
Effects of a Personalized Physical Exercise Program in the Ventricular-arterial Coupling of Older Adults. A Pilot Study
- DOI
- 10.2991/artres.k.200222.001How to use a DOI?
- Keywords
- Ventricular-arterial coupling; physical exercise; elderly; cardiovascular efficiency
- Abstract
Introduction: This study was aimed at evaluating the changes in the Ventricular-Arterial Coupling (VAC) of old adults after the implementation of a multidisciplinary intervention program comprising a tailored physical exercise component.
Methods: A non-randomized pilot study, enrolling 21 old adults with age above 65 years of age (mean 81.08 years). The participants were divided into two groups (Group 1 and 2), both subject to a baseline thorough and multidisciplinary diagnostic evaluation. A tailored intervention program was implemented for a period of 3 months, after which the participants were re-evaluated. The Group 2 included a component of tailored exercise training and physiotherapy intervention. Central and peripheral Blood Pressure (BP) and hemodynamic parameters related to cardiovascular efficiency were evaluated by transthoracic echocardiography and pulse wave analysis. Self-efficacy for exercise scales as well as handgrip strength and nutritional status were also evaluated at baseline and after intervention.
Results: Baseline diagnostic information was similar in both groups. After the intervention, significant changes were observed in Group 2, mainly a reduction in BP, in arterial stiffness and a better cardiovascular efficiency was also depicted, with a decrease in the stroke work and an increase in the VAC, as well as in the left ventricle efficiency parameter. Regarding the indicators of frailty, there was an improvement in handgrip strength and self-efficacy for exercise in Group 2. No significant changes were observed in Group 1.
Conclusion: The results of this pilot study highlight the positive modulation provided by a tailored physical exercise approach of the old adult, increasing cardiac efficiency and thus constituting a factor for improving overall well-being. Large randomized trials are needed to further validate these findings.
- Copyright
- © 2020 Association for Research into Arterial Structure and Physiology. Publishing services by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
The demographic ageing is currently acknowledged as a major societal challenge with a significant impact on several dimensions of modern societies. The Portuguese demographic data in 2017 indicated that more than 21.5% of the population was over 65 years old, and 13.8% was over 85 years old [1]. As the average life expectancy increases, so does the need for adequate health care to face the complexity and heterogeneity of individual ageing, with a strong focus on physical capacity, autonomy, family and social structure, literacy and culture, thus providing the basis for social participation and inclusion and ageing with greater dignity. It is therefore necessary to have well-trained professionals to ensure adequate and personalized health care to each individual through the life course. It is also important to recognize the need to generate knowledge in gerontology, not only because of our demographic reality but also to ensure innovation and management of the best health care [2].
Ageing is known to produce several cardiovascular changes, such as the reduction in cardiac output and maximum Heart Rate (HR), the increase in Blood Pressure (BP) and the increase in Arterial Stiffness (AS), associated with a decrease in the ability to produce muscle work [3]. BP is one of the first changes resulting from aging and one of the easiest to detect through simple measurements. However, Systolic BP (SBP) increases more significantly as a consequence of the age-related arteriosclerosis, strongly related to the increase in the speed of the reflected waves which boosts systemic BP centrally as a function of its precocity, mainly increasing SBP with the maintenance, or even reduction, of central Diastolic BP (DBP) [4]. This hemodynamic phenomenon causes an increase in Pulse Pressure (PP), with higher pulsatility which in turn damages the arterial wall contributing to accelerated trajectories of arterial stiffening of the arteries. When this age-dependent adaptations occur in association with other cardiovascular risks, such as dyslipidemia, diabetes, smoking, obesity or sedentary lifestyle, arterial stiffening trajectory is further accelerated and the risk for major cardiovascular events increases significantly [5]. Physical exercise has been recognized for its potential to modulate the trajectories of AS and to improve overall cardiovascular health [6]. For example, Cameron et al. [7] demonstrated that physical exercise contributes to improve arterial function in patients with high cardiovascular risk. Physical exercise could thus promote better cardiovascular efficiency by improving the Ventricular-arterial Coupling (VAC) and coronary irrigation, especially in elderly individuals who were previously sedentary.
This study aims at demonstrating the cardiovascular benefits of physical exercise in the old adult, focusing mainly on cardiovascular efficiency as measured by the coupling of the left ventricle with the aorta – VAC. This parameter has been explored over the years, primarily by biophysicists, in animal models, and more recently, associated with the study of cardiovascular efficiency in humans [5–15], namely associating VAC with the increase in the cardiovascular efficiency at peak exercise [16]. However, studies associating VAC to cardiovascular efficiency gains related to physical exercise in old adults are scarce. Therefore, we designed a pilot non-randomized study to assess the effect of a tailored exercise intervention in the VAC and overall cardiovascular efficiency of the old adult.
