
Gender differences in bicycle exercise stress echocardiography testing
- DOI
- 10.1016/j.artres.2018.02.002How to use a DOI?
- Keywords
- Exercise testing; Stress echocardiography; Sex; Gender
- Abstract
Background: Sex-specific differences for myocardial infarction and coronary artery disease (CAD) have been reported in several studies. The aim of our present study was to identify gender-specific differences regarding bicycle-exercise-stress-echocardiography.
Methods: We compared 87 (69.0%) male and 39 (31.0%) female patients with suspected or known stable coronary artery disease (CAD), who underwent bicycle-exercise stress-echocardiography.
Results: False-positive exercise-test results were more prevalent in females (21.1% vs. 17.4%) and arterial hypertension was connected with false-positive results in women only. In males, higher peak-exercise heart-rate was accompanied by lower risk of false-positive stress-echocardiography results. Higher systolic peak blood pressure during exercise was related to a higher risk for pending coronary artery interventions in females, whereas higher peak heart-rate during exercise was accompanied by a lower risk for pending coronary artery interventions also in females.
Conclusions: Exercise-echocardiography demonstrated significant sex-specific differences. Higher efforts during stress-test lead to better test-accuracy.
- Copyright
- © 2018 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Sex-specific differences for myocardial infarction and coronary artery disease (CAD) have been reported in several studies.1–4 These differences comprise prevalence,1,2,5 age at events, cardiovascular risk factors, quality of symptoms, treatment, adverse events and prognosis.3,4 In general, women were found to outlive men and to develop fewer atherosclerotic cardiovascular events.6 In average, women are older at cardiovascular events.4,6 However, this gap in incidence gets closed with advancing age and in the elderly, cardiovascular diseases are the leading cause of death in both genders.6 CAD is the most common cause of death for American and European men and women.7,8
For CAD, several diagnostic procedures are available and in use.2 The cardio-pulmonary exercise testing is routinely performed to elicit cardiovascular abnormalities that are commonly not present at rest and is a longstanding and powerful tool used to identify suspected CAD or aggravation of CAD.2 Among the stress testing diagnostic tools, exercise echocardiography was found to be superior over exercise ECGs in terms of diagnostic accuracy and risk stratification for the future.9–11 Therefore, exercise stress echocardiography testing is the non-invasive method of choice for the assessment of CAD. It is a routine, versatile and reliable non-invasive test in patients with known or suspected CAD in both genders.9,12,13 However, in approximately 15% of the patients with suspected or known CAD, wall motion abnormalities can be detected in exercise echocardiography suggesting relevant coronary stenosis leading to myocardial ischemia under physical exercise stress, where by significant coronary stenoses could be excluded in coronary angiography (termed as a false positive stress echocardiography result).2,13 It was reported that especially the comorbidity of arterial hypertension and its treatments can lead to false positive results.13,14 Data about sex-specific differences are limited.
Thus, we aimed to investigate sex-specific differences in exercise echocardiography especially with regard to factors influencing false positive exercise echocardiography results and coronary interventional treatment.
Methods
Patients
We performed a retrospective study of patients with suspected or known stable CAD. The study protocol has been described in detail previously.13 Briefly summarized, patients were included at the Center of Cardiology, Department of Cardiology I, University Medical Centre Mainz (Germany) between January 2015 and April 2015. All patients were treated in the cardiac polyclinic (outpatient department clinic) during this timeframe and were identified with a search of the hospital information system database. Studies in Germany involving a retrospective analysis of diagnostic standard data do not require an ethics statement.
Patients were eligible for this study, if they were at least 18 years old, presented with suspected or known CAD, and were treated in the cardiac polyclinic (outpatient department clinic). Clinical reasons for performing the exercise stress echocardiography tests was a suspicion of CAD or a known CAD diagnosis with suspected aggravation due to new stenoses leading to myocardial ischemia under physical stress.
