
Central pressure should not be used in clinical practice
- DOI
- 10.1016/j.artres.2014.11.002How to use a DOI?
- Keywords
- Central pressure; Arterial stiffness; Aorta
- Abstract
The heart, brain and kidneys are key targets of pulsatile damage in older people and in patients with longstanding hypertension. These central organs are exposed to central systolic and pulse pressures, which may differ from the corresponding peripheral pressures measured in the brachial artery. Studies employing the generalized transfer function as a means to estimate central pressure have demonstrated a large difference between central and peripheral systolic and pulse pressure that diminishes with age but remains substantial even in octogenarians. As a result of this persistent difference, some have advocated that central pressure may represent a more robust indicator of risk for target organ damage and major cardiovascular disease events. From the perspective of risk prediction, it is important to acknowledge that a new technique must add incremental predictive value to what is already commonly measured. Thus, in order to justify the added complexity and expense implicit in the measurement, central pressure must be shown to add significantly to a risk factor model that includes standard cardiovascular disease risk factors. A limited number of studies have shown marginally better correlations between central pressure pulsatility and continuous measures of target organ damage in the heart. A similarly limited number of prospective studies in unique cohorts have suggested that central pressure may provide marginally better risk stratification, although no reclassification analysis has been published. Thus, currently available evidence does not provide sufficient justification for widespread adoption and routine use of central pressure measurements in clinical practice.
- Copyright
- © 2014 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Because of variable effects of timing and amplitude of wave reflections in the arterial system, peripheral blood pressure as conventionally assessed in the arm can differ from central blood pressure in the proximal aorta. As a result of this difference, recent consensus statements have suggested that central pressure may be a better marker of cardiovascular disease risk than the conventional blood pressure from which central blood pressure is derived.1,2 The hypothesis that central blood pressure should be a better marker of risk for cardiac complications of hypertension seems well founded. In the presence of a potentially large and highly variable relation between central and peripheral blood pressure, central pressure should provide a better measure of hemodynamic load on the heart and therefore should be a better indicator of cardiac risk. However, only a few studies have demonstrated differing relations of central and peripheral pressures with cardiac structure and function and no study has demonstrated that knowledge of central pressure meaningfully reclassifies risk. Furthermore, the concept that “central pressure” is a better indicator of central hemodynamic stress has been extrapolated to other target organs, such as the brain and kidneys, which lie a considerable distance from the heart and proximal aorta. Whether imputed or measured proximal aortic pressure is truly relevant to structure and function in these more distal locations within the arterial tree remains incompletely elucidated. Before central blood pressure can be recommended for widespread clinical usage, a number of critical technical limitations of currently available devices need to be resolved. Then, using properly validated, robust measures of central pressure, it will be necessary to demonstrate that knowledge of central pressure meaningfully reclassifies risk.