2. MATERIALS AND METHODS
2.1. Study Design, Population and Ethics
A non-randomized study was designed to evaluate the effect of a multidisciplinary intervention program on heart function, AS and central hemodynamic indices in community dwelling elderly adults. The study cohort was recruited from a day care center in Portugal (Associação para a Defesa do Idoso e da Criança - ADIC, Vilarinho, Portugal). Individuals over 65 years of age, of both genders, physically autonomous, with no previous recent history of cerebrovascular events, no cognitive or neurological deficits, were invited to participate in the study. Twenty-one individuals who agreed to participate voluntarily in the study were included and were divided into two groups that differed only in the intervention of the physical exercise program: The control group (Group 1; n = 10) did not comply with the physical exercise plan and was asked to maintain normal life habits and to comply with the nutritional recommendations, the therapeutic counselling and the overall promotion of well-being. The intervention group (Group 2; n = 11) was submitted to a tailored physical activity and functional exercise plan and was also asked to maintain normal life habits and to comply with the same overall recommendations as the Group 1. The Group 2 adhere to the physical intervention plan during a three-month period (participation above 95% of the sessions).
The study was conducted taking into account the recommendations of the Declaration of Helsinki and approved by the Ethics Committee of the Polytechnic of Coimbra. The anonymity and confidentiality of the collected data were guaranteed. The study has strictly scientific objectives, with no conflicts of interest to declare. All participants signed an informed consent form.
2.2. Overall Procedure
Participants were recruited for the study in January 2018. Between February and March 2018, a multidisciplinary baseline diagnostic assessment was made to each participant, including the collection of sociodemographic information, clinical history with identification of comorbidities and ongoing therapy, determination of the dietary profile and physical activity profile, estimation of overall cardiovascular risk and history of falls. The grip strength was measured with an appropriate dynamometer. The Portuguese version of the self-efficacy questionnaire for physical exercise was used to assess the degree of individual confidence to perform activities [17]. The dietary profile was assessed by the Portuguese version of the ‘mini nutritional assessment’ [18]. Cognitive function was assessed by the Cambridge Neuropsychological Test Automated Battery (CANTAB - Cambridge Cognition, Cambridge, UK) platform [19,20]. The height was measured with a calibrated stadiometer. Weight and body composition were obtained through bioimpedance with an OMRON BF 511 device (OMRON HEALTHCARE Co., Ltd., Japan), assessing weight, percentage of fat mass, percentage of lean mass and level of visceral fat. Body Mass Index (BMI) was obtained as weight (kg)/height2 (m). Waist and hip perimeter were measured with an appropriate tape, using appropriate anatomical references according to the STEPS procedure of the WHO [21]. The waist-to-hip ratio was calculated. Brachial and central BP, and central hemodynamic parameters were automatically obtained with the AGEDIO device (IEM, Stolberg, Germany) from participants free of tobacco and caffeine consumption for a minimum period of 2 h, with the participant seated after a 5-min rest period, with the arm supported at the level of the heart and with the arm free of any constrictive effect of clothing, and with an arm cuff with an appropriate diameter positioned at the level of the brachial artery. Fasting blood glucose, cholesterol fractions and other biochemical parameters were obtained by collecting blood samples and analyzing them in appropriate and properly calibrated laboratory equipment. The overall cardiovascular risk was assessed by the SCORE tables [22].
2.3. Intervention
The intervention program involved all participants and was designed to meet the individual needs identified in the initial assessment. This included an adapted physical exercise plan and physiotherapy sessions, administered by a team composed of a physiotherapist and a certified physical education teacher, nutritional and therapeutic drug counselling by nutrition and pharmacy professionals, and hearing and occupational rehabilitation activities with cognitive stimulation involving professionals in the area of audiology, psychology and with advanced training in the area of health education.
The participants were divided into two groups according to their adherence to the physical exercise plan: Group 1 with low (below 50% of the sessions) or no adherence; Group 2 with good adherence (above 95% of the sessions). This physical exercise program was developed in a personalized way, consisting of outdoor aerobic exercise sessions and laboratory sessions with a dedicated technological platform [17] with the objective of increasing aerobic capacity and global strength, coordination and functionality. The aerobic exercise sessions followed the recommendations of the WHO [23] consisting of two sessions per week with the following structure: a 10-min walk on flat or slightly sloping ground, joint mobilization exercises with respiratory coordination and balance and coordination exercises (total duration per session: 1 h). The laboratory sessions took place three times a week (1-h sessions), including strength and balance/coordination exercises based on the Otago program [24] embedded in a technological platform using inertial and pressure sensors, feedback and exergames. The intervention was implemented for three months after the baseline assessment and was readjusted individually according to individual needs. Participants were also encouraged to maintain these behaviors beyond the duration of the study to ensure maximum benefit and its maintenance over time.
