
Brachial flow-mediated dilatation response to acute different upper body training postures in lean inactive vs. lean active men
Fax: +662 649 5000x22502.
- DOI
- 10.1016/j.artres.2018.01.003How to use a DOI?
- Keywords
- Bench press; Endothelial function; Flow-mediated dilatation; Lat pull down; Resistance training
- Abstract
Background: Resistance training postures trigger different results on endothelial function: however, the acute effect of resistance training on upper body muscle in active and inactive persons is inconclusive. The present study aimed to investigate the acute effects of 2 different types of upper body training (bench press training and lat pull down training) on flow-mediated dilation (FMD), and to compare the effects between lean inactive men (LI) and lean active men (LA).
Methods: LI (n = 16) and LA (n = 16) men undertook 2 upper body training postures at 60% of 1 repetition maximum (RM), 15 repetitions a set for 3 sets. Before and after immediate training, the biological data, FMD data, and blood pressure data were collected.
Results: Both the LI and LA groups showed similar results at the baseline of biological data, including carotid intima media thickness data (P > 0.05), while the higher muscular strength was observed in the LA group. Significantly higher shear rate and blood pressure after training were observed in both groups (P < 0.05); however the magnitude of increment in blood pressure was greater in LI group. FMD was significantly increased in the LA group following bench press training while it decreased in the LI group following lat pull down training (P < 0.05).
Conclusion: Higher fitness status can acutely protect against the undesirable effects on vascular function following resistance training. In active persons, we suggest performing both the bench press and lat pull down trainings, without any limitations. In contrast for inactive persons, the bench press is recommended at the beginning of training for protection against decreased FMD. After vascular adaptation, lat pull down training might be added in order to strengthen upper body muscles.
- Copyright
- © 2018 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Endothelial cells are simple squamous monolayer cells that line the inside of the lumen of blood vessels in a mosaic pattern. These cells have a crucial responsibility for maintaining vascular homeostasis, especially, the balance of vasodilators and vasoconstrictors.1 Thus, any imbalance can lead to endothelial dysfunction which can cause the development of cardiovascular diseases, i.e., atherosclerosis, coronary artery disease, and arterial hypertension.2,3 To enhance endothelial function, several strategies have been recommended, including antihypertensive therapy, cholesterol decreasing drugs, exercise training, and other methods involving the reduction of cardiovascular risk factors. Specifically, exercise training that affects vascular function has been widely investigated for improving the deterioration of endothelial function.
The most common method for evaluating endothelial function in exercise training is by flow-mediated dilatation (FMD), which is a non-invasive method that represents the change of diameter via the activation of blood flow.4–6 Higher FMD in humans is related with lower vascular risk and stage of hypertension.7 Aerobic exercise has shown an increment of FMD in both acute and chronic effects in active subjects.8,9 In contrast, some studies have reported conflicting results concerning the acute effects in sedentary subjects.8 It is possible that the variation of the baseline of vascular risk factors and health status in individuals might be an important factor associated with the change of FMD.
The acute effects of FMD following resistance training were inconclusive, especially when researchers focused on different training postures.10,11 Our previous studies reported the acute effects of different abdominal types of training on FMD in untrained sedentary subjects.10,11 We found that FMD was acutely improved after 3 sets of crunch training, with no change in side-crunch training and plank 30 s training, and a decrease in both leg raise and plank 60 s training. These results encourage the inactive subjects to select proper postures that might not impair FMD at the beginning of training. Nonetheless, there is no concrete evidence regarding the acute effects of resistance training on other body regions, especially the upper body region. The purpose of this study was to investigate the acute effects of the different types of upper body training (bench press training and lat pull down training) on FMD. These effects were compared between lean inactive and lean active male subjects. Our working hypothesis was that the different upper training postures would yield variable results in both exercise status groups.
Methods
Participants
Thirty-two lean young male subjects, active (n = 16) and inactive (n = 16), were recruited from Srinakhariwirot University, Nakhon Nayok, Thailand. The lean inactive (LI) group was characterized by no exercise training in the past 6 months. The lean active (LA) group had experience in resistance training program for a minimum of 3 times per week for at least 6 months, but no aerobic training program, or an aerobic program but of less than 1 time per week. All participants were aged between 18 and 22 years, with a body mass index (BMI) of 18.5–24.9 kg/m2, were nonsmokers, and free from known cardiovascular diseases. The study was approved by the Ethics Committee of Srinakharinwirot University, Thailand and written consent was obtained from all participants.
