
Sex differences in noninvasive estimates of left ventricular pressure energetics but not myocardial oxygen demand in young adults
- DOI
- 10.1016/j.artres.2014.07.003How to use a DOI?
- Keywords
- Pressure wave reflections; Blood pressure; Women; Pulse wave analysis
- Abstract
Background: Sex differences in arterial stiffness and wave reflections may lead to disproportionate increases in afterload and myocardial work in women. We examined sex differences in arterial stiffness, pressure from wave reflections, measures of left ventricular (LV) energetics and myocardial work.
Methods: 99 Healthy adults participated in this study 84 were selected (42 females, 42 males) to be matched for potential confounders of central hemodynamic burden such as age, BMI, and mean arterial pressure. Aortic pressure waves were derived from the radial artery using a generalized transfer function. Pulse contour analysis and wave separation analysis were used to obtain: pulse wave velocity (PWV) as a measure of aortic stiffness, augmentation index (AIx) and reflection index (RIx) as measures of global wave reflections, LV pressure effort (ΔEw) as a measure of LV energy required to overcome wave reflections and the subendocardial viability ratio (SEVR) as a proxy of myocardial work.
Results: Women exhibited higher ΔEw (p < 0.05), heart rate corrected AIx (p < 0.05) and RIx (p < 0.01), and lower PWV (p < 0.001) compared to men. Pressure from wave reflections (Pb) was significantly associated with ΔEw in women (r = 0.81, p < 0.001), but not in men (r = 0.14, p > 0.05). There were no sex differences for SEVR (p = 0.4).
Conclusion: Women had higher pressure from wave reflections which was associated with greater LV pressure effort compared to men. Although women had increased LV pressure effort, proxies of myocardial perfusion and work were not affected.
- Copyright
- © 2014 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
As the left ventricle (LV) contracts, a pressure wave is transmitted into the aorta and propagated throughout the arterial tree. This pressure wave will encounter various points of impedance due to change in vessel stiffness, bifurcations, and/or high resistance arterioles. Numerous smaller pressure waves are then reflected back toward the LV and summate to augment central aortic blood pressure and thus afterload.1 Central aortic pressure augmentation can be influenced by both the magnitude as well as the timing of reflected pressure waves.1 Optimal ventricular-vascular coupling ensures that wave reflections arrive during diastole, enhancing perfusion of the coronary arteries.1 Additionally, central pressure augmentation is minimized during systole so that the oxygen requirements of the myocardium are kept nominal.2
With aging or in the presence of diseases, wave reflections of greater magnitude return to the heart earlier in the cardiac cycle.3 The augmentation of central pressure caused by wave reflections increases the systolic load placed on the LV and thus increases LV oxygen requirements4 predisposing the myocardium to ischemia.5 Extra work placed on the LV that does not positively contribute to stroke volume ejection is referred to as “wasted pressure effort” (the energy needed to by the LV to overcome afterload due to wave reflections).4,6 LV wasted pressure effort (ΔEw) is associated with cardiac target organ damage (i.e. LV hypertrophy) and has been hypothesized to play a critical role in the pathogenesis of heart failure.4
Women typically have greater central hemodynamic load compared to age-matched men and this has been linked to diastolic dysfunction, myocardial ischemia and higher incidences of heart failure with preserved ejection fraction in women.2,7–12 Studies investigating sex differences in central hemodynamics as they relate to LV energetics and coronary perfusion have been done predominantly in older adults.2,13–16 However sex differences in pressure from wave reflections arise at a young age.17 Whether there are subsequently sex differences in LV wasted pressure effort and indices of coronary perfusion in younger adults is unknown.
Traditional means of assessing pressure from wave reflections use the augmentation index (AIx) as a surrogate of global wave reflections. Wave separation analysis (WSA) allows for partitioning of the pressure wave into its forward (Pf) and reflected/backward (Pb) constituent waves.18,19 This method may be more appropriate to examine central hemodynamic load in young adults with “Type C” waveforms (i.e. late systolic pressure is < primary wave pressure yielding a negative AIx).20–23 Although WSA requires assessment of a central flow envelope for pressure wave deconstruction, recent techniques that make use of a pseudo-flow waveform have proven of value.18,19,24 Using this novel approach, the purpose of this study was to investigate sex differences in pressure from wave reflections, LV wasted pressure effort and metrics of myocardial work and coronary perfusion in young adults. We hypothesized that compared to age-matched men, young women would have higher pressure from wave reflections and this would be associated with increased wasted LV pressure effort, increased myocardial work and reduced coronary perfusion.
