
Seroprevalence of Hepatitis B Virus in HIV Tested Positive Patients Accessing Treatment in Specialist Hospital Jimeta
 , Halima Ibrahim2, Halima Isa1
, Halima Ibrahim2, Halima Isa1- DOI
- 10.2991/dsahmj.k.210406.001How to use a DOI?
- Keywords
- Demographic characteristics; rapid diagnostic test; seroprevalence; coinfection; HBsAg; Jimeta
- Abstract
Background: Human Immunodeficiency Virus (HIV) positive patients are likely to be at risk of other infectious pathogens such as Hepatitis B Virus (HBV). HIV and HBV are blood-borne pathogens and are transmitted via intravenous drug use, sexual contact, or mother to child during pregnancy or birth.
Objective: The present study aimed at determining the seroprevalence of HBV infection among HIV infected patients who are on antiretroviral treatments in Specialist Hospital Jimeta.
Methodology: A hospital-based cross-sectional study was conducted among 246 patients from August 2019 to January 2020 at Jimeta Specialist Hospital, Adamawa state, Nigeria. The presence of HBV was detected using DiaSpot Hepatitis B Surface Antigen (HBsAg) kit, whereas demographic data were obtained using a prestructured questionnaire. In the HBsAg detection test, a small quantity of blood was collected using pasture pipette and centrifuge, and then three drops of the plasma were dropped on the test portion of the strip and left for 15 min; the results were then recorded. Data were analyzed using SPSS for Windows version 25.0 and presented in the form of texts, frequency tables, percentage, and graphs; association was assessed using chi-square test, in which p < 0.05 is considered statistically significant.
Results: Out of 246 HIV positive individuals screened for the presence of HBsAg, 27 (11.0%) were positive; 21 (8.6%) were female and six (2.40%) were male. Overall, 14 (51.9%) of the participants are non-educated. The highest prevalence was obtained in the age group of 31–45 years with 16 (59.3%). Moreover, most HIV patients who were HBV positive were single with a prevalence of 15 (55.6%), and 210 (38.7%) have knowledge and understanding of vaccination.
Conclusion and Recommendation: Higher proportions of HIV positive patients are non-educated. Similarly, HIV positive patients who are 30 years or older should always be checked for HBV infection. In particular, HIV positive patients should be screened frequently for the presence of HBsAg during their hospital visit.
- Copyright
- © 2021 Dr. Sulaiman Al Habib Medical Group. Publishing services by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Hepatitis B Virus (HBV) increases the risk of liver diseases and when there is coinfection with Human Immunodeficiency Virus (HIV) that will increase the risk of hepatotoxicity because of frequent use of antiretroviral treatments. They share several routes of transmission as both HIV and HBV spread from person to person in semen, blood, or other body fluids. Globally, approximately 90% of infected patients were infected with HBV, and Hepatitis B Surface Antigen (HBsAg) was detected in the 15% of HIV positive individuals [1]. They both share certain epidemiological characteristics such as their mode of transmission and the population that is at higher risk of infections. The seroprevalence of HBV in those infected with HIV ranges between 6.3% and 39% [2]. Furthermore, chronic hepatitis B mortality rate increases because of HIV and it will progress faster to liver cirrhosis and hepatocellular carcinoma. HIV patients who contacted HBV suffered from low HBsAg seroconversion with high levels of HBV DNA [3].
Hepatitis B virus is endemic in Africa and Asia, where most of the infections occur via perinatal transmission, medical and cultural procedures, and close contact with family members. Regardless of HIV infection, the prevalence of HBV is often close to 15% in both Asia and Africa [4], whereas in Nigeria, several studies have recorded the prevalence of HBsAg to range from 7.5% to 44.7% from one locality to another. In Benin City, Nigeria, the prevalence of HBsAg among children is 10.8% [5]. However, it is expected that the prevalence of HBV in HIV positive patients will vary from one locality to another. The present study is aimed at determining the seroprevalence of HBV in patients who tested positive for HIV and are accessing treatment at Specialist Hospital, Jimeta.
2. MATERIALS AND METHODS
2.1. Study Design
A hospital-based cross-sectional study was conducted among 246 patients from August 2019 to January 2020 at Jimeta Specialist Hospital. The hospital, which has a 474-bed capacity, serves approximately 315–350 patients daily. It is located in Jimeta (latitude: 9°16′27.00″ N; longitude: 12°26′26.99″ E), which has a population of 3,106,585 [6].
2.2. Sample Size
The number of samples collected for the present study was calculated using single mean sample size estimation as described by Naing et al. [7]. The value of p was taken as 0.20, using the following formula introduced by Daniel [8].
Hence, 245.9 samples are required for this study; this number was later approximated to 246 samples.