Exercise stress test protocol
The exercise stress echocardiography tests were conducted using a semi-supine bicycle ergometer with a ramp protocol, which included an increase of 25 or 50 W every 2 min. The bicycle stress echocardiography test was performed using standard techniques and endpoints according to the current guidelines.15,16 The intended and required heart rate was 80% of 220 minus age, which was utilized as the submaximal load during exercise test.13
Echocardiographical analysis
Echocardiographical images were obtained at baseline (before exercise had started) with two-dimensional transthoracic echocardiography in parasternal long axis, parasternal short axis, apical four chamber view, apical five chamber view, apical two chamber view and apical three chamber view. During exercise stages, peak- and post-exercise images focused on apical four chamber, apical five chamber, apical two chamber and apical three chamber views, which were recorded. During stress test, 12-lead ECG and blood pressure levels were assessed.15,16 Presence of angina, ST segment changes in ECG and exercise capacity were also noted.16
Experienced echocardiographers evaluated the echocardiographic images. An ischemia was defined as a stress-induced new or worsening of pre-existing wall motion abnormalities or a biphasic response.13,16,17 Inotropic reserve was defined as improvement of any wall motion abnormalities during stress testing in absence of inducible ischemia.13,17 Necrotic response was defined as akinetic or dyskinetic myocardium without thickening during stress test.13,16,17 The hypocinetic segments at rest without worsening the during stress testing were considered as a rest wall motion abnormality.17 A test was considered positive for ischemia when at least 2 adjacent segments of the same vascular territory revealed a wall motion abnormality increment.16,17 A normal test resulted if no new wall motion abnormalities occurred during stress test or even at rest in comparison with pre-examination.16,17
Study groups
Female and male patients with suspected or known stable CAD were compared in accordance to the assessed exercise echocardiography parameters.
Definitions
According to ESC guidelines,2 a relevant coronary artery stenosis was defined as causing exercise- and stress-related chest symptoms due to stenosis ≥50% in the left main coronary artery and ≥70% in one or several major coronary arteries and/or fractional flow reserve (FFR) ≤0.80.2
A false positive stress echocardiography result was defined as a positive ischemic exercise echocardiography result with a suspected relevant coronary artery stenosis and the exclusion of a relevant coronary stenosis in a subsequent coronary angiography test.13
Exaggerated blood pressure response during stress testing was defined in accordance to the ACC/AHA 2002 guideline update for exercise testing as systolic peak blood pressure values that exceed 214 mmHg during exercise testing.18
The rate-pressure product is the computed product of peak heart rate multiplied by peak systolic blood pressure during exercise.19,20
Revascularization strategies were performed according to ESC guidelines.2
Statistics
Descriptive statistics for the relevant baseline characterization of both groups are provided with means and standard deviations, medians and interquartile ranges (IQR) or corresponding frequencies, as appropriate. Continuous variables, which did not follow a normal distribution, were compared with the help of the Wilcoxon Whitney Mann U test. Normally distributed continuous variables were compared using the Student T test. Categorical variables were tested using Fisher’s exact or Chi2 test, as appropriate.
We analyzed the associations between false positive exercise echocardiography results as well as coronary interventional treatment on the one hand and several parameters on the other hand, including age, peak heart frequency and systolic peak blood pressure, exaggerated systolic peak blood pressure of >214 mmHg, percentage of patients that reached 80% of the required heart rate (220 minus age [submaximal load] during stress test), percentage of the reached heart rate related to the heart rate of computed submaximal load during stress test, peak wattage load, and rate-pressure product (>30000 mmHg/min) during exercise testing, presence of known CAD (before testing) and arterial hypertension with univariate logistic regression models in both sexes.
Receiver operating characteristic (ROC) curves with areas under the curves (AUCs) were calculated to test the effectiveness of peak heart frequency during exercise testing to predict the possibility of the false positive stress echocardiographic results and systolic peak blood pressure during exercise testing to predict a pending interventional coronary artery treatment in patients with suspected or known CAD in both genders.
The commercially available software, SPSS® (version 23; IBM; Chicago, IL, United States of America), was used for the computerized analysis. P values of <0.05 were considered to be statistically significant.
Results
In total, 126 patients with suspected or known CAD were enrolled into this study. Among these, 39 (31.0%) were of female and 87 (69.0%) of male sex. Median age of both sex-groups was similar (Table 1).