2.4. Endpoints
Arterial function and hemodynamic parameters were obtained through Pulse Wave Analysis (PWA) using a validated AGEDIO device [25–28]. With the participant seated, and after a brief resting period of approximately 5 min, a cuff was placed properly adjusted to the circumference of the arm, in the right upper limb, and the brachial BP was measured by oscillometry, providing the systolic (bSBP), diastolic (bDBP), mean arterial (bMAP) and pulse (bPP) brachial pressures, as well as the Heart Rate (HR). Immediately after the measurement of the brachial BP, the device reinflated the cuff up to the level of the bDBP, maintaining this level for about 10 s, continuously recording the brachial pulse waves with a high-fidelity pressure [26,27]. The bSBP and bDBP were used to calibrate pulse waves. Next, the device software HMS, version 5.1 (IEM GmbH, Stolberg, Germany) applied a generalized transfer function, the ARCSolver algorithm, to reconstruct the aortic pulse wave [25–28]. A wave separation analysis was implemented to decompose the aortic pulse wave into the anterograde (incident) and retrograde (reflected) pulse wave. This information, together with the characteristic impedance, age and gender, made it possible to determine the oscillometric Pulse Wave Velocity (PWV). After a signal quality analysis, the fundamental parameters derived from the PWA were obtained, including: aortic BP (aSBP, aDBP, aPP and aMAP); oscillometric PWV, which was estimated based on aortic pulse wave reconstruction based on characteristic impedance and age, and assuming a three-element Windkessel [25,26]; the augmentation pressure (AugmP), Augmentation index (AIx) and the HR corrected augmentation index (AIx@75), measures of the aortic SBP augmented component and dependent on the timing of the reflected wave; the Total Vascular Resistance (TVR), derived from the ARCSolver algorithm. Arterial stiffness was classified as abnormal according to the available reference values [29] as a PWV value two standard deviations above the PWV reference value adjusted for age and gender [29,30].
Transthoracic Echocardiography (TTE) was performed in all individuals using a VIVID 1 (GE Healthcare, Chicago, IL, USA) and a 1.7/3.4 MHz probe by the same experienced operator. The complete TTE examination was performed, with standard measurements, complying with the measurements according to international recommendations [31–33]. The measurements were recorded in three cardiac cycles. With the probe in parasternal position, in two-dimensional, long axis, the values of the interventricular septum, Left Ventricular (LV) posterior wall and LV dimensions were collected. The measurements were made according to the recommendations [31–33]. The four- and two-chamber apical measurements allowed the analysis of the LV and Left Atrium (LA) base volumes. The LA was evaluated using the modified Simpson method and corrected to the body surface. Simpson’s method was applied to evaluate the LV Ejection Fraction (EF) and Deveraux’s formula was applied to the LV mass. The combination of the LV Doppler method, the LV area and the time–speed integral of the LV, allowed for the calculation of the Stroke Volume (SV) of the participants. In the four-chamber apical, the pulse wave Doppler was used to determine the diastolic filling velocities (E and A), the EA ratio and the deceleration time of the E wave. The tissue Doppler image of the mitral valve was made through a septal and lateral section from which the mean values obtained corresponded to the diastolic velocity of the ring (′), and the left side Ee′ ratio, the LV filling pressure was evaluated. The diameters of the ascending thoracic aorta were measured two to three centimeters above the aortic valve. The dimensions of the aortic arch and descending aorta were measured through a suprasternal window [31–33].
Ventricular-arterial coupling reflects the matching between the arterial system and the LV, was expressed as the ratio of arterial elastance (Ea) to LV elastance (Elv) [33]. The Ea is an integrated index of net arterial load that is imposed to LV work and Elv is an index of contractility and systolic stiffness of myocardium. The matching of both elastances provides greater cardiovascular efficiency and optimal transfer of blood from the LV to the Aorta, thus maintaining BP, LV pressure and Cardiac Output (CO) in a physiological range at the highest myocardial energetic efficiency [34]. A VAC of 1 reflects the perfect balancing between the Ea and the Elv [33]. The non-invasive assessment of Ea and Elv was determined using End Systolic Pressure (ESP) derived from the arterial waveform using the AGEDIO device (as previously described), and the End Systolic Volume (ESV) of the LV and the SV, obtained from the Echocardiogram (as described earlier). Table 1 indicates the main equations applied to derive the VAC parameters and other hemodynamic data of interest.
| Ventricular-arterial coupling | Ea/Elv |
| Arterial elastance | ESP/SV |
| Ventricular elastance | ESP/ESV |
| Stroke work | ESP × SV |
| Potential energy | ESP × ESV/2 |
Formulas for calculating ventricular-arterial coupling and relevant hemodynamic endpoints
2.5. Statistical Analysis
The data was computerized and compiled in a database built in the Excel 2016 program (Microsoft Office, Redmond, WA, USA) and then imported and statistically analyzed in the SPSS program version 24 (IBM, Armonk, NY, USA).
Categorical variables were reported as frequency and percentages, and the χ2 test or the Fisher’s exact test were used when appropriate. Continuous variables were presented as mean and Standard Deviation (SD). The Mann–Whitney U-test was used for comparisons between groups related to continuous variables in the first evaluation. A mixed two-factor ANOVA was used to evaluate the changes in the variables between the first and second evaluations in each and between groups. Greenhouse–Geisser correction was used when sphericity was violated, and Bonferroni’s adjustment for the degrees of freedom was adopted in multiple comparisons to locate the significant effects of a factor. Comparisons between groups in the second evaluation were based on an additional ANCOVA, adjusting the comparison to the baseline values (covariable in the model).