Methods
Participants
Ninety-nine young healthy, normotensive men (n = 49) and women (n = 50) from the local university community volunteered to participate in this study. All participants were nonsmokers and free from cardiovascular, metabolic, renal, and respiratory disease as self-reported by a health history questionnaire. Participants did not take cardiovascular medications of any kind. For the female participants, there was no standardization for the timing of measurements relative to menstrual cycle phase. From the 99 subjects studied, 42 men and 42 women were selected in order to ensure no statistically significant differences in variables that may affect central hemodynamics. Confounding variables considered included: age, mean arterial pressure, body mass index, and heart rate. This study was approved by the institutional review board of Syracuse University, and all subjects provided written informed consent before study initiation.
Study design
Hemodynamic measures were made in a quiet, dimly lit, stable temperature (20°–21 °C) room. All participants were instructed to refrain from all forms of habitual exercise for 24 h before testing, and all testing was completed in the postprandial state with participants abstaining from caffeine for >6 h and food for >4 h. Height and weight were measured using a wall-mounted ruler and electronic scale, respectively. Participants then rested in the supine position for 10 min before measurement of brachial blood pressure (BP). Brachial BP was measured in duplicate using a previously validated automated oscillometric cuff (Panasonic Ew3109, Secaucus, NJ).25 If the 2 measures were not within 5 mm Hg for both systolic BP and diastolic BP, an additional measure was taken. BP measures were made until 2 consecutive readings were within 5 mm Hg for both systolic and diastolic BP.
Pulse contour analysis
Aortic pressure waveforms were synthesized from a 10- epoch period in duplicate using radial applanation tonometry and a generalized transfer function (SphygmoCor; AtCor Medical, Sydney, Australia) that has been previously validated.26 The aortic pressure waveform was calibrated using brachial mean arterial pressure and diastolic pressure. For mean arterial pressure, a form factor of 0.4 was used because the “one-third” rule may underestimate true mean arterial pressure.27 Pulse pressure (PP) was calculated as systolic blood pressure minus diastolic blood pressure. Augmentation index (AIx) was calculated as the difference between the early- and late systolic peaks of the aortic waveform to the total PP expressed as a percentage (P2 − P1/PP × 100). A novel wave separation technique based on the original flow triangulation work of Westerhof et al. and Kips et al. was used, as previously described in detail to assess forward wave pressure (Pf) and reflected/backward wave pressure (Pb).18,19 Wave reflection index was calculated as Pb/Pf × 100.24 Additionally, aortic pulse wave velocity (PWV) was estimated using the time lag between derived aortic Pf and Pb.28 Quantification of the effective reflection distance was calculated as PWV × 0.5 Tr.20 The average values obtained from the 2 radial measures were used for all analyses.
Calculation of LV energetics, myocardial work and coronary perfusion
Wasted pressure effort was calculated using the equation ΔEw = 2.09 × AP × (ED-Tr).4,29 Augmented pressure (AP) is the difference between peak pressure and pressure at the inflection point caused by wave reflection. Ejection duration (ED) is the time from the onset of pressure increase to the closure of the aortic valve assessed by the dicrotic notch. Time to reflection (Tr) is the systolic travel time of the pressure wave, and 2.09 is a constant. The ratio of myocardial perfusion relative to left-ventricular workload was calculated as the subendocardial viability ratio (SEVR or Buckberg Index), using systolic and diastolic pressure-time integrals. The diastolic pressure time integral (DPTI) is an estimate of the oxygen supply to the myocardium while the systolic pressure time integral (SPTI) is a measure of the amount of work being done by the LV.2
Statistical analysis
Data are reported as mean ± SEM. A priori significance was set at p < 0.05. An analysis of variance was used to compare all continuous variables in women versus men. Categorical variables were compared using chi-square tests. Analysis of covariance was used to additionally correct for height and heart rate when comparing select outcome measures. Pearson bivariate correlations were used to investigate associations between variables of interest. Statistical Package for the Social Sciences (SPSS, Chicago, IL) version 21.0 was used for all analyses.
