
Covid-19 Vaccinated and Positive Rate of Infection in Israel and the United Arab Emirates
 , Sarim Al Zubaidy2
, Sarim Al Zubaidy2- DOI
- 10.2991/dsahmj.k.210427.001How to use a DOI?
- Keywords
- Vaccination; infection; Covid-19; herd immunity
- Abstract
Thanks to the high vaccination rates posted in Israel and the United Arab Emirates since mid-December 2020, by end of March 2021 a significant portion of the population has been vaccinated. This adds to the percentage of those who have been infected and have recovered, protected to a different extent depending on the time of infection. The manuscript tries to understand the effect of vaccinated and previously infected on the number of new cases, based on the available data for the number of cases, tests, vaccines’ doses, and fatalities. The positive effect of vaccinations on the new cases has been masked so far by confounding factors, as it is not evidenced by the proposed data.
- Copyright
- © 2021 Dr. Sulaiman Al Habib Medical Group. Publishing services by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
According to their latest statement [1], the World Health Organization (WHO) supports herd immunity for Covid-19 through vaccination. Herd immunity is achieved when a large share of the population (the herd) develops immunity to a disease, making spreading unlikely [2–5]. The WHO supports herd immunity through vaccination and not infection, because infection would result in unnecessary cases and deaths. How protective are vaccinations or prior infections and for how long is an open question [6–9].
Using Kermack and McKendrick’s [10] simple SIR model (S susceptible, I infected, R removed), vaccination would lower the number of “susceptible” individuals—moving them to the “removed” category, thereby limiting further spread of the virus. To achieve herd immunity, a substantial percentage of the population needs to be vaccinated. The percentage of people that must be vaccinated against Covid-19 for herd immunity is not known [1]. People who have been infected and have recovered are similarly moved from the “susceptible” to the “removed” category. The removal is only temporary, protection against subsequent waves with possibly different strains is unlikely.
The vast majority of the population in most countries is presently susceptible. Seroprevalence results suggest that in general less than 10% of the population has been infected and has recovered from Covid-19 infection. The WHO states that experts do not know how strong or lasting is the immune response developed after Covid-19 infection. How protective are vaccines in limiting the spread of infection or reducing the consequences has yet to be determined with accuracy. The immune response triggered by vaccines or infection may differ for different people. Moreover, viruses are continuously evolving. It is unknown if the immune response to a previous strain, either from infection or a vaccine, can protect against a novel strain, and how protective it is versus the same strain against time. Although antibodies exist after infection, they tend to vanish eventually thus displacing people from the “removed” category back to the “susceptible” column. Protection with vaccines is not perfect. Vaccines so far have been administered in two doses (although one-dose vaccines are now becoming available). With two doses of vaccines, protection after the first dose is expected to be minimal. Protection is better after two doses. Antibodies from vaccines also vanish with time. As we work toward herd immunity, vulnerable groups that cannot get vaccinated should be kept safe from infection. The WHO states that although older people and those with underlying conditions are not the only ones at risk, they are certainly those most at risk. Physical barriers temporarily reduce the number of “susceptible” moving them to the temporarily “removed.”
Regarding the pattern of the outbreak in Israel, several studies have now been reported in the literature. Glied [11] praises the strength of the Israeli healthcare system and the success of vaccine implementation. The author believes that the pattern of the outbreak in Israel is an indication of “the strengths of the Israeli healthcare system facilitated implementation of the roll-out, but the government’s unambiguous prioritization of vaccination drove implementation success.” In the same journal, Rosen et al. [12] also highlight the rapid vaccination undertaken by Israel and note that “as of the end of 2020, the State of Israel, with a population of 9.3 million, had administered more COVID-19 vaccine doses than all countries aside from China, the US, and the UK.” McKee and Rajan [13], also in the same journal, similarly discuss the success of the vaccination campaign in terms of speed to achieve large shares of vaccinated people.
Several studies [14–16] noted that during the vaccination roll-out, which started on December 19, 2020, there has been a dramatic growth in the number of cases in Israel, despite a lockdown implemented around Christmas 2020, which lasted until January 17, 2021; records show that there was a peak of infected cases of 996.17 cases per million, 7 days moving average, and then on January 25, 2021, a peak of fatalities of 7.49 per million was recorded. These peaks were well above the values experienced prior to the first and second waves in Israel, and well above the values of every other country in the Middle East whose health systems were of similar quality.
In particular, two studies [14,16] focused on the efficacy of Covid-19 policies and therapies of the United Arab Emirates (UAE) as assessed in terms of case fatality rate.
Bentout et al. [17] presented a modeling work (in a nonmedical journal) that predicts peak time and the number of infectious cases at the peak prior to and after implementation of nonpharmaceutical interventions. Developed at the very beginning of the pandemic, the computations highlighted the positive effect of restrictions. One of the countries considered is the UAE. Actual patterns of infection have been different, indicating issues with the modeling assumptions.
Meanwhile, Daneshvar et al. [18] presented work that subjectively attempts to correlate some climatic factors, such as upward long-wave radiation flux (ULR), temperature, and CH4 in the UAE and aerosol index and NO2 in Switzerland, with the severity of the outbreak.