Technical limitations of devices that measure central pressure
A number of commercially available devices purport to measure central blood pressure. However, results from various devices vary widely and consensus on an optimal method to impute central pressure is lacking. Critically, methods used to calibrate peripheral waveforms that are used to derive the central pressure waveform are controversial and have a major effect on estimates of central pressure.3,4 Various approaches to calibration contribute to variable errors in estimated differences between central and peripheral pressures that exceed the actual differences in pressure between the 2 locations.5–7
One approach for estimating central pressure involves use of a generalized transfer function, which is applied to a peripheral pressure waveform in order to obtain a surrogate for the central pressure waveform.8 The transfer function is essentially a low pass (smoothing) filter that compensates for the boost in high frequency components of the pressure waveform as it travels from central aorta to the brachial or radial artery where the waveform is recorded by using a cuff or tonometer. Studies that used invasive peripheral waveforms have shown that central pressure can be estimated using such an approach.9 However, noninvasive devices generally measure systolic and diastolic blood pressure in the brachial artery and then use those values to calibrate the peak and trough of a radial pressure waveform (Fig. 1). Because of variable amplification of the pressure waveform as it travels from the brachial to the radial recording site, the calibration of the radial waveform with brachial systolic and diastolic pressure leads to underestimation of radial systolic, mean and pulse pressure, whereas diastolic pressure is comparable between brachial and radial sites.4,10 Since the radial waveform is improperly calibrated, the derived aortic pressure waveform will have systolic, mean and pulse pressures that are too low. When the underestimated values for central systolic and pulse pressure are then compared to brachial cuff pressure, the pressure difference is overestimated by an amount equal to pressure amplification between brachial and radial recording sites (Fig. 1). In order to avoid calibration errors, either a brachial waveform, which is obtained at the same location as cuff pressure, should be used as the source waveform from which to estimate central pressure or the radial waveform should be calibrated to brachial mean and diastolic pressures. The latter approach requires a brachial pressure waveform, which can be acquired by tonometry or by using the oscillometric pressure waveform recorded from a properly fitted and properly inflated brachial cuff. Using brachial blood pressure and a formula to estimate brachial mean pressure is not acceptable because the shape (or K) factor of the brachial pressure waveform is highly variable. In addition, the maximum amplitude algorithm, which is commonly employed in oscillometric devices to estimate mean arterial pressure, has limitations that may be related to arterial stiffness.11–13
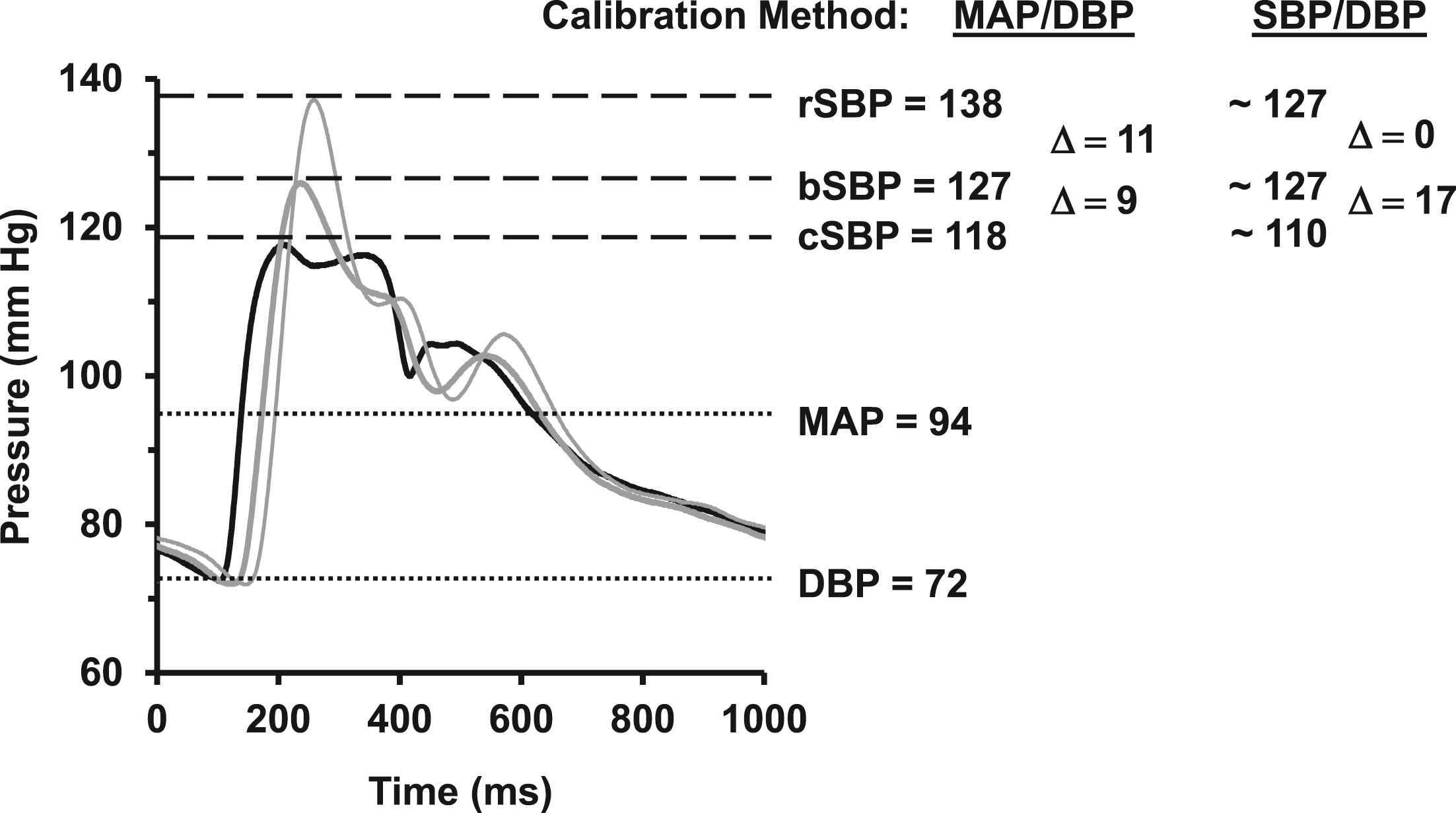
Waveform calibration. Optimal calibration of tonometry waveforms is based on the observation that mean arterial pressure (MAP) and diastolic pressure (DBP) are similar throughout the arterial system whereas systolic pressure can vary substantially because of variable timing of wave reflections. The carotid (black), brachial (thick gray) and radial (thin gray) waveforms in this figure were calibrated by using MAP and DBP and, therefore, demonstrate progressive amplification from carotid-to-brachial (9 mm Hg) and from brachial-to-radial (11 mm Hg) sites. If instead one uses brachial systolic (SBP) and DBP to calibrate the radial waveform, one will obtain a central pressure that is too low because the radial pressure was too low. When one then compares this artificially low central pressure to brachial pressure, it seems that there is a large difference between central and peripheral pressures. However this difference represents the difference between central and radial—not central and brachial—pressures. Thus, incorrect calibration simultaneously underestimates central pressure and overestimates central-to-brachial pressure amplification.