Results
Participant characteristics are shown in Table 1. Eighty-four participants (42 men, 42 women) were included in this study for final analysis. By design, men and women did not statistically differ in age, BMI, mean arterial pressure, and heart rate (p > 0.05). Women were significantly shorter than men (p < 0.05). The percentage of participants who had a family history of cardiovascular disease did not differ between sexes (p > 0.05).
| Variable | All (n = 84) | Men (n = 42) | Women (n = 42) | p-Value |
|---|---|---|---|---|
| Age (years) | 26 ± 1 | 27 ± 1 | 26 ± 1 | 0.47 |
| Height (m) | 1.7 ± 0.01 | 1.8 ± 0.01 | 1.6 ± 0.01 | <0.001 |
| Weight (kg) | 72.5 ± 1.4 | 78.8 ± 1.9 | 66.3 ± 1.4 | <0.001 |
| Body mass index (kg/m2) | 24.4 ± 0.3 | 24.5 ± 0.4 | 24.3 ± 0.4 | 0.72 |
| Oral contraceptive use | – | – | 22 (52%) | – |
| Family Hx CVD | 10 (12%) | 6 (14%) | 4 (9.5%) | 0.89 |
HX, history; CVD, cardiovascular disease.
Participant characteristics.
Hemodynamic variables
Hemodynamic variables are shown in Table 2. Wave separation analysis (WSA) could not be performed in 4 participants. Measures of Pf, Pb and RIx are therefore shown for 80 participants (male = 39, female = 41). PWV from WSA could not be obtained from 6 participants. Therefore PWV data are shown for a total 78 participants (male = 39, female = 39). As can be seen in Table 2, compared to men women had lower PWV (p < 0.001), Pf (p < 0.05), Tr (p < 0.05), effective reflection distance (p < 0.001), but higher heart rate corrected AIx and RIx (p < 0.01). There were no significant sex differences in ejection duration, systolic and diastolic pressure time integral, subendocardial viability ratio, or Pb (p > 0.05 for all). Women had a significantly higher wasted pressure effort than men (Fig. 1). Women presented with a mean wasted pressure effort of 1162.7 ± 314.4 dynes s cm2, while men had a mean of 87.7 ± 201.9 dynes s cm2 (p < 0.01). Co-varying for height attenuated differences