Exercise intervention
Participants performed bench press training on a Smith machine (Smith machine FW-161, Johnson Health Tech Co., Ltd) and standard lat pull down training on a cable system (Johnson SU-152, Johnson Health Tech Co., Ltd). For bench press training, participants started in the supine position on the bench, gripping the bar, then lowered the bar to their chest at nipple level. Participants began the first repetition by pushing the bar until they achieved full elbow extension, and then lowered the bar to the starting position. The distance between both hand grips was calculated by 165% biacromial breadth (the distance between acromion processes × 1.65). For lat pull down training, participants started in a seated position on the bench with their thighs attached to the machine. They used a pronated grip on the bar. Participants began the first repetition by pulling the bar downward to chin level, and then slightly extended their elbows and shoulders until fully extended to the starting position. The distance between both hand grips was equal to the distance of the outside of the distal end of the metacarpal to the seventh cervical vertebra.
In both the bench press and lat pull down trainings, participants were instructed to perform 2 s for the concentric phase and 2 s for the eccentric phase which was controlled by a metronome. Each type of training involved training at 60% of 1 repetition maximum (RM), 15 repetitions a set for 3 sets, with 1 min to rest between each set.
Study design
Both the LA and LI groups undertook two upper body training postures, the bench press and lat pull down, using weight machines. Training session was separated by at least 72 h. Twenty-four hours prior to each session, the participants were asked to refrain from vigorous physical activities and caffeine. At the first training session, both the LA and LI groups performed two trials in a randomized order, either the bench press or lat pull down training. The remaining upper body training posture was undertaken by participants at the second training session. Participants in both groups were instructed about the training and permitted to practice a week prior to their first session. At each training session, all the participants had their biological data, blood pressure data, FMD data, and intima media thickness (IMT) of the common carotid artery data measured. After the completion of training, all of the above biological data were repeated immediately.
Measurements
Body weight and body fat were measured using a body composition analyser (Omron BF511, Omron Healthcare Europe B. V., Hoofddorp, Netherlands). Participants were asked to rest in the supine position for 10 min. Then blood pressure and heart rate were measured using a semi-automated blood pressure device (Carescape V100, GE Dinamap, USA). Maximal strength was performed with a Smith machine and lat pull down cable system using the one-repetition maximum (1RM) method.
FMD was determined using a portable ultrasound (Vivid i-GE Healthcare, Cardiovascular Ultrasound System; GE Medical Systems, Tirat Carmel, Israel). All participants rested in the supine position for 20 min and blood pressure cuff was placed around the right forearm. Throughout the experiment, the brachial artery was imaged longitudinally above the antecubital fossa. Baseline of brachial artery data was monitored for 1 min and then the cuff was inflated immediately to 50 mmHg above systolic blood pressure. The inflation was maintained for 5 min and then deflated for 5 min.12 B-mode was used to record brachial artery diameter while pulsed-waved Doppler mode was used to measure mean blood velocity. Ultrasound images were transferred to the edge detection software (Brachial Analyzer, Medical imaging applications, USA) to analyse offline arterial distension data. Shear rate was calculated by mean blood velocity/artery diameter.13 FMD was calculated using the equation FMD = (Maximal post occlusion brachial diameter − baseline brachial diameter) x 100/baseline brachial diameter.14
IMT of the common carotid artery, the range from the lumen-intimal interface to the medial-adventitial border, was determined by ultrasound. Participants in supine position were investigated on the right IMT of the carotid artery. B-mode images were stored and transferred to digital viewing software (Carotid Analyzer, Medical imaging applications, Coralville, IA, USA).15 During the collecting and evaluating FMD and IMT data, the operator was blinded to the fitness status of participants.