2.3. Study Population
Venous blood samples were collected from 246 patients with HIV who attended Specialist Hospital Jimeta. Written consent was obtained from participants prior to collection of blood samples for the study. The objectives of the study were also explained to the participants.
2.4. Sample Collection
Samples were collected by the phlebotomist using standard procedures, in which about 5 mL of the venous blood sample was collected aseptically by venipuncture and dispensed into a sterile bottle. The sera were separated by centrifugation at room temperature at 300 rpm for 5 min and taken to the work bench for further processing [9].
2.5. Determination of HBsAg
The HBsAg test strip was used for this analysis, and the test was conducted according to the manufacturer’s instruction. The strip was open and placed on a dry flat surface. A pasture pipette was used to collect a small quantity of the plasma, and three drops of the plasma were then dropped on the test portion of the strip. The strip was left for 15 min; the result was observed and recorded according to the indication of color band on the test region and the control region.
2.6. Demographic Data of Participants
The sociodemographic variables (gender, age, marital status, and educational status) and other associated factors such as knowledge of HBV, history of HBV vaccination, and vaccination status data were collected using a self-administered prestructured questionnaire after written consent was obtained.
2.7. Statistical Analysis
Data were analyzed using SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY, USA) and presented in the form of texts, frequency tables, percentages, and graphs. Association was assessed using chi-square test, and p ≤ 0.05 was considered statistically significant [8].
3. RESULTS
3.1. Gender Distribution of HBV in HIV Positive Patients
The results of the distribution of hepatitis B among HIV positive patients in relation to gender, showed that 27 (11%) of both male and female participants are hepatitis B positive whereas the remaining 219 (89%) are negative. A higher prevalence of HBV and HIV positivity was observed in females (21; 8.6%) than in males (6; 2.4%), as depicted in Table 1.
| Gender | Positive (%) | Negative (%) | Total (%) |
|---|---|---|---|
| Male | 6 (2.4) | 66 (26.9) | 72 (29.4) |
| Female | 21 (8.6) | 153 (62.4) | 174 (71.0) |
| Total | 27 (11.0) | 219 (89.0) | 246 (100) |
Pearson chi-square = 0.387; p = 0.538.
Gender distribution of HBV in HIV-positive patients
3.2. Distribution of HBV in HIV Positive Patients with Respect to Educational Status
Regarding HBV and HIV positivity and educational status of the patients, 92 (37.4%) of patients have secondary school level of education, with one (3.7%) positive case; meanwhile, non-educated patients accounted for 51 (20.7%) among HIV positive patients, of whom 14 (51.9%) were positive (Table 2).
| Educational status | HBV test | Total (%) | |
|---|---|---|---|
| Positive (%) | Negative (%) | ||
| Primary | 2 (7.4) | 56 (25.6) | 58 (23.6) |
| Secondary | 1 (3.7) | 91 (41.6) | 92 (37.4) |
| Tertiary | 10 (37.0) | 35 (16.0) | 45 (18.3) |
| Non-educated | 14 (51.9) | 37 (16.9) | 51 (20.7) |
| Total | 27 (100) | 219 (100) | 246 (100) |
Pearson chi-square = 32.564; p = 0.000.
Distribution of HBV in HIV positive patients versus educational status
As depicted in Figure 1, most HIV positive patients are aware of HBV, and they are interested in taking the HBV vaccine; however, few of them who were included in this study were vaccinated. Moreover, a large number of HIV positive patients were not tested for HBV. Thus, they were also not vaccinated.