An alternative approach for estimating central pressure involves finding the inflection point or peak created by the reflected wave in a properly calibrated brachial or radial pressure waveform. This landmark has been referred to as “SBP2.” Since flow in the aorta is low during late systole, pressure gradients in the arterial system are relatively small. Furthermore, since the late (reflected wave) pressure peak represents the dominant peak in most adults from midlife onward, the reflected wave peak recorded in the periphery (SBP2) may represent a surrogate for central aortic systolic pressure in older adults.14–17 However, devices that utilize the SBP2 approach based on a radial artery pressure waveform are limited by the same calibration issues described above for the transfer function approach.
Central pressure also can be assessed by using direct tonometry of the carotid waveform. Direct carotid tonometry can be performed quickly and robustly by a trained operator in 1–2 min. The resulting waveform requires calibration, which is based on the observation that mean and diastolic pressure are equal in large arteries (Fig. 1). Using direct carotid tonometry, we have shown that moderate differences between carotid and brachial systolic and pulse pressure have on average essentially equilibrated by midlife.18 Based on the foregoing observation, brachial pressure would appear to represent a reasonable surrogate for central pressure from midlife onward, although variability about the mean in individuals is clearly present.
Proper calibration also requires accurate noninvasive assessment of blood pressure. Most available central blood pressure devices depend on oscillometric blood pressure for calibration, whereas the de facto standard for noninvasive measurement of blood pressure is the traditional auscultatory method, which serves as the standard for validation of oscillometric devices. Many of the available oscillometric blood pressure devices are known to underestimate systolic and overestimate brachial diastolic blood pressure.7,19 Estimates of central pressure based on these faulty estimates of brachial blood pressure will be proportionally confounded. Use of auscultatory blood pressure, which represents the standard against which oscillometric devices are validated, limits errors implicit in oscillometric blood pressure estimation but necessitates careful training and quality control. In vascular projects at the Framingham Heart Study, the AGES-Reykjavik Study and the Jackson Heart Study, blood pressure is assessed by using a computer controlled blood pressure device designed and built by Cardiovascular Engineering, Inc. The system, which includes an integrated audio system and a broadband microphone in the cuff, records the complete blood pressure acquisition, including electrocardiogram, cuff mean and oscillometric pressure and microphone broadband and audio signals.18,20 As a result, trained analysts are able to playback and review all blood pressures in order to ensure that auscultatory systolic and diastolic pressures were properly identified. As a result, the analyses are free of the confounding effects of oftentimes proprietary assumptions implicit in oscillometric blood pressure determinations.