Statistical analyses
The data are shown as mean ± standard deviation. Differences between the lean active and lean inactive groups on biological data at baseline of participant characteristics were tested using independent t tests. Blood pressure, shear rate, and flow-mediated dilatation data were analyzed using repeated-measures ANOVA followed by LSD’s multiple comparison (group × intervention). The calculations of change scores were to compare the magnitude of changes following each resistance postures. Associations were examined by correlational and regressional analyses. Values of P < 0.05 were considered to be statistically significant.
To detect a 2% change in the FMD difference, each four conditions (LI and LA performed bench press and lat pull down training) requires 10 participants.16,17 A statistical power of 80% is consistent with 2% of the change in standard deviation.18 Consequently, sixteen participants were recruited in each conditions.
Results
The biological data at baseline of participant characteristics are shown in Table 1. Both the lean active and lean inactive groups showed similar results in number, age, height, body mass, body mass index, body fat, heart rate at rest, systolic blood pressure, diastolic blood pressure, mean arterial pressure, flow-mediated dilatation, and carotid artery intima media thickness. However, significantly lower muscular strength in both types of training (bench press and lat pull down) was observed in the LI group compared with the LA group (P < 0.05).
| Lean active | Lean inactive | |
|---|---|---|
| Number (n) | 16 | 16 |
| Age (y) | 18.6 ± 0.7 | 18.5 ± 0.8 |
| Height (cm) | 176 ± 3.7 | 175 ± 3.6 |
| Body mass (kg) | 73.2 ± 5.4 | 72.4 ± 3.5 |
| Body mass index (kg/m2) | 23.4 ± 1.0 | 23.6 ± 0.8 |
| Body fat (%) | 17.6 ± 1.1 | 18.4 ± 1.0 |
| Heart rate at rest | 68.6 ± 5.0 | 67.1 ± 3.8 |
| Systolic blood pressure (mmHg) | 128.6 ± 10.2 | 125.0 ± 10.1 |
| Diastolic blood pressure (mmHg) | 67.5 ± 6.2 | 74.0 ± 9.3 |
| Mean arterial pressure (mmHg) | 87.9 ± 6.7 | 91.0 ± 8.4 |
| Flow-mediated dilatation (%) | 14.4 ± 2.7 | 13.6 ± 3.6 |
| Carotid intima media thickness (mm) | 0.57 ± 0.01 | 0.58 ± 0.01 |
| Bench press muscular strength (kg) | 91.8 ± 16.5 | 43.8 ± 5.2* |
| Lat pull down muscular strength (kg) | 77.3 ± 10.4 | 37.5 ± 2.1* |
Data are mean ± SD.
P < 0.05 vs. Lean active.
Biological data at baseline of participant characteristics.
Figure 1 demonstrates significantly higher systolic blood pressure after lat pull down training, which was unchanged after bench press training in both the LA and LI groups (P < 0.05). Only in the LI group, diastolic and mean arterial blood pressure were significantly greater after bench press and lat pull down trainings (P < 0.05), and the change in mean arterial pressure in the LI group after lat pull down training was higher than after bench press training (P < 0.05).