| Parameter | Female patients (n = 39) | Male patients (n = 87) | P for difference |
|---|---|---|---|
| Age | 67.0 (56.0/75.0) | 63.0 (53.0/74.0) | 0.398 |
| Patients with known coronary artery disease | 21 (53.8%) | 75 (86.2%) | <0.001 |
| One-vessel coronary artery disease | 12 (30.8%) | 22 (25.3%) | <0.001 |
| Two-vessel coronary artery disease | 6 (15.4%) | 23 (26.4%) | |
| Three-vessel coronary artery disease | 3 (7.7%) | 30 (34.5%) | |
| Arterial hypertension | 26 (68.4%) | 65 (75.6%) | 0.406 |
| Peak heart frequency during exercise (beats/min) | 134.8 ± 16.2 | 130.0 ± 16.9 | 0.170 |
| Percentage of required heart rate (220 minus age (submaximal load) during stress test) | 85.7 ± 7.7% | 83.0 ± 10.7% | 0.173 |
| Percentage of patients that reached 80% of the required heart rate (220 minus age [submaximal load] during stress test) | 33 (84.6%) | 56 (68.3%) | 0.057 |
| Peak wattage during stress test | 100.0 (75.0/100.0) Watt | 125.0 (100.0/150.0) Watt | <0.001 |
| Peak systolic blood pressure during exercise testing | 182.5 (168.3/204.3) mmHg | 185.0 (165.8/207.0) mmHg | 0.848 |
| Peak diastolic blood pressure during exercise testing | 91.5 (77.0/99.5) mmHg | 87.5 (75.0/98.0) mmHg | 0.642 |
| Difference between systolic and diastolic peak blood pressures during exercise testing | 90.5 (82.0/112.8) mmHg | 93.5 (78.8/116.3) mmHg | 0.672 |
| Patients with an exaggerated systolic blood pressure response during exercise testing (systolic peak blood pressure >214 mmHg) | 5 (13.2%) | 14 (17.1%) | 0.789 |
| Rate-pressure product >30,000 mmHg/min | 7 (18.4%) | 11 (13.4%) | 0.583 |
| Coronary angiography | 11 (28.9%) | 26 (30.2%) | 0.885 |
| Coronary artery intervention or coronary artery bypass surgery | 3 (7.9%) | 11 (12.8%) | 0.548 |
| Percutaneous transluminal coronary angioplasty (PTCA) and/or coronary stenting | 2 (5.3%) | 11 (12.8%) | 0.341 |
| Coronary artery bypass surgery | 1 (2.6%) | 0 (0.0%) | 0.306 |
| False positive stress test result | 8 (21.1%) | 15 (17.4%) | 0.625 |
Characteristics of both patient groups. P values of <0.05 were considered to be statistically significant.
As expected, males presented more frequently with known CAD, a more severe known CAD status and were more likely to have more than one coronary vessel diseased (Table 1).
In males, 29 (33.3%) positive stress echocardiography results were counted. Among these patients, 26 (90.0%) underwent cardiac catheter with coronary angiography and in 11 (12.8%) an interventional coronary artery treatment due to relevant/high-grade coronary artery stenosis was performed.
In total, 14 (35.9%) females revealed a positive stress test results. In these, 11 (78.6%) women underwent cardiac catheter with coronary angiography and 3 (7.9%) females were treated by interventional coronary artery treatment due to relevant/high-grade coronary artery stenosis.
Overall, 8 (21.1%) female and 15 (17.4%) male patients had a false positive exercise test result (see the flow chart in Fig. 1).