A value of p < 0.05 was defined as a criterion of statistical significance for a 95% confidence interval. The magnitude of the effects was assessed by the value of
3. RESULTS
The study enrolled 21 elderly individuals, aged between 65 and 94 years. The main characteristics of the studied population are shown in Table 2. It should be noted that no statistically significant differences were identified between the groups. Participants had a low average literacy. Smoking habits were present in just one case. About 76.2% of the participants in the study reported a family history of cardiovascular disease. Arterial hypertension, was found in 85.0% of the participants, 71.4% of them were undergoing pharmacological therapy. Dyslipidemia was found in 61.7% of participants in the study. No major heart abnormalities were identified in the cardiac ultrasonography, except for some mild heart valve abnormalities associated with ageing. No significant clinical or demographic differences were observed comparing both groups. No changes in on-going pharmacological treatment were made during the study period.
| Variables | Group 1 (n = 10) | Group 2 (n = 11) | p-value |
|---|---|---|---|
| Age (years) | 81.7 ± 7.4 | 80.5 ± 9.8 | 0.973 |
| Weight (kg) | 66.3 ± 13.5 | 67.0 ± 12.5 | 0.918 |
| BMI (kg/m2) | 28.5 ± 4.0 | 27.7 ± 3.9 | 0.468 |
| Gender | |||
| Male, n (%) | 38.1 (8) | 28.6 (6) | 0.361 |
| Female, n (%) | 9.5 (2) | 23.8 (5) | 0.361 |
| Dry lean mass (%) | 21.5 ± 5.8 | 23.0 ± 5.4 | 0.631 |
| Body fat mass (%) | 26.0 ± 7. 7 | 24.4 ± 9.2 | 0.436 |
| MNA | 22.6 ± 4.1 | 22.9 ± 3.7 | 0.941 |
| Handgrip strength (kg/F) | 14.5 ± 4.0 | 13.4 ± 5.6 | 0.557 |
| Self-efficacy for exercise | 10.5 ± 2.9 | 9.4 ± 4.3 | 0.705 |
| bSBP (mmHg) | 147.2 ± 26.3 | 150.5 ± 23.5 | 0.762 |
| bDBP (mmHg) | 78.0 ± 14.6 | 83.6 ± 18.3 | 0.455 |
| bMAP (mmHg) | 109.6 ± 17.9 | 114.2 ± 19.6 | 0.583 |
| bPP (mmHg) | 69.2 ± 20.7 | 67.0 ± 14.7 | 0.781 |
| HR (bpm) | 71.6 ± 10.3 | 71.6 ± 13.8 | 0.992 |
| EPR | 0.3 ± 0.4 | 0.3 ± 0.1 | 0.557 |
| EDV (cm3) | 134.2 ± 41.3 | 147.0 ± 36.0 | 0.512 |
| ESV (cm3) | 47.0 ± 14.2 | 57.2 ± 19.0 | 0.349 |
| EF (%) | 61.3 ± 3.0 | 60.8 ± 5.6 | 0.152 |
| TAPSE (mm) | 19.8 ± 1.5 | 19.0 ± 2.2 | 0.319 |
| LA area (cm2) | 15.9 ± 6.9 | 12.5 ± 1.7 | 0.426 |
| RA area (cm2) | 12.8 ± 4.5 | 10.3 ± 0.9 | 0.282 |
| cLVM (g/m2) | 82.0 ± 16.3 | 88.9 ± 13.9 | 0.223 |
BMI, body mass index; MNA, mini nutritional assessment; bSBP, brachial systolic blood pressure; bDBP, brachial diastolic blood pressure; bPP, brachial pulse pressure; bMAP, brachial mean arterial pressure; cLVM, corrected left ventricle mass; HR, heart rate; EPR, relative thickness of the left ventricle wall; EDV, end diastolic volume; ESV, end systolic volume; EF, ejection fraction; TAPSE, tricuspid annular plane systolic excursion; LA area, left atrium area; RA area, right atrium area.
Baseline characteristics of the participants
The effect of exercise program on bBP and central BP is depicted for both groups in Table 3. As shown, no significant differences were observed between-groups regarding the baseline for all considered variables. Post-intervention BP significantly decreased only in Group 2, particularly bSBP. No significant differences were found between-groups at baseline and after the intervention, although a significant decrease in Central SBP (cSBP) was observed in Group 2, with cSBP reducing from 135.5 ± 21.2 at baseline to 122.4 ± 18.0 after the intervention program (p = 0.002).