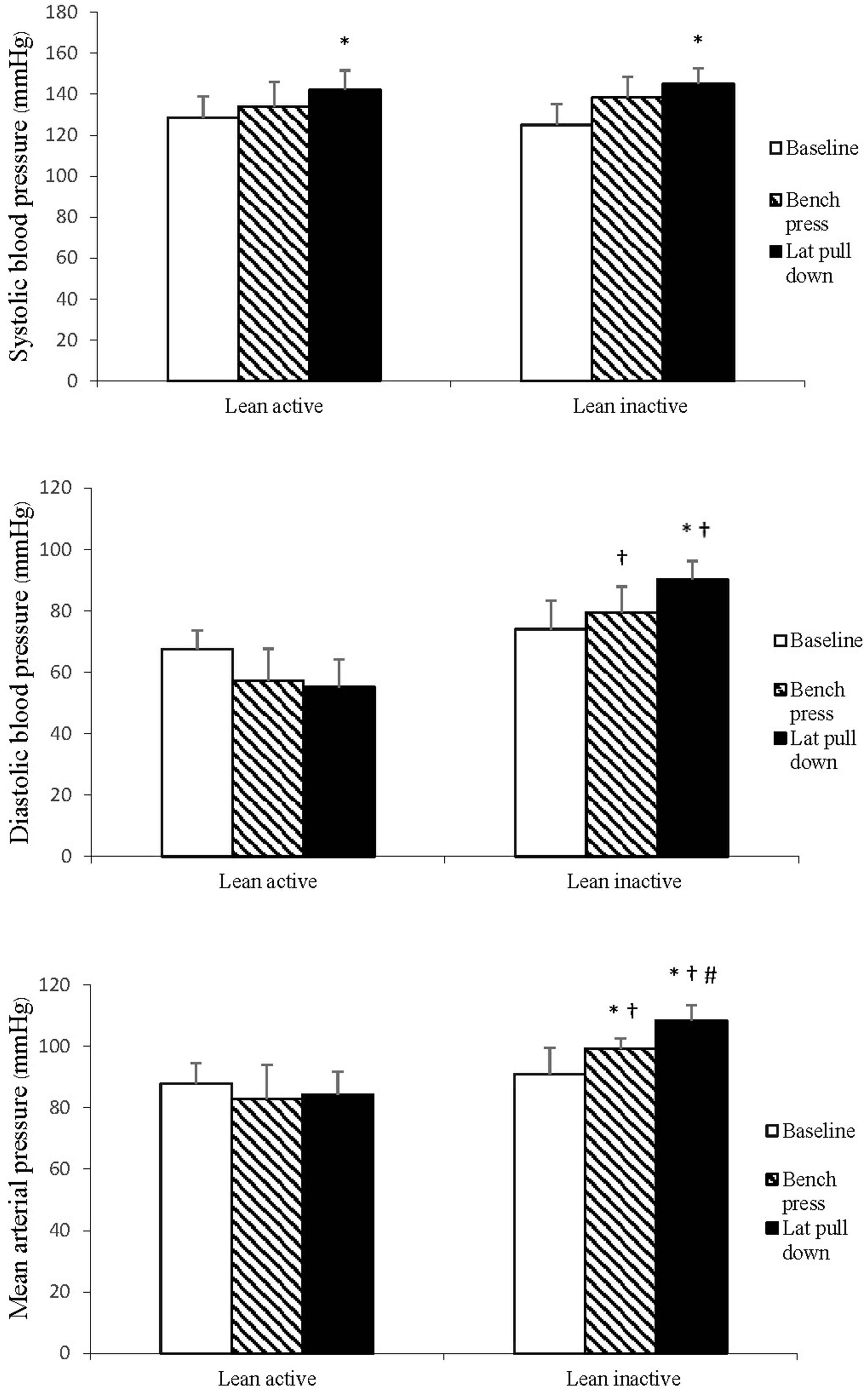
Blood pressures. *P < 0.05 vs. Baseline, †P < 0.05 vs. Lean active at the same training posture, #P < 0.05 vs. Bench press.
Shear rate data are demonstrated in Fig. 2. There was a significant increase in the shear rate in both the LA and LI groups after bench press and lat pull down trainings.
