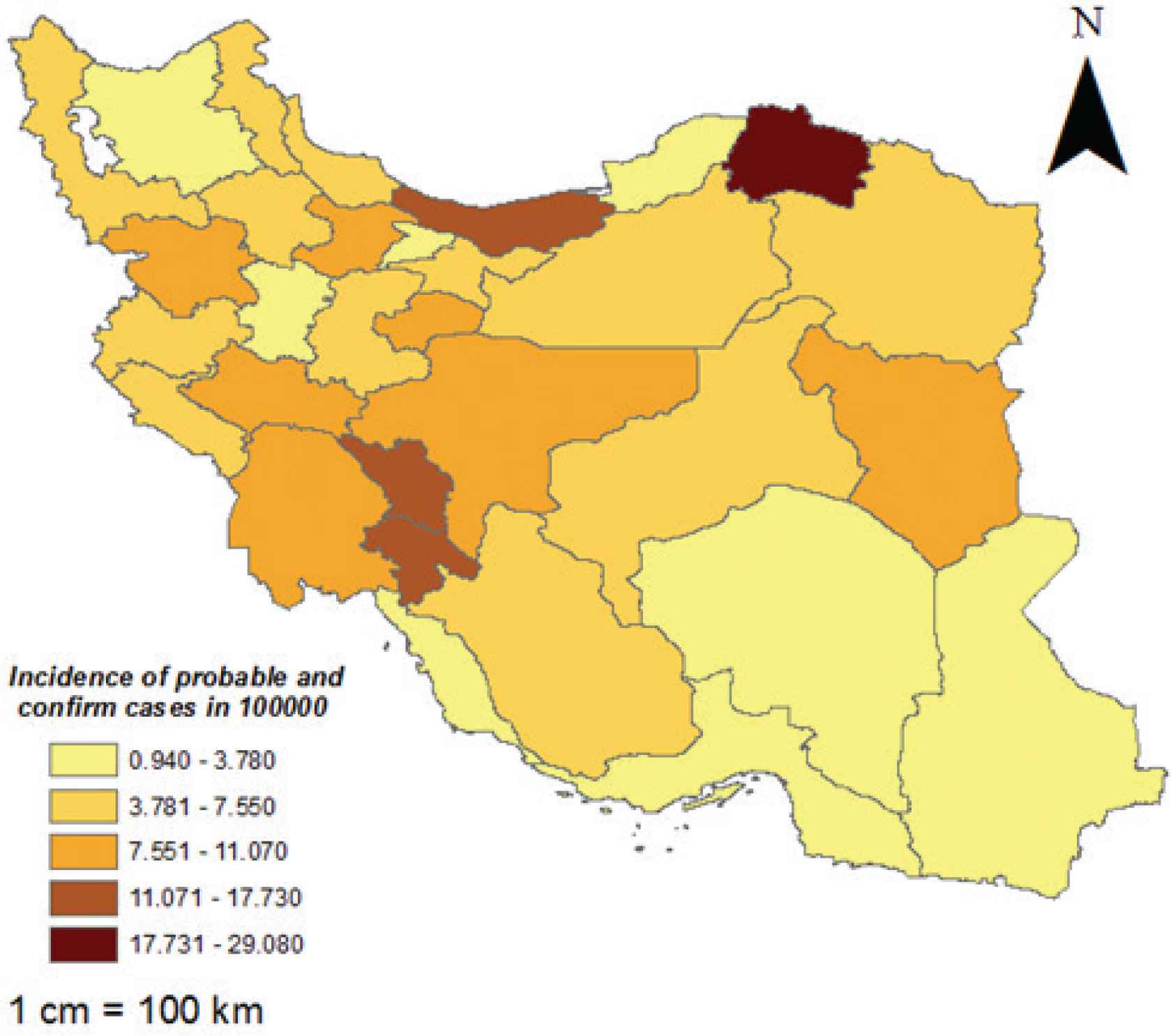
Geographical distribution of probable and confirm incidence of meningitis by incidence (in a population of 100,000) after pentavalent vaccine administration.
4. DISCUSSION
According to the results of this study in all group ages, most cases of meningitis were related to the age group of children under 5 (55.4%), which confirmed the findings of previous studies. Due to inaccurate registration of children under one, it was not possible to investigate the causes of meningitis in children due to the possibility of changing the pattern of meningitis.