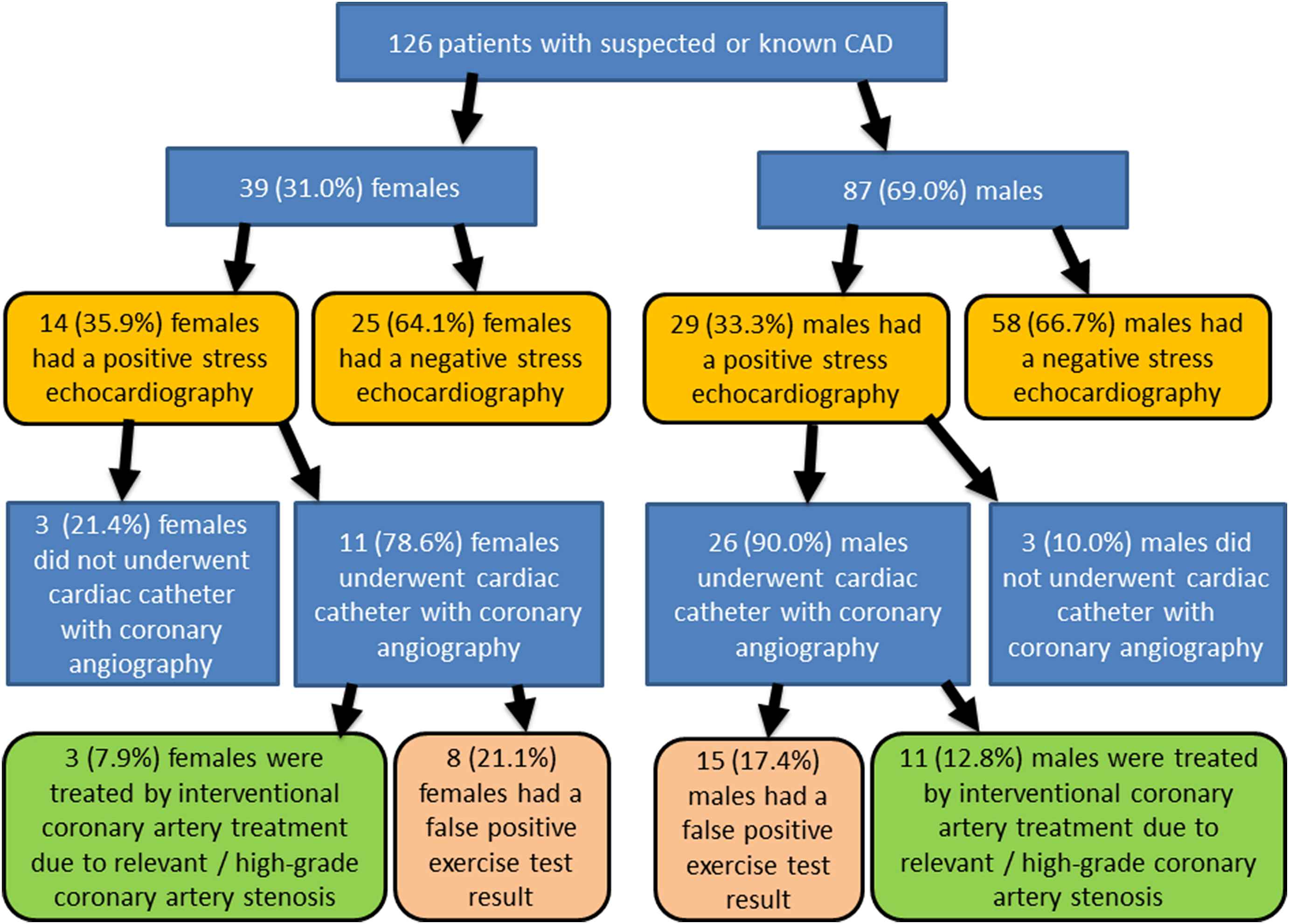
Study flow chart.
While the peak wattage during exercise test was higher in men, women reached more often 80% of the intended and required submaximal load (80% of heart rate 220 minus age) (Table 1). Interestingly, neither in relation to the comorbidity of arterial hypertension, nor in false positive exercise test results or interventional coronary artery treatments a significant difference between both genders could be detected.
We analyzed predictors of a false positive exercise echocardiography with uni-variate regression models sex-specifically (Table 2). In males, a higher peak load during exercise test with higher peak heart frequency and higher percentage of heart frequency according to the intended submaximal load as well reaching 80% of the intended submaximal load, were all accompanied by a lower risk of false positive stress echocardiography results in contrast to females. Reaching 80% of the intended submaximal load during exercise, reduced the risk for a false positive stress echocardiography result by 81% in males.
| Gender | Females (n = 39; 8 patients (21.1%) with false positive exercise test) | Males (n = 87; 15 patients (17.4%) with false positive exercise test) | ||
|---|---|---|---|---|
| Odds Ratio (CI 95%) | P-value | Odds Ratio (CI 95%) | P-value | |
| Age (per 10 years) | 1.03 (0.55–1.92) | 0.935 | 0.78 (0.46–1.30) | 0.337 |
| Systolic peak blood pressure during exercise testing (per 10 mmHg) | 1.04 (0.79–1.36) | 0.775 | 0.92 (0.75–1.15) | 0.473 |
| Exaggerated systolic peak blood pressure of >214 mmHg | Regression model was not calculable, therefore Chi–Square Test was used for calculation | 0.564 | 0.76 (0.15–3.87) | 0.745 |
| Peak heart frequency during exercise testing (per 10 beats/min) | 1.17 (0.71–1.95) | 0.542 | 0.70 (0.49–1.01) | 0.055 |
| Percentage of patients that reached 80% of the required heart rate (220 minus age [submaximal load] during stress test) | Regression model was not calculable, therefore Chi–Square Test was used for calculation | 0.563 | 0.19 (0.06–0.64) | 0.008 |
| Percentage of required heart rate (220 minus age (submaximal load) during stress test) | 1.09 (0.96–1.24) | 0.164 | 0.92 (0.86–0.99) | 0.021 |
| Rate-pressure product (per 1000 mmHg/min) | 1.05 (0.89–1.23) | 0.588 | 0.90 (0.80–1.02) | 0.101 |
| Rate-pressure product >30000 mmHg/min | 0.55 (0.06–5.35) | 0.605 | 0.44 (0.05–3.73) | 0.451 |
| Peak wattage during stress test | 0.97 (0.94–1.01) | 0.136 | 0.99 (0.97–1.01) | 0.169 |
| Coronary artery disease | 0.46 (0.09–2.28) | 0.341 | 1.07 (0.21–5.45) | 0.939 |
| Arterial Hypertension | Regression model was not calculable, therefore Chi–Square Test was used for calculation | 0.039 | 0.18 (0.02–1.48) | 0.111 |
Univariate logistic regression model for the association between several parameters and a false positive exercise echocardiography result. P values of <0.05 were considered to be statistically significant.