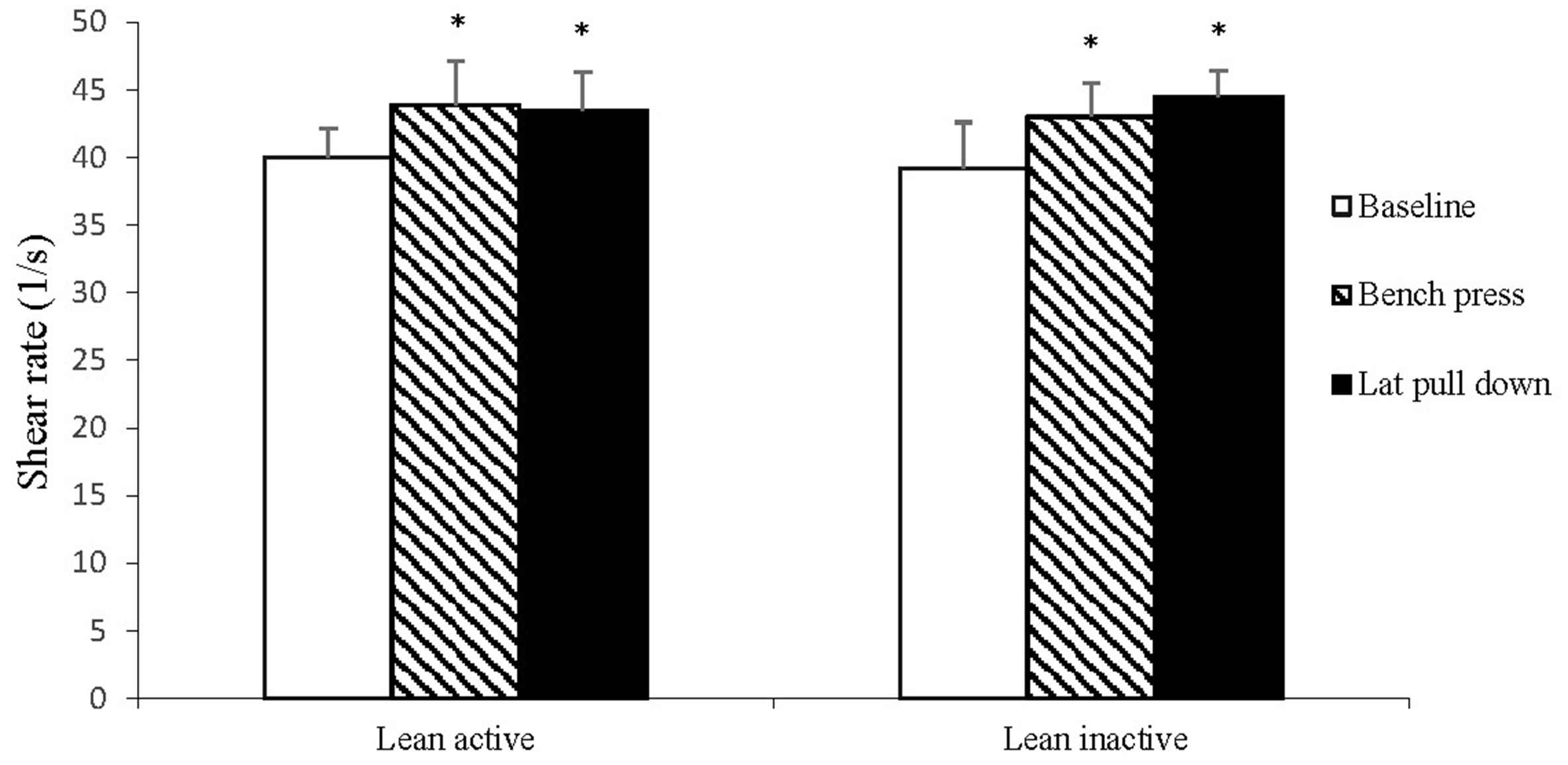
Shear rate. *P < 0.05 vs. Baseline.
The changes in FMD are shown in Fig. 3. FMD was significantly higher in the LA group after bench press training (P < 0.05), and showed no change in the LI group. However, a significant decrease in FMD was observed only in the LI group following lat pull down training (P < 0.05).