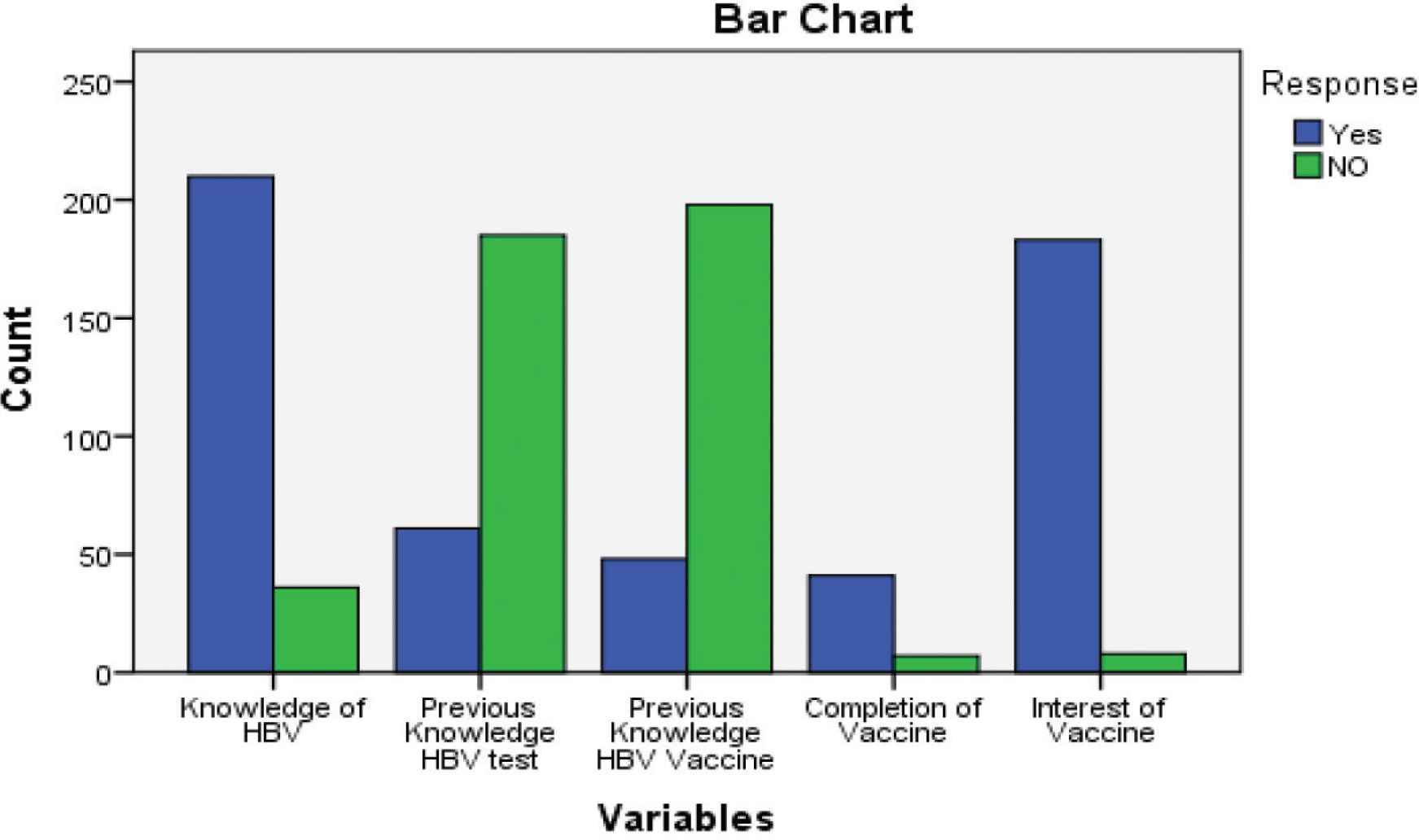
Vaccinated and unvaccinated distribution of hepatitis B virus (HBV) in human immunodeficiency virus (HIV) positive patients.
3.3. Prevalence of HBV among HIV AIDS Patients based on their Age Group
Table 3 gives the prevalence distribution of respondents in relation to age categories. The results indicated that the age group of 31–45 years showed the higher number of HBV coinfections with HIV, at 120 (48.8%), of which 16 (59.3%) were positive coinfections, and the least was found in the age group 1–15 years, with a total of nine (3.7%) coinfected patients with two (7.4%) positive cases.
| Age group (years) | HBV test | Total (%) | |
|---|---|---|---|
| Positive (%) | Negative (%) | ||
| 1–15 | 2 (7.4) | 7 (3.2) | 9 (3.7) |
| 16–30 | 3 (11.1) | 66 (30.1) | 69 (28.0) |
| 31–45 | 16 (59.3) | 104 (47.5) | 120 (48.8) |
| >45 | 6 (22.2) | 42 (19.2) | 48 (19.5) |
| Total | 27 (100) | 219 (100) | 246 (100) |
Pearson chi-square = 5.064; p = 0.167.
AIDS, acquired immunodeficiency syndrome.
Prevalence of HBV among HIV AIDS patients based on age group
3.4. Distribution of HBV in HIV Positive Patients based on Marital Status
Table 4 depicts the result of the distribution of HBV in HIV patients in relation to marital status. The result of the study revealed that coinfection of HBV is higher in HIV positive patients who are single, with 15 (55.6%), whereas lowest were found in widows.
| Marital status | HBV test | Total (%) | |
|---|---|---|---|
| Positive (%) | Negative (%) | ||
| Single | 15 (55.6) | 39 (17.8) | 54 (22.0) |
| Married | 8 (29.6) | 115 (52.5) | 123 (50.0) |
| Divorced | 4 (14.8) | 32 (14.6) | 36 (14.6) |
| Widow | 0 (0.0) | 33 (15.1) | 33 (13.4) |
| Total | 27 (100) | 219 (100) | 246 (100) |
Pearson chi-square = 22.188; p = 0.000.