Arterial hypertension was connected with a false positive exercise echocardiography result in women only, but not in men (Table 2).
While no investigated parameters were predictive for coronary artery intervention in men, peak heart frequency and systolic peak blood pressure during exercise were predictive for necessary coronary artery intervention in women (Table 3), whereby the number of interventional treatments in the female subgroup was low.
| Gender | Females (n = 39; 3 (7.9%) patients had a coronary artery intervention or coronary artery bypass surgery) | Males (n = 87; 11 (12.8%) patients had a coronary artery intervention or coronary artery bypass surgery) | ||
|---|---|---|---|---|
| Odds Ratio (CI 95%) | P-value | Odds Ratio (CI 95%) | P-value | |
| Age (per 10 years) | 1.17 (0.43–3.14) | 0.762 | 1.43 (0.82–2.51) | 0.212 |
| Systolic peak blood pressure during exercise testing (per 10 mmHg) | 1.60 (1.01–2.54) | 0.045 | 0.98 (0.77–1.24) | 0.873 |
| Exaggerated systolic peak blood pressure of >214 mmHg | 20.67 (1.42–300.54) | 0.027 | 0.44 (0.05–3.73) | 0.451 |
| Peak heart frequency during exercise testing (per 10 beats/min) | 0.28 (0.08–0.96) | 0.043 | 1.08 (0.74–1.57) | 0.708 |
| Percentage of patients that reached 80% of the required heart rate (220 minus age [submaximal load] during stress test) | 0.05 (0.00–0.68) | 0.025 | 0.51 (0.14–1.87) | 0.313 |
| Percentage of required heart rate (220 minus age (submaximal load) during stress test) | 0.75 0.59–0.97) | 0.025 | 1.03 (0.98–1.09) | 0.267 |
| Rate-pressure product (per 1000 mmHg/min) | 1.02 (0.81–1.30) | 0.848 | 1.05 (0.89–1.14) | 0.938 |
| Rate-pressure product >30000 mmHg/min | 2.33 (0.18–30.10) | 0.516 | 1.51 (0.28–8.12) | 0.634 |
| Peak wattage during stress test | 1.00 (0.95–1.04) | 0.887 | 0.99 (0.97–1.01) | 0.463 |
| Coronary artery disease | Regression model was not calculable, therefore Chi–Square Test was used for calculation | 0.232 | 1.72 (0.20–14.80) | 0.622 |
| Arterial Hypertension | Regression model was not calculable, therefore Chi–Square Test was used for calculation | 0.538 | 1.53 (0.30–7.70) | 0.608 |
Univariate logistic regression model for the association between several parameters and a pending coronary interventional treatment (coronary artery intervention or coronary artery bypass surgery). P values of <0.05 were considered to be statistically significant.
Remarkably, a high systolic peak pressure during exercise was associated with an elevated risk for pending coronary artery interventions in women. A 10 mmHg higher systolic peak pressure during exercise was related to a 60% increased risk for pending coronary artery interventions in females. In contrast, 10 beats/min higher peak heart frequency during exercise was accompanied by 72% lower risk for a pending coronary artery intervention in females. If female patients, reached 80% of the intended submaximal load during exercise, the risk for pending coronary artery interventions was distinctly reduced compared with those female patients, who did not achieve this intended heart rate threshold (Table 3).
The ROC analyses for heart rate to predict false positive exercise echocardiography results showed in both genders only poor efficiency results. The AUCs were with 0.56 in females and 0.64 in males not promising (Fig. 2). In contrast, the ROC curve for peak systolic blood pressure to predict a pending coronary artery intervention treatment in females showed with an AUC of 0.80 a good performance, while it failed in men to be levantly predictive (AUC 0.46) (Fig. 3).