| Variables | Group 1 (n = 10) | Group 2 (n = 11) | p-value |
|---|---|---|---|
| bSBP (mmHg) | |||
| Baseline | 147.2 ± 26.3 | 150.6 ± 23.5 | 0.762 |
| Post-intervention | 137.7 ± 23.3 | 135.6 ± 15.7 | 0.081* |
| Diff. | −9.5 ± 8.0 | −14.9 ± 3.9 | |
| p-value | 0.300 | 0.003 | |
| bDBP (mmHg) | |||
| Baseline | 78.0 ± 14.6 | 83.6 ±18.3 | 0.455 |
| Post-intervention | 76.6 ± 10.4 | 77.1 ± 11.3 | 0.920* |
| Diff. | −1.4 ± 3.7 | −6.5 ± 3.2 | |
| p-value | 0.720 | 0.070 | |
| bMAP (mmHg) | |||
| Baseline | 109.6 ± 17.9 | 114.2 ±19.6 | 0.583 |
| Post-intervention | 104.5 ± 15.0 | 107.7 ± 16.0 | 0.640* |
| Diff. | −5.1 ± 5.4 | −6.5 ± 3.4 | |
| p-value | 0.370 | 0.090 | |
| bPP (mmHg) | |||
| Baseline | 69.2 ± 20.7 | 67.0 ± 14.7 | 0.781 |
| Post-intervention | 61.1 ± 18.5 | 58.6 ± 11.9 | 0.710* |
| Diff. | −8.1 ± 7.9 | −8.5 ± 4.3 | |
| p-value | 0.330 | 0.080 | |
| HR (bpm) | |||
| Baseline | 71.6 ± 10.3 | 71.6 ± 13.8 | 0.992 |
| Post-intervention | 71.9 ± 12.9 | 77.0 ± 12.0 | 0.360* |
| Diff. | 0.3 ± 2.6 | 5. 5 ± 3. 8 | |
| p-value | 0.910 | 0.180 | |
| cSBP (mmHg) | |||
| Baseline | 128.9 ± 20.7 | 135.5 ± 21.2 | 0.483 |
| Post-intervention | 123.4 ± 20.8 | 122.4 ± 18.0 | 0.900* |
| Diff. | −5.5 ± 1.0 | −13.1 ± 3.1 | |
| p-value | 0.380 | 0.002 | |
| cDBP (mmHg) | |||
| Baseline | 79.8 ± 14.7 | 85.0 ± 19.1 | 0.496 |
| Post-intervention | 78.2 ± 9.7 | 80.2 ± 12.0 | 0.680* |
| Diff. | −1.6 ± 3.8 | −4.8 ± 3.7 | |
| p-value | 0.680 | 0.220 | |
| cPP (mmHg) | |||
| Baseline | 49.2 ± 13.1 | 50.4 ± 12.8 | 0.839 |
| Post-intervention | 45.1 ± 15.9 | 42.2 ± 11.7 | 0.630* |
| Diff. | −4.1 ± 5.0 | −8.2 ± 4.3 | |
| p-value | 0.430 | 0.090 | |
ANCOVA results. bSBP, brachial systolic blood pressure; bDBP, brachial diastolic blood pressure; bMAP, brachial mean arterial pressure; bPP, brachial pulse pressure; HR, Heart rate; cSBP, central systolic blood pressure; cDBP, central diastolic blood pressure; cPP, central pulse pressure.
Variation in brachial and aortic blood pressure endpoints from baseline to post-intervention
Considering the changes in the main hemodynamic endpoints, depicted in Figure 1, Group 2 presented a significant reduction in Stroke Work (SW) after the intervention, as well as an increase in the VAC parameter and in the LVwe. Also, oscillometric PWV was reduced in Group 2 after the intervention. No significant changes were observed in Group 1 in any of the considered parameters.