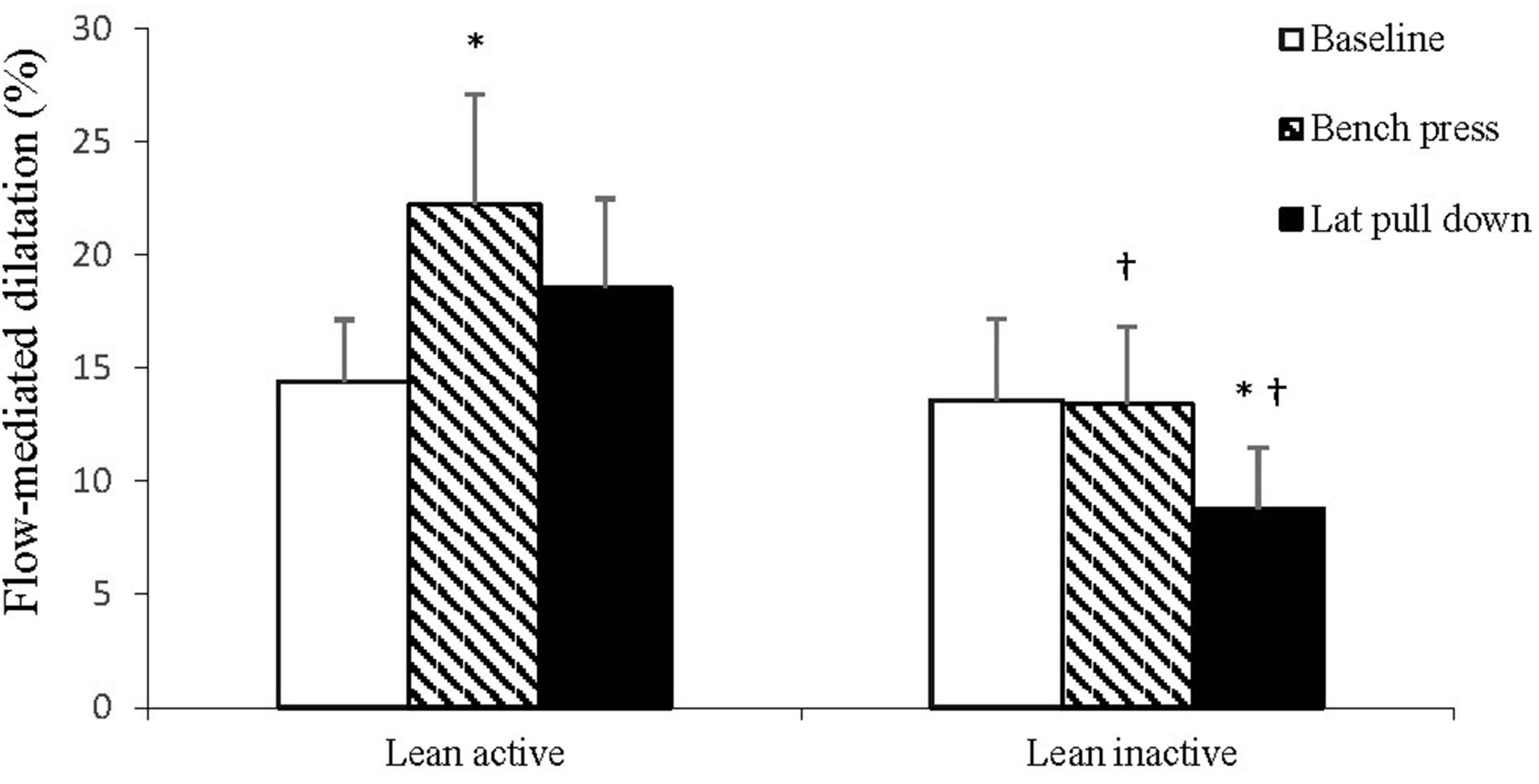
Flow-mediated dilatation (FMD). *P < 0.05 vs. Baseline, †P < 0.05 vs. Lean active at the same training posture.
The changes of diastolic blood pressure, pulse pressure (systolic–diastolic blood pressure) and mean arterial pressure were significantly correlate with the changes of FMD (r = −0.67, 0.60, −0.70 respectively) only in the LI group that performed lat pull down.
Discussion
The major findings of this study were that lat pull down training acutely induced the impairment of FMD in the LI group, whereas the result was unchanged in the LA group. Increased FMD following bench press training was observed only in the LA group. Our findings encourage bench press training for preventing the undesirable effects of vascular impairment and to strengthen the upper body muscles in both the active and inactive subjects.
Resistance training with the lat pull-down cable, generates muscle activity mainly in the latissimus dorsi, pectoralis major, posterior deltoid, long head of the triceps, and teres major,19 while bench press training using a weight machine is associated with muscle activation on the pectoralis major, anterior and medial deltoid, and triceps brachii.20 Considering the muscle activation which strengthens various parts of the upper body, both training postures were selected for this study. Lat pull down and bench press training demonstrated a significant, acute increase in systolic and mean arterial blood pressure in both the LA and LI groups. This result is similar to our previous studies in which plank, crunch, side crunch, and leg raise training were performed.10,11 Interestingly, the LI group showed significantly higher mean arterial pressure after performing lat pull down training compared with the LA group. This finding leads us to believe that the different fitness status of subjects might trigger the different changes in blood pressure.