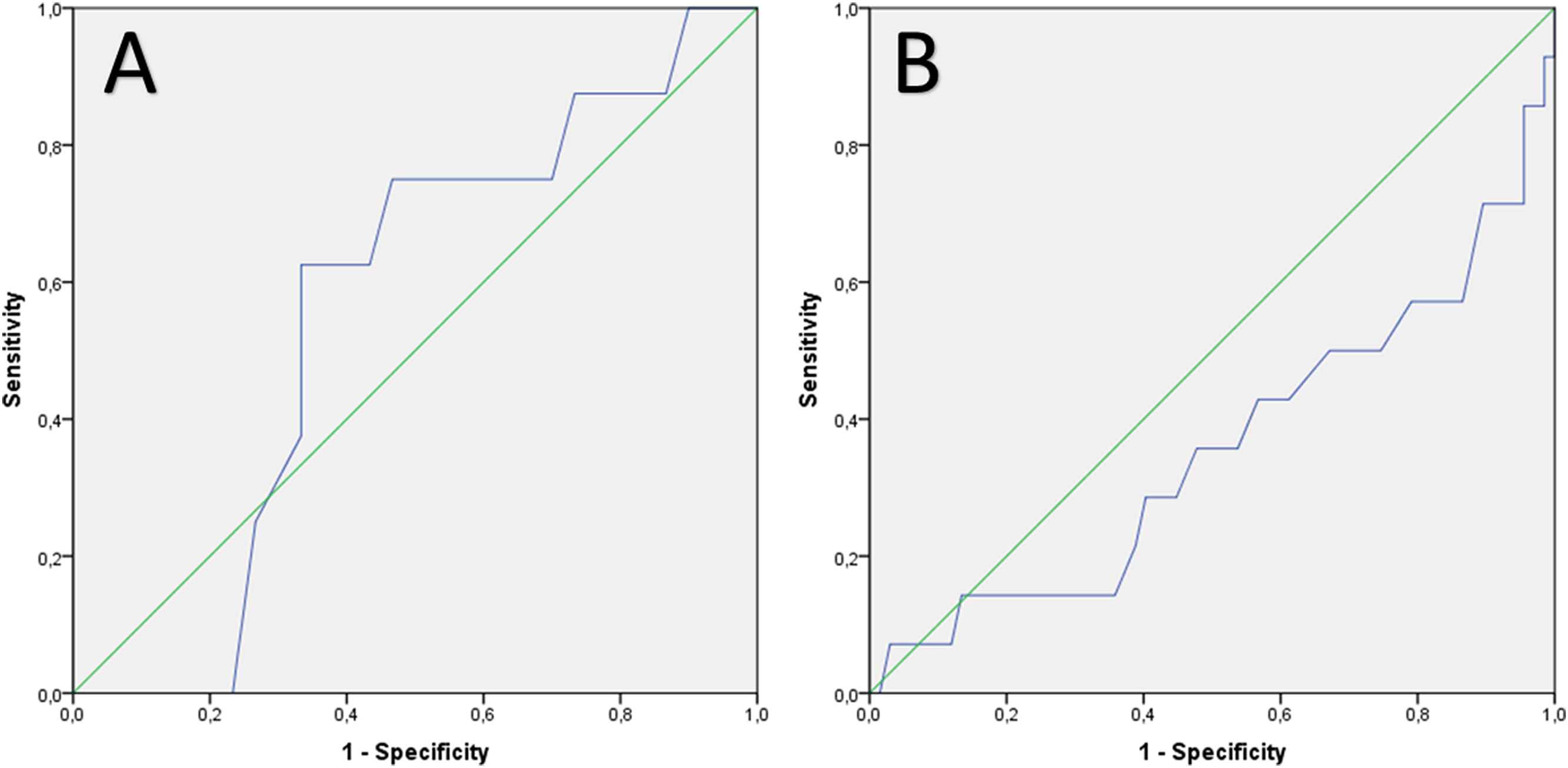
ROC analysis for prediction of false positive exercise echocardiography result using the peak heart frequency during exercise testing in (A) females (AUC 0.56) and (B) males (AUC 0.64).