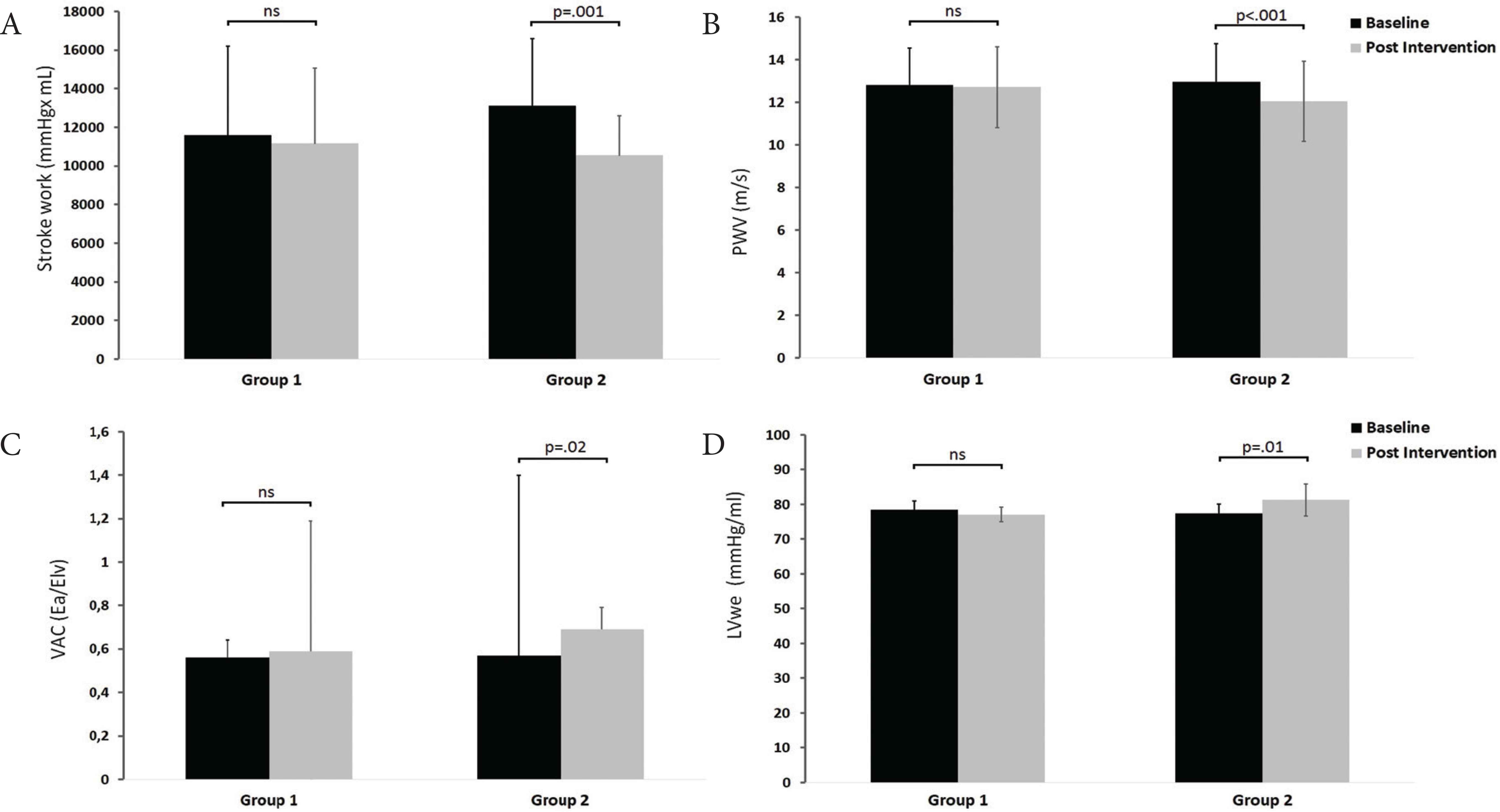
Hemodynamics changes from baseline to post-intervention for Group 1 (without exercise) and Group 2 (with exercise), in (A) Stroke work (SW), (B) pulse wave velocity (PWV), (C) ventricular-arterial coupling (VAC) and (D) left ventricular efficiency (LVwe). ns, non-significant.
Other additional hemodynamic endpoints showed a similar trend from baseline to post-intervention, with significant improvements being observed in Group 2, particularly in the AugmP, the PE and the PVA, with no significant variations observed in any parameter in Group 1 (cf. Table 4).
| Group 1 (n = 10) | Group 2 (n = 11) | p-value | |
|---|---|---|---|
| AIx (%) | |||
| Baseline | 25.5 ± 15.1 | 32.2 ± 12.8 | 0.286 |
| Post-intervention | 26.5 ± 11.9 | 26.6 ± 14.0 | 0.990* |
| Diff. | 1.0 ± 2.9 | −5.6 ± 2.3 | |
| p-value | 0.740 | 0.350 | |
| AugmP (mmHg × ml) | |||
| Baseline | 14.1 ± 7.0 | 18.6 ± 9.7 | 0.246 |
| Post-intervention | 14.4 ± 9.4 | 11.6 ± 7.2 | 0.460* |
| Diff. | 0.3 ± 1.5 | −6.9 ± 1.7 | |
| p-value | 0.850 | 0.002 | |
| Ea (mmHg × ml) | |||
| Baseline | 1.7 ± 0.5 | 1.38 ± 0.4 | 0.145 |
| Post-intervention | 1.5 ± 0.4 | 1.56 ± 0.4 | 0.510* |
| Diff. | −0.2 ± 0.1 | 0.18 ± 0.1 | |
| p-value | 0.030 | 0.060 | |
| Elv (mmHg × ml) | |||
| Baseline | 3.1 ± 1.0 | 2.5 ± 0.8 | 0.180 |
| Post-intervention | 2.5 ± 0.8 | 2.3 ± 0.7 | 0.550* |
| Diff. | −0.6 ± 0.2 | −0.2 ± 0.1 | |
| p-value | 0.040 | 0.210 | |
| PE (mmHg × ml) | |||
| Baseline | 3140 ± 1177 | 3814 ± 1132 | 0.197 |
| Post-intervention | 3303 ± 1066 | 3373 ± 889 | 0.870* |
| Diff. | 163 ± 306 | −441 ± 140 | |
| p-value | 0.610 | 0.010 | |
| PVA (mmHg × ml) | |||
| Baseline | 14741 ± 5732 | 16921 ± 4399 | 0.338 |
| Post-intervention | 14466 ± 4891 | 12996 ± 2518 | 0.390* |
| Diff. | −276 ± 1158 | −3925 ± 663 | |
| p-value | 0.820 | <0.001 | |
ANCOVA results. AIx, augmentation index; AugmP, augmentation pressure; Ea, arterial elastance; Elv, left ventricular elastance; PE, potential energy; PVA, ventricular pressure–volume area.