FMD has emerged as a non-invasive procedure for evaluating vascular function in which higher FMD is related to lower vascular risk.7 The result from our previous studies emphasized the selection of training postures that did not trigger the negative effects on FMD at the beginning of the training period in inactive persons.10,11 It is a matter of fact that obesity is considered an independent risk factor for atherosclerosis and coronary heart disease21; thus we decided to recruit only lean and non-diabetic subjects into our study in order to eliminate this confounder bias. We would like to know the FMD results among the active and inactive subjects following two upper body training postures. The crucial result revealed that lat pull down training impaired FMD in inactive subjects but did not show any impairment in active subjects. In addition, bench press training brought about the enhancement of FMD only in active subjects. This result concurs with a previous study which found that FMD is improved in overweight active men and decreased in overweigh inactive men.8 Even though our study was performed on lean inactive and lean active subjects, there was no significant difference in the baseline value of carotid intima media thickness, markers for atherosclerotic development, and risk factors for cardiovascular disease.15 This could explain why higher fitness status can protect against the unfavorable effects on FMD.
The changes of FMD in this study may be elucidated through two main pathways: shear rate and blood pressure. Normally, exercise induces increased blood flow to the active muscles and activates nitric oxide release through an increased shear rate.22,23 The higher level of nitric oxide stimulates the enhancement of FMD after immediate exercise.24 Our results show an increment of shear rate in both the inactive and active groups after performing two training interventions; however, improved FMD was observed in only the active group after bench press training. Birk et al.18 have demonstrated that a decreased FMD is more apparent at higher levels of shear rate (after 50%, 70%, and 85% of maximum heart rate of training). The proposed mechanism may involve limiting
Resistance training can generate a high blood pressure of up to 400 mmHg.27 Our experiment also found an augmentation of blood pressure after two training exercises in both the active and inactive groups. The potential mechanism to explain the decreased FMD following lat pull down training in inactive subjects may contribute to higher blood pressure following the training.28,29 In contrast to active subjects, the decrease of FMD might not appear in the higher blood pressure condition.30 This explains how both training exercises affect the different fitness statuses of active and inactive subjects. The correlation analyses in this communication have shown that the impairment of FMD following lat pull down training in the LI group may be resulted from the increased diastolic and mean arterial blood pressures, and the decreased pulse pressure. However, there was no change with bench press training. The improved FMD in the LA group did not correlate with the increased blood pressure; therefore, we believe that the enhanced FMD might mainly be resulted from increased shear rate. However, further studies are necessary to investigate the underlying mechanism of these outcomes.
There are some limitations in this study that should be mentioned. First, the only upper body training exercises selected were the bench press and lat pull down training. In order to determine the appropriate training posture for each muscle group, other postures of the upper body should be studied in the future. Second, the number of participants in each group was relatively small.
In conclusion, bench press and lat pull down training are recommended to enhance upper body strength. High fitness status can be acutely protected against the negative effects on vascular function following resistance training. For active persons, we suggest that they perform both lat pull down training and the bench press, without any limitations. However, for inactive persons, bench press training is recommended at the beginning in order to prevent the adverse effects of decreased FMD. After vascular adaptation is implemented, lat pull down training might be added to strengthen upper body muscles.
Declaration of interest
We declare that there is no conflict of interest in this research.
Acknowledgements
We would like to thank the subjects for participation. This research was supported in part by Sport science laboratory, Faculty of Physical Education, Srinakharinwirot University, Thailand.
References
Cite this article
TY - JOUR AU - Witid Mitranun AU - Prasit Peepathum PY - 2018 DA - 2018/02/07 TI - Brachial flow-mediated dilatation response to acute different upper body training postures in lean inactive vs. lean active men JO - Artery Research SP - 1 EP - 7 VL - 22 IS - C SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2018.01.003 DO - 10.1016/j.artres.2018.01.003 ID - Mitranun2018 ER -