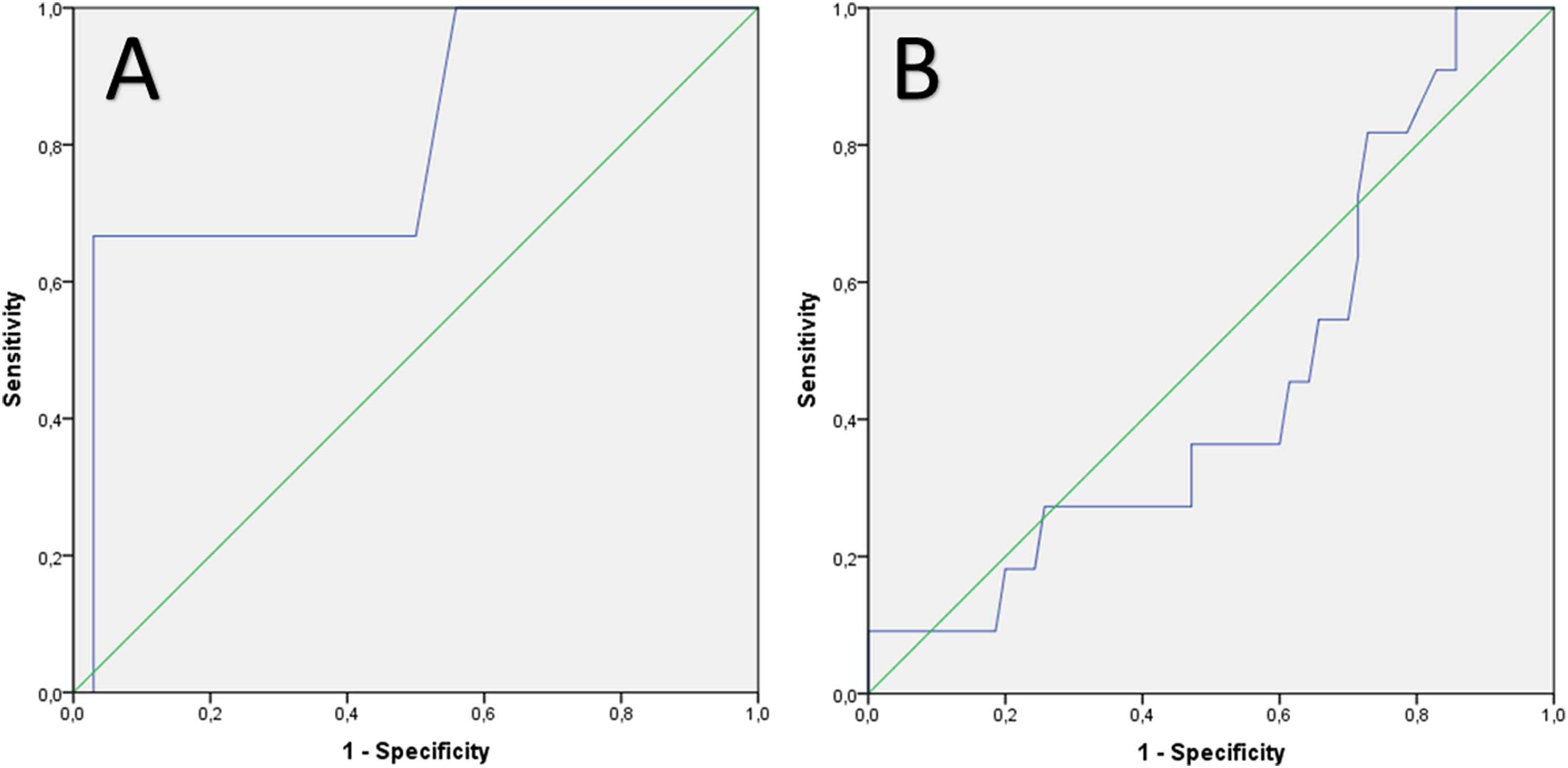
ROC analysis for prediction of pending interventional coronary artery treatment using systolic peak blood pressure during exercise testing in (A) females (AUC 0.80) and (B) males (AUC 0.46).
Discussion
Ischemic heart disease is the most common cause of death in American and European males and females.7,8 Sex-specific differences in CAD and it’s acute presentations myocardial infarction and acute coronary syndrome are well known and comprising prevalence,1,2,5,6age at events, cardiovascular risk factors, typical symptoms, treatment and outcome.3,4 Female CAD patients experience more often treatment delays and receive less often aggressive therapy.21,22 In addition, studies indicate that women undergo less frequently diagnostic tests inclusively exercise echocardiography,22,23 which may explain the delay in making the diagnosis and performing adequate treatment.21
In detection of CAD, exercise echocardiography is a powerful diagnostic tool to identify patients with significant CAD.10,16,24,25 In patients with CAD, it plays a crucial role in the initial detection of CAD, in determining prognosis and in therapeutic decision making.9,10,16,24,25 Stress echocardiography was shown to have good prognostic value in patients with suspected or known CAD.7,9,10 Presence of ischemia in stress echocardiography was an independent predictor of death7,10,11,16,17 and contrary a normal exercise echocardiogram was connected with a low mortality risk.11,16,17 However, in approximately 15% of all patients with suspected or known CAD, stress echocardiography will lead to false positive stress echocardiography results.2,13
Although the use of exercise echocardiography has increased exponentially worldwide,23 this testing tool has only been validated in studies dominated by male patients and data about sex-specific differences are limited.23 It is hypothetically if the current diagnostic paradigm is primary suitable for men, but may not be appropriate for all women.21
Thus, we aimed to investigate sex-specific differences in exercise echocardiography especially with regard to factors of false positive exercise echocardiography results and coronary interventional treatment.
The main findings of our study can summarized as followed:
- I.
As expected, men could reach on average a higher peak load during exercise test.
- II.
Higher efforts with more than 80% of the computed submaximal load heart frequency reduced the risk of false positive exercise echocardiography results in males, but not in females.
- III.