Variation in hemodynamic endpoints from baseline to post intervention
Table 5 depicts the changes in handgrip strength, a marker of frailty of the elderly, their perception of exercise capacity, and the nutritional status. A statistically significant improvement was observed from the baseline to the post intervention, only in the group with the tailored physical exercise component in the intervention plan (Group 2), translating into a better overall functional profile of these elder participants.
| Group 1 (n = 10) | Group 2 (n = 11) | p-value | |
|---|---|---|---|
| Handgrip strength (kg/F) | |||
| Baseline | 14.5 ± 4.0 | 13.4 ± 5.9 | 0.600 |
| Post-intervention | 13.7 ± 5.8 | 17.8 ± 6.4 | 0.320* |
| Diff. | −0.8 ± 0.8 | 4.5 ± 1.4 | |
| p-value | 0.341 | 0.009 | |
| Self-efficacy for exercise | |||
| Baseline | 10.5 ± 2.9 | 9.4 ± 4.3 | 0.490 |
| Post-intervention | 12.6 ± 2.7 | 14.2 ± 4.6 | 0.090* |
| Diff. | 2.1 ± 1.1 | 4.8 ± 1.3 | |
| p-value | 0.099 | 0.005 | |
| MNA | |||
| Baseline | 22.69 ± 3.70 | 21.23 ± 3.52 | 0.885 |
| Post-intervention | 24.25 ± 1.93 | 23.17 ± 3.52 | 0.409* |
| Diff. | 1.56 ± 1.97 | 1.93 ± 2.77 | |
| p-value | 0.060 | 0.017 | |
ANCOVA results. MNA, mini nutritional assessment.
Indicators of frailty, perceived exercise capacity and nutritional state
4. DISCUSSION
Research on the health benefits of physical exercise, particularly in the elderly, has been a concern of many researchers in recent years [8–15,35–37]. This study aimed at studying the effect of physical exercise on cardiac efficiency in the elderly, using the data obtained in the AGA@4life intervention program [4], which intended to promote active and healthy ageing through a multidisciplinary approach focused on the individual needs, thus aiming to enhance health and well-being. This program is founded on a multidisciplinary approach of ageing, addressing it in a systematic method and covering aspects such as functional capacity, risk of falling, comorbidity (e.g. cardiovascular, cardiorespiratory, metabolic and osteoarticular diseases), cognition, quality of life and mood, polypharmacy, nutrition, environmental and daily context, social support and personal expectations regarding the care provided, among others.
The relevance of physical exercise in the elderly has been extensively described, and guidelines are available to mediate the proper prescription of exercise according to age and associated comorbidities [8,35,36,38]. Previous research highlighted the benefits of exercise in the elderly. Rikli and Jones [36] suggested a battery of tests that assessed physical fitness in the elderly, through tasks of daily living. Subsequently, in 2008, Taylor and Johnson [35] relied on research carried out to date to develop a grid of the benefits of regular physical exercise in the elderly. This is divided into three areas: physiological, functional and other benefits associated with concomitant pathologies. It is important to highlight the emphasis they place on the improvement of cardiovascular capacity, muscle vascularization, blood circulation, increased tolerance for submaximal activities and higher heart rates associated with the practice of exercise.
In our study, we observed a significant positive impact of a tailored physical exercise program on the cardiovascular profile of the elderly, especially concerning cardiovascular efficiency. In fact, significant differences between the Group 1 and 2, composed of participants who participated on more than 95% of the physical exercise sessions, were observed in several hemodynamic parameters. Regarding BP (brachial and central), there was a significant reduction in pSBP and cSBP only in Group 2. Also, the AIx and the AugmP both diminished significantly with exercise. Vascular modulation associated with physical exercise induced changes in the interaction of LV with the aorta, as measured by VAC, as previously demonstrated [39]. The significant improvement of this parameter observed in Group 2 indicates a better coupling of the LV with the aorta, contributing to an optimization of the performance of the LV, thus improving the SW, decreasing the energy expenditure, and translating into an overall better energy efficiency in LV mechanics [14–16,34,39]. The changes in the LVwe parameter is also in line with this positive modulation of cardiac efficiency provided by physical training in the elderly, emphasizing the improvement in cardiac performance. According to Chantler et al. [34] optimal values for the evaluation of cardiac efficiency indexed to the VAC parameter range from 0.7 to 1.0. The post-intervention results in Group 2 reveal an average VAC of 0.69 ± 0.10, representing a significant shift of the heart-to-vessel coupling into a more favorable hemodynamic profile. This was not observed in Group 1, in which the final VAC remained out of the optimal range (0.59 ± 0.60).