Key misconceptions and limitations of central blood pressure
Misconception: That observed differences between central and peripheral systolic and pulse pressure represent a physiologic signal. A number of recent publications have emphasized the potential for wide overlap of central blood pressure values across peripheral blood pressure groupings.2,21 However, these observations have not acknowledged the possibility that variable central pressure overlap across discrete peripheral blood pressure groupings is likely is heavily contaminated by measurement error. Prior studies have demonstrated an R2 > 0.90 for the relation between central and peripheral systolic pressure.22,23 This very high degree of correlation means that variation in the difference between central and peripheral pressure is quite small relative to the range of variability in peripheral or central pressure. In addition, the foregoing publications, which were based on the transfer function approach, presented relations between derived central and measured peripheral systolic blood pressure with a slope that was less than one, indicating that the difference between central and peripheral pressure increased with increasing brachial pressure.22,23 Such a pattern conflicts with the known equilibration of central and peripheral blood pressures that occurs with increasing arterial stiffness; however, the pattern is consistent with the low pass filter characteristics implicit in the transfer function approach. A low pass filter produces a waveform with a highly correlated pulse pressure that invariably has a lower amplitude than the original source waveform; therefore, a low pass filter will have a greater absolute effect on waveforms with a greater amplitude, resulting in divergence (rather than the expected convergence) of pressures at higher systolic pressure. In light of the observation that peripheral pressure explains more than 90% of the variance in central pressure, and given that derivation of central pressure requires input from at least one additional measurement (e.g., radial tonometry) that is subject to error, it seems likely that variability about the regression line relating central and peripheral pressure (i.e., the remaining 10% of variance) is predominantly noise.
Misconception: That true differences between central and peripheral pressure will necessarily provide important prognostic information. Caveats related to measurement and calibration techniques aside, most would agree that differences between central and peripheral pressure are strongly related to age and sex and also depend on the level of brachial systolic blood pressure. With advancing age and higher brachial systolic pressure, brachial and central pressures converge.18 In addition, the gap between central and peripheral pressure is lower in women across the full lifespan because women have higher central pressure augmentation than men. As noted above, the central systolic pressure determined by the transfer function method is very highly correlated with the peripheral pressure used for calibration. As a result of the foregoing observations, even in a minimally adjusted risk prediction model that includes just age and sex, it is difficult to demonstrate that central pressure adds independent prognostic information once brachial pressure has been considered. Such a model is intrinsically unstable because age, sex and brachial pressure will explain more than 90% of the variance in central pressure. Furthermore, much of the remaining unexplained variance in central pressure is likely to be measurement error, particularly in light of major known sources of error in the calibration blood pressure and procedure.
Limitation: Because of a lack of standardization, estimates of central pressure obtained by various devices vary widely. In studies that have performed direct comparisons of existing devices, agreement between devices is suboptimal.5–7 In many cases, variability attributable to device and calibration factors equals or exceeds variability in differences between brachial and central pressure,3 suggesting that brachial blood pressure may be a more robust surrogate for central pressure than values returned by various devices. In light of the low concordance between estimates of central pressure returned by various devices and the high degree of correlation between central and peripheral pressure, it seems that shifting the focus to improved methods for obtaining a robust estimate of peripheral pressure may be warranted. In addition, new approaches for estimating central pressure from a high quality peripheral waveform that has been properly calibrated should be explored and all methods should be validated against clinical endpoints in adequately powered observational or interventional studies.
Evidence that central blood pressure provides additive prognostic information
A number of studies have suggested that central pressure may provide novel physiologic or prognostic information that is missed by peripheral pressure. For example, central pressure has been shown to have a closer correlation with surrogate measures of cardiovascular disease.1 In addition, several outcome studies have shown that central pressure may be more closely related to events than peripheral pressure in various unique cohorts, including dialysis patients,24,25 Native Americans with a high prevalence of obesity and diabetes,26,27 and a nursing home cohort.28 However, many of these assertions were based on a comparison of correlation coefficients or hazard ratios rather than a demonstration that central pressure adds diagnostic or prognostic utility in a model that already considers peripheral pressure, which is the standard for introduction of a new biomarker.29 In addition, the generalizability of results obtained in narrowly defined samples has to be questioned and tested in a more representative sample of unselected or less highly selected individuals.
The observation that central and peripheral effects of therapeutic interventions may differ has been proposed as evidence that central pressure provides a superior measure of hemodynamic load on the heart and central organs.30 However, the Café study, which is frequently cited as an example of differential modulation of central and peripheral pressure, actually demonstrated that central and peripheral systolic had identical relations with events.31 Importantly, these equivalent results were observed despite the fact that central pressure was differentially modulated by therapy. Half of the patients in that study were treated with a drug (atenolol) that slows heart rate, lengthens the systolic ejection period, creates more overlap between the forward and reflected wave and systematically increases central pressure augmentation. In light of the known inferiority of atenolol for reduction of events, the relation between central pressure and events should have strengthened by the study design. Despite this potential bias in favor of central pressure, central and peripheral pressures had equivalent relations with events.