between women and men central hemodynamic indices but sex differences still prevailed: AIx (adjusted means: 4.6 ± 2.7 females, 2.7 ± 2.7 males, p < 0.05), RIx (adjusted means: 49 ± 2.6% females, 46 ± 2.7 males, p < 0.05) and ΔEw (adjusted means: 873.3 ± 332.6 dynes s·cm2 females and 391.4 ± 344.3 dynes s·cm2 males, p < 0.05).
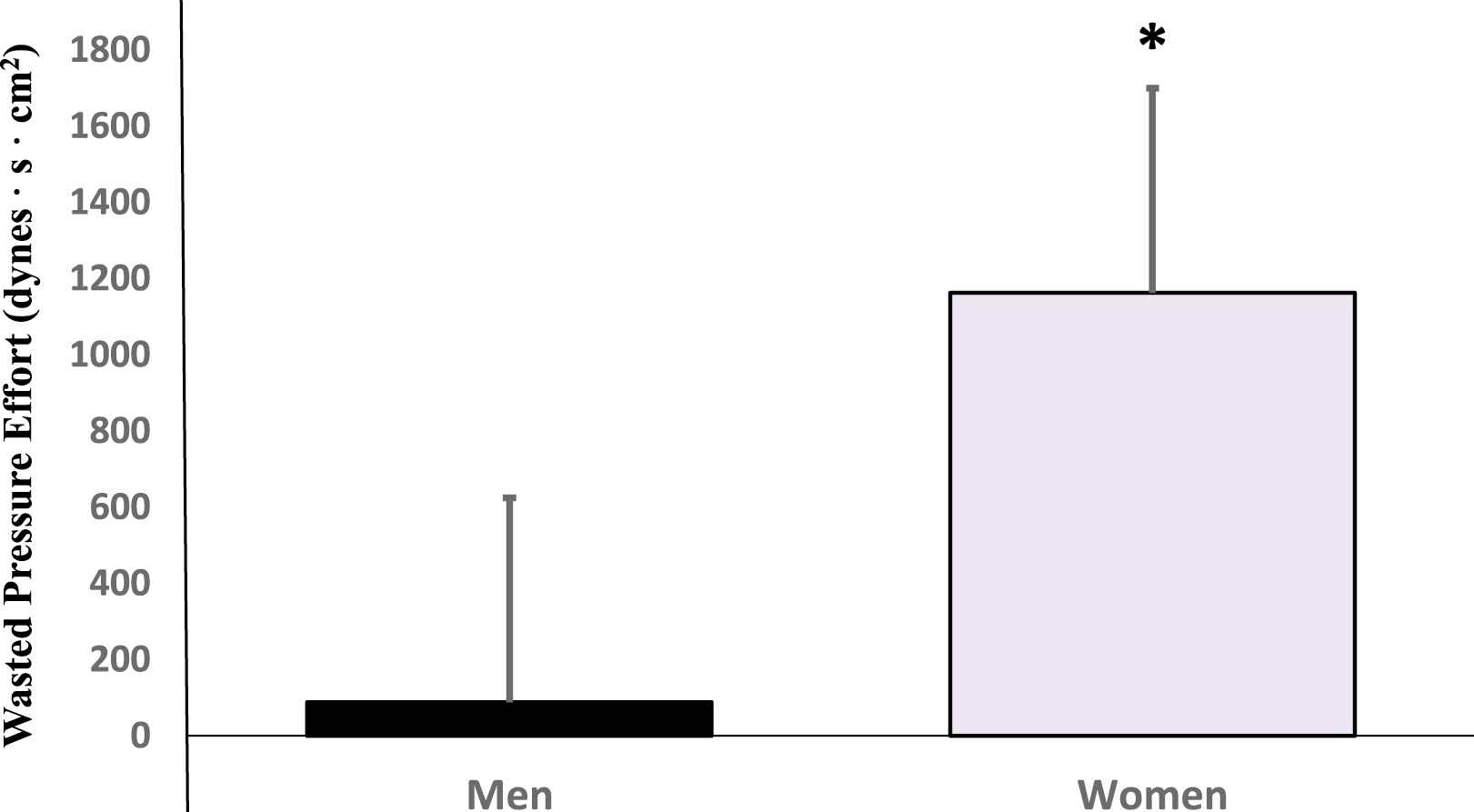
Sex differences in wasted pressure effort of the left ventricle. *p < 0.05.
| Variable | All | Men | Women | p-Value |
|---|---|---|---|---|
| Brachial systolic blood pressure (mm Hg) | 118 ± 1 | 120 ± 1 | 115 ± 1 | 0.001 |
| Brachial diastolic blood pressure (mm Hg) | 73 ± 1 | 73 ± 1 | 73 ± 1 | 0.6 |
| Mean arterial pressure (mm Hg) | 88 ± 1 | 89 ± 1 | 87 ± 1 | 0.12 |
| Brachial pulse pressure (mm Hg) | 45 ± 1 | 48 ± 1 | 42 ± 1 | <0.001 |
| Ejection duration (ms) | 335.6 ± 2.3 | 334.1 ± 3.2 | 337.01 ± 3.3 | 0.53 |
| Augmentation indexa (%) | 3.7 ± 1.4 | 0.6 ± 2.0 | 6.8 ± 2.0 | 0.003 |
| Systolic pressure time integral | 1959 ± 33 | 1935 ± 52 | 1985 ± 43 | 0.5 |
| Diastolic pressure time integral | 3283 ± 34 | 3312 ± 46 | 3255 ± 49 | 0.4 |
| Subendocardial viability ratio (%) | 173 ± 4 | 177 ± 6 | 169 ± 5 | 0.4 |
| Heart rate (bpm) | 61 ± 1 | 59 ± 2 | 61 ± 1 | 0.2 |
| Time to reflection (ms) | 162.5 ± 2.6 | 171.7 ± 3.7 | 153.6 ± 3.0 | <0.001 |
| Central systolic pressure (mm Hg) | 103 ± 1 | 104 ± 1 | 102 ± 1 | 0.2 |
| Central diastolic pressure (mm Hg) | 74 ± 1 | 74 ± 1 | 74 ± 1 | 0.7 |
| Central pulse pressure (mm Hg) | 29 ± 1 | 30 ± 1 | 27 ± 1 | 0.014 |
| Pulse-wave velocity (m/s) | 6.2 ± 0.12 | 6.7 ± 0.2 | 5.8 ± 0.2 | <0.001 |
| Forward wave pressure (mm Hg) | 26 ± 0.71 | 28 ± 1 | 24 ± 1 | 0.001 |
| Backward wave pressure (mm Hg) | 12 ± 0.42 | 12 ± 1 | 12 ± 1 | 0.5 |
| Reflection indexa (%) | 47 ± 1.4 | 44 ± 2 | 50 ± 2 | 0.004 |
| Effective reflection distance (cm) | 50.2 ± 1.3 | 55.9 ± 2.0 | 44.7 ± 1.4 | <0.001 |
Adjusted for heart rate.
Hemodynamic variables in men and women.