The positive modulation provided by physical exercise is in line with previous research, such as the one published by Carrick et al. [13], in which the continuous performance of physical exercise throughout life positively influenced VO2max, SW, systemic O2 extraction and VAC in a large cohort. Other researchers [13–16,34,37] have previously observed similar improvements, initially in animal models with invasive procedures, and later in humans relying on non-invasive methodologies. It is also important to highlight the statistically significant increase observed in Group 2 in the handgrip strength, a recognized marker of frailty in the old adult, and also in the perceived self-efficacy for exercise, which corresponds to an objective indicator of improved self-efficacy capacity for exercise, highlighting not only cardiovascular improvements, but also better overall functional capacity.
Our results provide added evidence in favor of physical exercise intervention, with the particularity of documenting cardiovascular benefits under a tailored approach, in which aspects such as the type of exercise, as well as its frequency, duration and load are adjusted continuously according to each individual needs and functional capacity gains. Further, this personalized approach also considers each individual expectations and motivation on a daily basis, aiming at maintaining the engagement of the individual with the program and promoting active lifestyles beyond the supervised activities. The results highlight the importance of multidisciplinary actions in the promotion of active and independent living, supporting the availability of support and proximity structures included in the healthcare system to meet the old adult necessities in a systematic and comprehensive approach.
This study had limitations that should be considered, among which we highlight the small number of participants, which is a significant aspect, although the results are consistent for the most important endpoints considered in the analysis. Information on the VAC can be found in several studies, but none addressed the effect of a personalized exercise intervention program in old populations, hence the innovative character of this study must be highlighted. Also, a longer follow-up would add relevant information concerning the long-term benefits of the intervention program.
5. CONCLUSION
As a conclusion, the present pilot study showed that tailored exercise prescribed and supervised by competent professionals provides cardiovascular benefits in the elderly, enhancing the coupling of the heart and arterial system, positively modulating the overall hemodynamic profile of the old adult, improving the functional capacity and strength and contributing to a better quality of life. Large randomized trials are needed to further validate these findings.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
TP designed and managed the study, analyzed and interpreted the data, and draft the manuscript. IC implemented the training protocols during the study, contributed to the analysis and interpretation of the data, and contributed in the writing of the manuscript. JC performed the heart ultrasound examinations, collaborated in the interpretation of the results and contributed in the writing of the manuscript. All authors read and approved the final manuscript.
FUNDING
This work is co-financed by the
ACKNOWLEDGMENTS
We acknowledge the contribution of all members of the AGA@4life consortium, including Anabela Martins, Maria Helena Loureiro, Armando Caseiro, Carla Silva, Rute Santos, Marina Saraiva, Tatiana Costa, Ana Ferreira, Jorge Conde, Paula Fonseca, Ana Paula Amaral, Clara Rocha, Joana Ramos.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Ethics Committee of the Polytechnic Institute of Coimbra. The anonymity and confidentiality of the collected data were guaranteed. The study has strictly scientific objectives, with no conflicts of interest to declare. All participants signed an informed consent form.
ABBREVIATIONS
- aDBP,
aortic diastolic blood pressure;
- AIx,
augmentation index;
- aMAP,
aortic mean arterial pressure;
- aPP,
aortic pulse pressure;
- AS,
arterial stiffness;
- aSBP,
aortic systolic blood pressure;
- AugmP,
augmentation pressure;
- bDBP,
brachial diastolic blood pressure;
- bMAP,
brachial mean arterial pressure;
- BMI,
body mass index;
- BP,
blood pressure;
- bPP,
brachial pulse pressure;
- bSBP,
brachial systolic blood pressure;
- CANTAB,
Cambridge Neuropsychological Test Automated Battery;
- CO,
cardiac output;
- DBP,
diastolic blood pressure;
- Ea,
arterial elastance;
- EF,
ejection fraction;
- Elv,
left ventricle elastance;
- ESP,
end systolic pressure;
- ESV,
end systolic volume;
- HR,
heart rate;
- LA,
left atrium;
- LV,
left ventricle;
- LVwe,
left ventricle efficiency;
- MAP,
mean arterial pressure;
- PP,
pulse pressure;
- PWA,
pulse wave analysis;
- PWV,
pulse wave velocity;
- SBP,
systolic blood pressure;
- SD,
standard deviation;
- SV,
stroke volume;
- SW,
stroke work;
- TTE,
transthoracic echocardiography;
- TVR,
total vascular resistance;
- VAC,
ventricular-arterial coupling;
- WHO,
World Health Organization.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Telmo Pereira AU - Inês Cipriano AU - Joaquim Castanheira PY - 2020 DA - 2020/03/02 TI - Effects of a Personalized Physical Exercise Program in the Ventricular-arterial Coupling of Older Adults. A Pilot Study JO - Artery Research SP - 56 EP - 63 VL - 26 IS - 1 SN - 1876-4401 UR - https://doi.org/10.2991/artres.k.200222.001 DO - 10.2991/artres.k.200222.001 ID - Pereira2020 ER -