Distribution of HBV in HIV positive patients based on marital status
3.5. Distribution of HBV in HIV Positive Patients in Relation to Vaccination Status
Table 5 shows that 210 (85.4%) of the respondents have knowledge of HBV infection as well as its vaccine. Among 61 (24.8%) respondents who are aware of the HBV test, 48 (19.5%) were vaccinated, of whom about 41 (16.7%) have completed their vaccination.
| Variables | Yes (%) | No (%) | Total (%) |
|---|---|---|---|
| Knowledge of HBV | 210 (85.4) | 36 (14.6) | 246 (100) |
| Are you aware of HBV test? | 61 (24.8) | 185 (75.2) | 246 (100) |
| Are you vaccinated? | 48 (19.5) | 198 (80.5) | 246 (100) |
| Completion of vaccination | 41 (16.7) | 205 (83.3) | 246 (100) |
| Interest of vaccination | 183 (74.4) | 63 (25.6) | 246 (100) |
Pearson chi-square = 454.967; p = 0.000.
Distribution of HBV in HIV positive patients in relation to vaccination status
4. DISCUSSION
The present study revealed that the overall prevalence of HBV among HIV positive patients is 27 (11.0%). This indicates that some HIV positive patients who were receiving antiretroviral therapy in specialist hospital Jimeta are also infected with HBV. A similar prevalence was reported from previous studies carried out in different parts of Nigeria. For example, Hamza et al. [10] observed a prevalence rate of 12.5% of HBV in HIV positive patients in tertiary hospitals in Northwestern Nigeria. Meanwhile, Otegbayo et al. [11] observed a prevalence of 11.9 in Ibadan; Adewole et al. [12] reported 11.5% in Abuja, and Lar et al. [13] reported 11.8% in Jos. Reports of HBV in HIV positive patients within and outside Nigeria suggested that the situation of coinfection of HBV in HIV positive patients is not affected by environment [14]. Perinatal and early childhood serves as major routes in which HBV is transmitted in countries with immediate and high HBV endemic areas; the infection rate of HBV in HIV positive patients ranges from 10% to 20%, and this is slower than 10–70% in observed in Nigeria [15]. However, lower HBV prevalence, that is, 6.2% and 5.7% was found among HIV positive patients in Tanzania and Brazil, respectively [14].
The highest prevalence of HBV was reported among HIV positive female patients (8.6%) compared with males (2.4%). Similar results were reported among HIV positive patients from a study conducted by Okechukwu et al. [16]. Our results are in line with those reported in another study carried out in Abuja, Nigeria, where large numbers of HIV infected female patients were also found to be infected with HBV [12].
The study observed that most of the HIV positive patients accessing treatments in the study area have knowledge of HBV, but very few of them were tested to check their HBV status. In terms of vaccination, very few of the HIV positive patients have completed their dose of vaccination; this could be a factor that may have increase the prevalence of HBV among HIV positive patients.
In general, as elderly people have lower immunity because of their age, this makes them more susceptible to HBV especially when they are HIV positive. Study respondents within the age group of 31–45 years have the highest percentage distribution of HBV, which could be attributed to their lower immunity as well their lifestyle. A similar study conducted by Okechukwu et al. [16] has observed that HIV patients belonging to the age group of 36–40 years are highly infected with HBV. However, this study suggested that there could be a decrease in HBsAg positivity with age because as HIV patients grow older their immunity also decreases, and they are thus unable to fight off and effectively eliminate most pathogens that get into the body. This could be because many of the infectious pathogens can be flushed out in younger age groups than in older age groups. One of the factors that determine the prevalence and incidence rate of infection is the age of study participants. In the present study, the differences in the prevalence of HBV infection in HIV patients in different age groups indicated that age plays an important role in the prevalence and incidence rate [17].
5. CONCLUSION
The findings of this study showed that HIV positive patients are also affected with HBV, and this is a threat to HIV positive patients. This study has also revealed that there is a higher prevalence of HBV among elderly people than in younger ones, and that this may be a result of the decrease in the level of immunity in older individuals. The rate of infection also suggests the need for a baseline screening for HBV markers in HIV positive patients to reduce and prevent the spread of the disease among HIV patients. Older HIV positive people should be given HBV vaccination because they are at greater risk of the infection.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
All authors contributed to conceptualization and experimental designed of the study. HIs managed literature searches. HI and MB were involved in laboratory experiments and data collection. HI contributed to the analyses of data generated in the study. The manuscript was written by MB and HIs, and was reviewed and approved by all authors.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Mohammed Bashir AU - Halima Ibrahim AU - Halima Isa PY - 2021 DA - 2021/04/14 TI - Seroprevalence of Hepatitis B Virus in HIV Tested Positive Patients Accessing Treatment in Specialist Hospital Jimeta JO - Dr. Sulaiman Al Habib Medical Journal SP - 74 EP - 77 VL - 3 IS - 2 SN - 2590-3349 UR - https://doi.org/10.2991/dsahmj.k.210406.001 DO - 10.2991/dsahmj.k.210406.001 ID - Bashir2021 ER -