One could speculate on many possible reasons that Café failed to demonstrate superior risk stratification with central pressure. However, before assuming that differential lowering of central pressure necessarily will have a favorable effect on outcome, it is important to consider potential adverse consequences of a reduction in wave reflection. Though often portrayed as harmful, wave reflection plays a critical role in proper function of the arterial system. Wave reflection limits the amount of pulsatile energy that penetrates into the periphery and thereby protects target organs from pulsatile damage.32–34 Vasodilator drugs reduce mean arterial pressure by reducing peripheral resistance, which reduces wave reflection and increases the amount of pulsatility that penetrates into the periphery. Increased transmission of pulsatility into the periphery may offset some of the favorable effect of reducing mean arterial pressure and may also confound the ability of central pressure to predict clinical outcomes.
A single published meta-analysis has examined relative prognostic value of central pressure and failed to show a significant difference between central and peripheral pressure.35 No study or meta-analysis has demonstrated that central pressure meaningfully reclassifies risk in a model that considers standard risk factors, including conventional brachial artery systolic pressure. Until such evidence is available, a recommendation in favor of widespread usage of central blood pressure in clinical practice is premature.
Moving blood pressure research out of the 19th century
The premise that there can be substantial differences between, and differential effects of interventions on, central and peripheral systolic and pulse pressure is widely accepted. There is little doubt that peripheral and central blood pressure waveform characteristics beyond peak and trough values provide novel information regarding cardiovascular physiology and (potentially) cardiovascular disease risk. Proponents of central blood pressure frequently emphasize the antiquated approach to peripheral blood pressure measurement, which has changed little since it was introduced more than 100 years ago. However, all current methods for estimating central pressure are critically dependent on concurrent assessment of conventional peripheral blood pressure in order to calibrate the putative central pressure waveform. Perhaps an important first step that has been overlooked is critical reevaluation of the approach used to estimate and report brachial blood pressure. Most central pressure devices utilize oscillometric blood pressure as a means to calibrate the central pressure waveform, despite well-known issues with oscillometric blood pressure determination that require further elucidation. In addition, devices measure and report systolic and diastolic pressure rather than mean arterial pressure and pulse pressure, which has contributed to the calibration difficulties discussed earlier. The calibration issue could be avoided if devices reported robust and accurate measures of mean arterial pressure in addition to systolic and diastolic pressure. However, it is important to note that the maximum amplitude algorithm, which oscillometric devices often employ to estimate mean arterial pressure, is susceptible to errors that are related to arterial stiffness.12,13 Newer algorithms that employ properly acquired and calibrated brachial pressure waveforms may be able to circumvent limitations of the maximum oscillometric amplitude approach, although additional research is needed to evaluate this question.
High blood pressure represents the leading modifiable risk factor for premature morbidity throughout the world. Therefore, development of devices that improve our ability to detect and treat high blood pressure remains an urgent public health priority. Newer devices that better stratify risk and provide superior monitoring of favorable (or unfavorable) effects of therapy are clearly needed. In order to gain widespread clinical acceptance, such devices will need to provide demonstrable superiority over existing (if antiquated) approaches to blood pressure measurement. The time for presenting theoretical advantages of pressure waveform analysis and central blood pressure measurement has passed. We now need clear evidence in adequately powered observational and interventional studies that novel approaches to blood pressure assessment and waveform analysis provide superior assessment of risk and monitoring of therapy.
Conflict of interest statement
Dr. Mitchell is the owner of Cardiovascular Engineering, Inc., a company that develops and manufactures devices to measure vascular stiffness, serves as a consultant to and receives honoraria from Novartis, Merck, and Servier and is funded by research grants HL094898, DK082447, HL107385 and HL104184 from the National Institutes of Health.
References
Cite this article
TY - JOUR AU - Gary F. Mitchell PY - 2014 DA - 2014/12/08 TI - Central pressure should not be used in clinical practice JO - Artery Research SP - 8 EP - 13 VL - 9 IS - C SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2014.11.002 DO - 10.1016/j.artres.2014.11.002 ID - Mitchell2014 ER -