Correlation analysis
Correlation matrices for central hemodynamic measures within each sex/gender are shown in Tables 3 and 4. Correlations of interest are as follows. There was a significant association between height and wasted pressure effort in the population as a whole (r = −0.24, p < 0.05). When examining associations within groups, height was significantly negatively associated with wasted pressure effort in women (r = −0.40, p = 0.01; Fig. 3a), but not men (r = 0.23, p = 0.12, Fig. 3b). Pb was significantly associated with wasted pressure effort in women (r = 0.79, p < 0.001), but not in men (r = 0.089, p > 0.05) (Fig. 2).
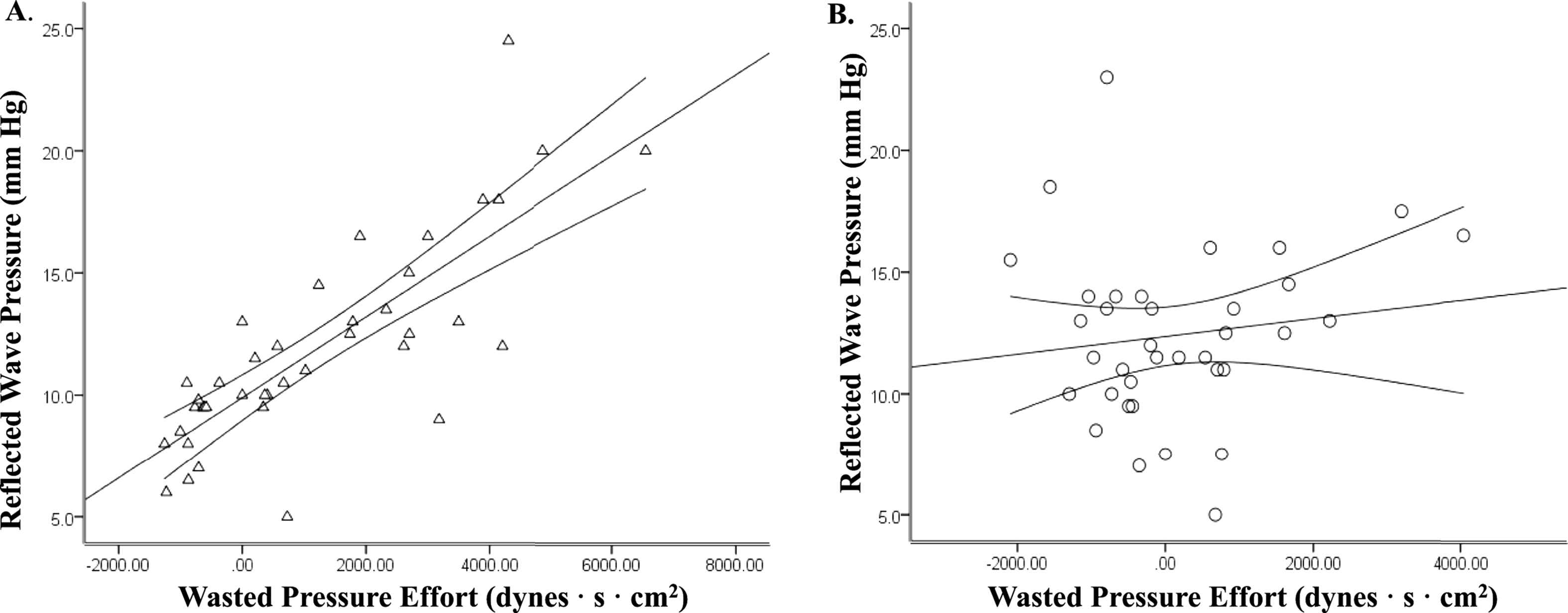
Association between reflected wave pressure (Pb) and wasted pressure effort in women (panel A) and men (panel B).