The number of diagnosed meningitis by culture was deficient. In other words, the rate of meningitis with the confirmed diagnosis was 3.4%, and very few patients were diagnosed based on cerebrospinal fluid culture. The incidence of meningitis due to H. influenzae type b has decreased with the addition of the pentavalent vaccine to the national immunization program, but the meningitis caused by Streptococcal pneumonia and N. meningitis is very common in the country and it is one of the main causes of meningitis. The incidence of meningococcal has been increasing over the years of this study. Given this, the addition of pneumococcal and meningococcal vaccines to the national immunization program has a particular importance.
In studies before the addition of the pentavalent vaccine to the national immunization program and after that addition of the vaccine, the number of confirmed cases of meningitis caused by H. influenzae type b decreased by 46.2% in all age groups. This reduction was 57% in children under 5 years old, indicating the effect of the pentavalent vaccine on the population covered, especially in children under 5 years old. Also, only 4.2% of the cases with meningitis received the vaccine, and 95.8% did not.
According to a study by Lee et al. in 2008 in the United States, the results showed that the number of meningitis cases caused by H. influenza in children under 5 was reduced by 65% after the vaccine. The results of this study are consistent with the current study, which showed a 57% reduction in the number of meningitis cases [15]. Another study conducted in Uganda by Rosamond Lewis on 0- to 59-month-old children reported the efficacy of the H. influenza type b vaccine to reduce the number of meningitis cases, more than 93% [16]. Results of another study in Kenya and India also reported vaccine effectiveness of 89% and 94%, respectively [17]. Another survey by Berangi et al. in Iran also showed a decrease in the incidence of meningitis in the country, and it can be concluded that vaccination has reduced the number of meningitis cases in Iran. Also, the highest number of meningitis cases is in children under 5, which is consistent with the results of another study [1].
One of the limitations of this study is the retrospective study and utilization of surveillance system data, which has deficiencies in the data recording, including inadequate registration of patients’ age, especially in children under 2, and failure to enter information on deaths before diagnosis.
Another limitation of this study was the low number of confirmed cases of meningitis due to the failure of rapid transfer of the specimen to the laboratory and providing the culture conditions that cause only 3.4% of patients had a confirmed diagnosis and the rest of had suspects and probable diagnosis which would cause errors in the results. It should be noted that according to the Iranian Census data, the number of meningitis cases in the urban population is higher due to the higher population than the rural.
Also, the number of underreported cases in some provinces of the country indicates a severe weakness in the reporting system, which needs to strengthen the syndromic care system and increase regular training to health professionals in identifying and reporting suspected cases. Another critical issue is the lack of up-to-date information so that access to information is delayed.
Although we see a decrease in the number of cases in many provinces due to the small number of cases and geographical distribution of the confirmed cases of meningitis caused by H. influenzae (based on GIS software) the obtain results is very fragile and small variations in the number of cases cause changes in the geographical distribution.
5. CONCLUSION
Considering that the number of meningitis cases caused by H. influenzae type b has changed before and after vaccination and the number of meningitis cases has decreased after vaccine integration, so the continuation of pentavalent vaccination is necessary. Since Pneumococcal pneumonia is one of the significant causes of meningitis, adding a pneumococcal vaccine to the routine vaccination cycle of the country is also essential.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
MK has established first idea data analysis and drafted the manuscript; SH helped to design and conduct the study. All authors have had substantial contribution in data gathering, manuscript drafting, and critical revision of manuscript and data analysis.
FUNDING
The study was partially funded by Vice-chancellor for Research and Technology, Hamadan University of Medical Sciences (No. 9710186173). Funding body of this study did not play any role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
ACKNOWLEDGMENTS
The authors are going to thank the Deputy for Research and Technology of Hamadan University of Medical Sciences for supporting the present study and for administering the data with the Ministry of Health. This article is taken from the thesis of Master of Science in Epidemiology of Hamadan University of Medical Sciences (9710186173).
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
The ethical approval was obtained from the Hamadan University of Medical Sciences IR.UMSHA.REC.1397.737. This study has been conducted using aggregate data not individual one. Accordingly, there was no necessity for obtaining consent to participate.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Saber Heidari AU - Manoochehr Karami AU - Seyed Mohsen Zahraei AU - Iraj Sedighi AU - Fatemeh Azimian Zavareh PY - 2021 DA - 2021/04/03 TI - Epidemiological Profile of Meningitis following Pentavalent Vaccination in Iran: Impact of Vaccine Introduction JO - Journal of Epidemiology and Global Health SP - 310 EP - 315 VL - 11 IS - 3 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.210330.001 DO - 10.2991/jegh.k.210330.001 ID - Heidari2021 ER -