The first wave of Covid-19 infection in Israel is discussed by Last [19], who noted that that after the first confirmed cases on February 21, 2020, the cases started to climb. The daily infection rate showed a sharp decrease from the peak value of 1131 down to about 100 new confirmed cases daily on April 30, 2020 thanks to lockdown measures.
This paper aims to provide a first answer to the following questions: For how long will infected and recovered individuals belong to the removed category (which is the susceptibility to infection of those who received one dose of a two-shot vaccine)? How many of those vaccinated belong to the removed category and for how long? How protective are vaccines and prior infections toward new strains? We will try to answer these questions based on the available data for the number of cases, tests, fatalities, and vaccine doses.
2. MATERIALS AND METHODS
Analysis of the time series of the number of cases, tests, positive rate, fatalities, vaccination doses, people having received at least one vaccine dose, and people fully vaccinated in Israel and the UAE, the countries with the largest shares of vaccinated individuals worldwide. These major parameters are proposed by databases such as ourworldindata [20]. The raw data on confirmed cases and deaths are sourced from the COVID-19 Data Repository by the Center for Systems Science and Engineering at Johns Hopkins University (Baltimore, MD, USA) [21]. Regarding vaccines, the data are collated by ourworldindata from public official sources.
3. RESULTS
Countries such as Israel and the UAE had over the past month posted the world’s highest vaccination rates, up to 1.2–1.4% of the total population per day. The percentage of the population that has been vaccinated (February 5, 2021) starts to become significant, and the number is growing fast. This permits a first assessment of the hypothesis of herd immunity by vaccination or infection.
Figure 1 shows the following details for Israel and the UAE: (A) number of new cases (7 days moving average) and cumulative cases per million; (B) number of tests per 1000 people (7 days moving average); (C) the positive rate (share of positive tests); (D) number of new fatalities per million (7 days moving average); (E) new vaccinations’ doses (7 days moving average) and cumulative vaccination doses per 100 people; (F) share of the population that has received at least one dose; and (G) share of the population fully vaccinated.
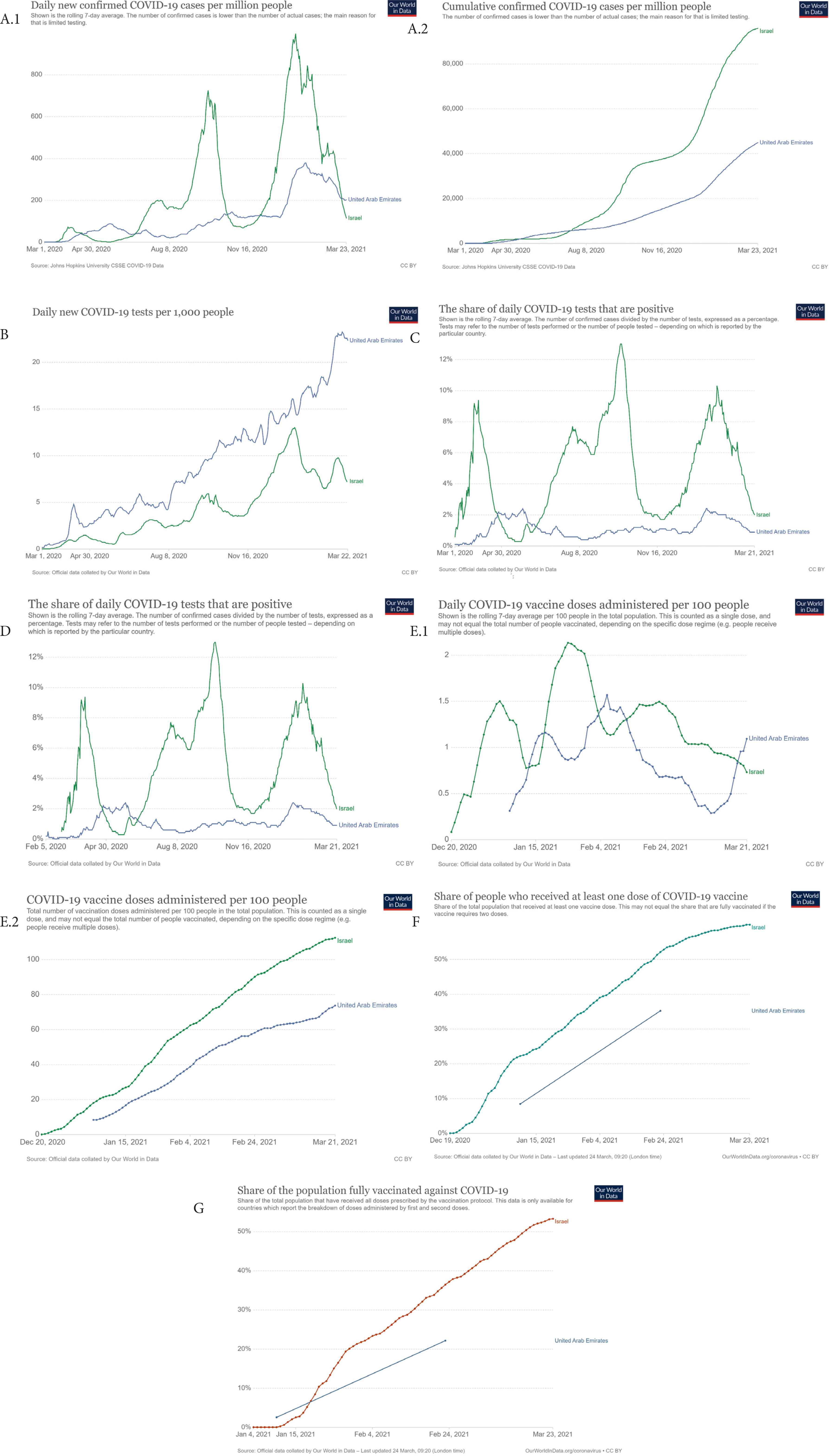
Covid-19 outbreak in Israel and the United Arab Emirates. (A) Number of new cases (7 days moving average) and cumulative cases per million. (B) Number of tests per 1000 people (7 days moving average). (C) Positive rate (share of positive tests). (D) Number of new fatalities per million (7 days moving average). (E) New vaccination doses (7 days moving average) and cumulative vaccination doses per 100 people. (F) Share of the population who received at least one dose. (G) Share of the population fully vaccinated. Data for the United Arab Emirates in (F) and (G) are likely incorrect. Images reproduced modified from ourworldindata.org (accessed on March 24, 2021).