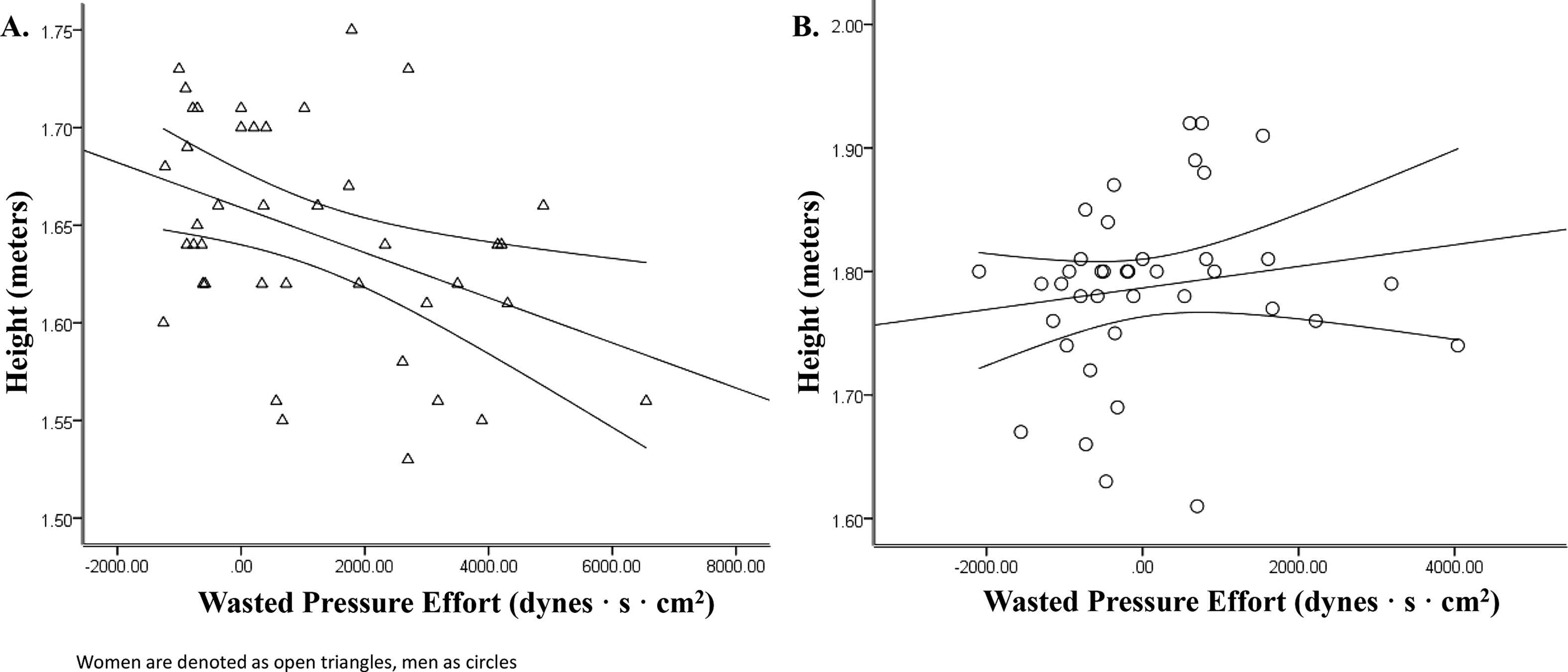
Association between height and wasted pressure effort in women (panel A) and men (panel B).
| Height | SPTI | DPTI | AIx | Tr | PWV | Pf | Pb | ΔEw | ERD | |
|---|---|---|---|---|---|---|---|---|---|---|
| SPTI | −0.17 | |||||||||
| DPTI | −0.37* | −0.34* | ||||||||
| AIx | −0.30 | −0.03 | 0.53* | |||||||
| Tr | 0.13 | 0.14 | −0.13 | −0.23 | ||||||
| PWV | 0.06 | −0.31 | 0.16 | 0.20 | 0.09 | |||||
| Pf | −0.01 | −0.03 | 0.06 | 0.08 | 0.001 | 0.32* | ||||
| Pb | −0.29 | −0.08 | 0.52* | 0.83* | −0.23 | 0.27 | 0.49* | |||
| ΔEw | −0.41* | −0.16 | 0.64* | 0.85* | −0.25 | 0.31 | 0.24 | 0.81* | ||
| ERD | 0.17 | −0.19 | 0.04 | −0.02 | 0.66* | 0.81* | 0.25 | 0.07 | 0.05 | |
| RIx | −0.32* | −0.08 | 0.57* | 0.92* | −0.28 | 0.13 | −0.05 | 0.82* | 0.81* | −0.05 |
SPTI, systolic pressure time integral; DPTI, diastolic pressure time integral; AIx, augmentation index; Tr, reflected wave transit time; PWV, pulse-wave velocity; Pf, forward wave pressure; Pb, reflected wave pressure; ΔEw, left ventricular wasted pressure effort; RIx, reflection index (Pb/Pf); ERD, effective reflection distance.
Significant association p < 0.05.