Although females did not present more often with arterial hypertension, the presence of arterial hypertension was accompanied by false positive exercise echocardiography results in women only.
- IV.
High systolic peak blood pressure values during stress testing go along with higher risk of pending coronary artery interventions in females, whereas higher peak heart frequency during exercise was associated with a lower risk for coronary artery interventions in women, but not in men.
As expected, men could achieve higher peak load (wattage) during exercise. It is well established that in general women revealed lower levels of physical activity,21 muscle mass, power and strength,26 therefore a higher peak load in men does not surprise in comparison to women.
As previously hypothesized by others,21 current diagnostic approaches for CAD regarding exercise echocardiography demonstrated significant sex-specific differences highlighted by this present study.
Contrary to other studies,27 the number of patients with a false positive exercise echocardiography results was not significantly different between both genders, but in accordance with prior study results,27 our study results showed that arterial hypertension was more relevant for false positive exercise echocardiography results in women than in men.
Men showed accelerated efforts during exercise compared to women, leading to a reduced risk of false positive exercise echocardiography results. These findings are partly in accordance with other studies,28 which indicate that higher peak heart rate is accompanied by higher accuracy of the exercise test.28
Interestingly, higher systolic peak pressure response during exercise test was associated with a pending coronary artery interventions in women, but not in men. Other studies reported in accordance with our findings, that an abnormal systolic blood pressure response during physical exercise recovery in patients with angina pectoris was indicative of severe myocardial ischemia.29
In addition, reaching a higher peak heart frequency during exercise was connected with a reduced risk for coronary artery intervention in women, but not in men.
The rate-pressure product failed to predict a pending coronary artery intervention in patients with suspected and known CAD, in discordance to other studies.19,20
Our findings indicate in accordance with other studies21,23,28 for significant sex-specific differences in the exercise echocardiographic approach to identify CAD in both sexes. The results highlighted that a higher effort during stress test (seen in a higher peak heart rate) is accompanied by better test accuracy, but interestingly for men to avoid false positive stress test results and in women to recognize ischemia during exercise testing caused by relevant coronary stenosis more precisely. Presence of arterial hypertension has a larger influence on exercise testing in females, causing potentially false positive stress test results compared to males. The efficiencies of the investigated markers to predict a false positive exercise test result and a subsequent coronary artery intervention were all weak (small AUCs), exclusively for peak systolic blood pressure to predict pending coronary artery intervention treatment in females with an AUC of >0.8.
Differences in exercise echocardiography to identify CAD in women and men, were in part already described in other studies.23 Roger et al.23 reported that the sensitivity and the positive predictive value for exercise echocardiography to identify CAD were higher in men than in women, whereas the specificity was similar between both genders.23
These sex-specific differences have to be kept in mind, when interpreting exercise echocardiography results.
Conclusions
This study demonstrated sex-specific differences in exercise echocardiography. Men could reach a higher peak load during exercise test. Higher efforts during exercise reduced the risk of false positive exercise echocardiography results in males, but not in females. Although females did not present more often with arterial hypertension, presence of arterial hypertension was accompanied with false positive exercise echocardiography results in women only. High systolic peak blood pressure values during exercise go along with higher risk of pending coronary artery interventions in females, whereas reaching higher peak heart frequency during exercise were associated with a lower risk for pending coronary artery interventions in women, but not in men.
Limitation
The primary limitations of the study are the small number of included patients, the single-center and retrospective study design. Regarding the small size of the study, firm conclusions are difficult to be drawn. Another limitation is that we did not quantitatively assess the stress echocardiographic results. They were only assessed semi-quantitatively with a visual assessment. This approach is still the routine stress echocardiography imaging interpretation today. Therefore, the quality of assessment of regional wall motion abnormalities during the stress test is subjective and dependent on the interpreter.30 Additionally, echocardiographers were not blinded to the preexisting CAD status. As in every echocardiographic imaging method, patient-dependent factors, such as obesity or lung diseases, can limit the quality of stress echocardiography results, and can make it harder for the interpreter to evaluate the stress test result.16
Funding
This study was supported by the German
Disclosures
The authors declare no conflicts of interest.
Appendix A
Supplementary data
Supplementary data related to this article can be found at
References
Cite this article
TY - JOUR AU - Karsten Keller AU - Kathrin Stelzer AU - Martin Geyer AU - Thomas Münzel AU - Mir Abolfazl Ostad PY - 2018 DA - 2018/02/21 TI - Gender differences in bicycle exercise stress echocardiography testing JO - Artery Research SP - 8 EP - 16 VL - 22 IS - C SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2018.02.002 DO - 10.1016/j.artres.2018.02.002 ID - Keller2018 ER -