Univariate associations for selected central hemodynamic parameters in women.
| Height | SPTI | DPTI | AIx | Tr | PWV | Pf | Pb | ΔEw | ERD | |
|---|---|---|---|---|---|---|---|---|---|---|
| SPTI | −0.14 | |||||||||
| DPTI | 0.10 | −0.35* | ||||||||
| AIx | 0.07 | −0.01 | 0.22 | |||||||
| Tr | 0.36* | −0.10 | −0.44* | −0.44* | ||||||
| PWV | 0.02 | 0.16 | −0.15 | −0.09 | ||||||
| Pf | −0.20 | −0.07 | −0.03 | −0.46* | −0.19 | 0.45* | ||||
| Pb | −0.10 | −0.05 | 0.14 | 0.34* | −0.36* | 0.39* | 0.58* | |||
| ΔEw | 0.15 | −0.07 | 0.10 | 0.77* | −0.23 | −0.02 | −0.47* | 0.14 | ||
| ERD | 0.11 | 0.09 | −0.39* | −0.37* | 0.60* | 0.80* | 0.29 | 0.13 | −0.15 | |
| RIx | 0.16 | −0.05 | 0.18 | 0.86* | −0.18 | −0.13 | −0.40* | 0.49* | 0.68* | −0.23 |
SPTI, systolic pressure time integral; DPTI, diastolic pressure time integral; AIx, augmentation index; Tr, reflected wave transit time; PWV, pulse-wave velocity; Pf, forward wave pressure; Pb, reflected wave pressure; ΔEw, left ventricular wasted pressure effort; RIx, reflection index (Pb/Pf); ERD, effective reflection distance.
Significant association p < 0.05.
Univariate associations for selected central hemodynamic parameters in men.
Discussion
In this study we examined sex differences in central hemodynamics, left ventricular energetics, and myocardial work in young adults. Novel findings of this study were: 1) women had higher wasted LV pressure effort than men; 2) wave reflection magnitude assessed using traditional pulse contour analysis (i.e. AIx) or wave separation analysis (i.e. RIx) was higher in women 3) pressure from wave reflections (Pb) was strongly associated with wasted pressure effort in women but not men; 4) there were no sex differences in measures of myocardial work or coronary perfusion in younger adults. Collectively, these results indicate that wasted LV pressure effort is greater in young women than men and may be partially driven by height-mediated differences in pressure from wave reflections. Despite these notable sex differences in central hemodynamic load, increased LV pressure effort in young women did not negatively translate into increased myocardial work or reduced coronary perfusion.
Wasted pressure effort and wave reflections
To our knowledge, this is the first study to explore sex differences in wasted LV pressure effort in young adults. Consistent with previous work done in older adults,4 our findings indicate that young women have higher wasted LV pressure effort, suggesting greater afterload placed on the LV due to wave reflections. Wasted pressure effort is linked to development of cardiac end-target organ damage.4 This becomes particularly apparent in the sixth decade of life with more women developing systolic and diastolic dysfunction, LVH, myocardial ischemia and heart failure than age-matched men.16,30,31 Indeed the association between central hemodynamic burden and LV dysfunction is greater in women than in men.11
Previous work from Hashimoto et al. has suggested that wasted LV pressure effort may be more sensitive to alterations in wave reflection magnitude rather than timing as ΔEw demonstrated poor associations with PWV and Tr.4,32 Although there were sex differences in Tr with women having faster wave travel time in the present study, Tr was not associated with ΔEw in either women or men in our younger cohort. Moreover, although no differences in Pb, when expressed relative to the magnitude of the incident wave (Pf) women demonstrated higher overall reflection magnitude.14 A novel observation was that wasted LV pressure effort was highly correlated with Pb in women but not men. Taken together and these findings suggest that the relative magnitude of reflected waves may contribute to the development of higher wasted LV pressure effort in women compared to men.
Wave reflections, particularly in younger women, have been shown to be one of the main determinants of increased central pulse pressure, independent of changes in carotid-femoral pulse wave velocity.33 Women had lower measures of aortic stiffness in the present study compared to their male counterparts and this is consistent with previous studies assessing carotid-femoral PWV in younger adults.17,34 This may offer insight into the lower Pf in women as incident wave pressure is largely determined by regional stiffness/impedance and LV ejection dynamics via a Windkessel effect. Aortic PWV was associated with Pf in both women and men. In younger women, there may be more optimal coupling between LV and the ascending aorta contributing to more ideal impedance matching and minimal genesis of pulsatile hemodynamics via increased forward wave pressure. It should be stressed that these relationships are known to change with advancing age and reduced aortic diameter coupled with increases in aortic stiffness in older women result in increases in Pf (from altered characteristic impedance) contributing to increases in central pulsatile load.3,35–37 Although men had higher PWV and greater incident wave pressure than women, Pf was paradoxically inversely associated with LV pressure effort in men. Pf as measured herein may be a better proxy of LV ejection/contractility in young men, not aortic characteristic impedance. With reduced pressure from wave reflections in young men, almost all LV energy contributes to forward stroke volume propulsion and none is wasted per se.
Myocardial-coronary oxygen supply and demand
There were no sex differences in diastolic and systolic pressure time integrals suggesting similar coronary oxygen supply and demand in men and women. Moreover the ratio of oxygen supply and demand known as the subendocardial viability ratio (SEVR) was not significantly different between men and women. In older adults and those with heart failure, coronary oxygen supply and demand can be compromised, often due to changes in wave reflections.2 Earlier return of wave reflections augment central systolic blood pressure, and take away from perfusion time and pressure during diastole. It has been shown that older women have increased systolic TTI, reduced diastolic TTI and reduced SEVR suggesting increased myocardial work and diminished coronary perfusion.2 Although there were significant differences in pressure from wave reflections and LV wasted pressure effort in young women and men, these differences did not further result in detrimental changes in measures of LV myocardial work and coronary perfusion in our younger cohort.
Influence of height, timing and pressure from wave reflections
Sex differences in the timing and magnitude of pressure from wave reflections have, in part, been attributed to differences in height.13,17,38 In general, shorter stature is synonymous with a smaller arterial tree. This has been posited to move reflection sites closer to the heart resulting in shorter transit time of pressure waves.39,40 In the current study, men were significantly taller than their female counterparts. Although women had lower PWV, this was not enough to equipoise sex differences in Tr due to differences in height. As such women had shorter effective reflection distances. We noted prominent associations between height and AIx (RIx) as well as height and wasted LV pressure effort. Interestingly, the inverse association between height and wasted LV pressure effort was more pronounced in women than men. Moreover, co-varying for height greatly attenuated differences measured for AIx, RIx and wasted LV pressure effort. Recent findings from Reeve et al., have suggested that height is an important risk factor for coronary disease and CVD mortality and this may be mediated by detrimental effects on central hemodynamics.41 Thus sex differences in height do explain, in part, some of the noted sex differences in LV pressure effort seen in the present study and this supports recent studies expounding the importance of height as a CVD risk factor.
Limitations
Aortic PWV was estimated from synthesized aortic pressure waves (derived via the radial artery and a generalized transfer function) using wave separation analysis. The current gold standard for measuring aortic stiffness is carotid-femoral PWV. Correlations between PWV assessed using WSA versus the carotid-femoral method have been shown to be moderately high.28 WSA was performed with use of a pseudoflow waveform that approximates aortic flow based on the contour of the synthesized aortic pressure wave rather than an actual aortic flow velocity envelope.18,19 Finally, we did not control for timing of measures relative to the menstrual cycle nor did we exclude based on use of oral contraceptives. Recent studies note minimal effects of the menstrual cycle and oral contraceptives on aortic stiffness and AIx.42–44 In the current study, there were no differences in AIx, RIx or ΔEw in women taking versus not taking oral contraceptives. Moreover, it would be hypothesized that measuring central hemodynamics during the early follicular phase (as is standard in vascular biology research; when estrogen is at its nadir) would result in greater endothelial dysfunction and increased peripheral vascular tone and thus greater pressure from wave reflections. Thus the very large sex differences in LV pressure effort in the present study may have been underestimated.
Conclusion
In conclusion, young women have higher values of wasted LV pressure effort but comparable myocardial work and coronary perfusion when compared to their male counter-parts. Further research is needed to examine how augmented wasted LV pressure effort in women in young adulthood might hasten development of LV dysfunction and heart failure later in life.
Conflicts of interest
None.
References
Cite this article
TY - JOUR AU - William E. Hughes AU - Nicole L. Spartano AU - Wesley K. Lefferts AU - Jaqueline A. Augustine AU - Kevin S. Heffernan PY - 2014 DA - 2014/08/28 TI - Sex differences in noninvasive estimates of left ventricular pressure energetics but not myocardial oxygen demand in young adults JO - Artery Research SP - 197 EP - 204 VL - 8 IS - 4 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2014.07.003 DO - 10.1016/j.artres.2014.07.003 ID - Hughes2014 ER -