From Figure 1A, about 10% and 4.5% of the population has been infected in Israel and the UAE, respectively. In March 2020, at the beginning of the pandemic, the WHO suggested that 80% could have been mild or asymptomatic [22]. This means that the unreported mild or asymptomatic cases may be at least two to three times the above reported cumulative case percentages. Thus, at present, 20–30% of the population in Israel and 9–13.5% of the population in the UAE have likely been infected.
From Figure 1B and 1C, it is clear that the number of positive cases is not independent of the number of tests. Many countries increase or decrease their testing activities to change the number of new cases. The positive rate is a much better parameter to indicate the severity of an outbreak. The number of cases recently reducing in Israel is only an artifact of the reducing number of tests.
From Figure 1D, the number of new fatalities has been much larger in Israel than in other countries of the Middle East with similar quality health systems such as the UAE. The number of fatalities is trailing the number of new cases with an about 2-week delay. The cumulative case fatality rate is about 0.74% in Israel and a much lower 0.33% in the UAE.
The vaccination numbers for the UAE are incomplete.
From Figure 1E, at a daily vaccination rate of more than 1% of the population per day, a number of vaccine doses about 110% of the population have been administered in Israel, and 80% in the UAE.
From Figure 1F, more than 60% of the population has received at least one vaccination dose in Israel, where almost 55% of the population is fully vaccinated.
4. DISCUSSION
The increasing number of vaccinations in Israel and the UAE has not been associated with a decreasing number of newly infected cases. Since mid-December 2020, the share of positive cases in those tested has been sharply rising in Israel. It has also been increasing, but starting from a much better level, in the UAE, where it is now declining.
Restrictions may affect the positive rate. However, although in the UAE there has been no change during the period of observation, in Israel restrictions have been made more, rather than less, severe.
One possible explanation for the increase of cases in Israel is that vaccinations may have increased the contacts between people in times where the number of infected was not negligible, thus translating into more opportunities for the virus to spread.
Another explanation is that between the two shots people may be more prone to becoming infected. However, this seems true for Israel compared with the UAE. Additional data to better understand the increased vulnerability between the two shots of a two-dose vaccine are minimal. On January 20, 2021, it was reported that thousands of Israelis tested positive for Covid-19 despite receiving the vaccine [23,24]. Overall, 12,400 of 189,000 people (or 6.6%) returned positive. The positive rate in the general population was less, at about 5%. The majority of the 12,400 were infected immediately after the first shots of the two shots vaccine. A total of 1410 individuals tested positive 2 weeks after the first shot. Meanwhile, 69 tested positive after two shots. The number of people tested after two shots is unknown.
Although there is a linear correlation between the positive rate and the number of vaccinations in Israel with high R2, this correlation is purely accidental. No similar correlation is found in the UAE data. As similar recent spikes have been registered in European countries, such as the UK, the growing number of cases in Israel and the UAE is likely the result of a much more infective second wave with a novel virus strain. The increasing number of cases could have been the result of imported cases, as Dubai in particular had borders open to travelers, who are also from highly infected areas, during Christmas and New Year’s Eve.
Vaccinations in Israel started on December 19, 2020. Israel experienced dramatic growth in the number of cases, despite a lockdown implemented starting in Christmas 2020 until January 17, 2021; a 7 days moving average peak of infected cases of 996.17 cases per million, and then on January 25, 2021, a 7 days moving average peak of fatalities of 7.49 per million were recorded. These peaks were well above the values experienced prior to the first and second waves in Israel, and well above the values of every other country in the Middle East with similar quality health systems. The UAE had a 7-day moving average peak of 378.49 on January 29, 2021, without any lockdown. Containment of peak has been achieved in Israel mostly by lockdown, imposed well before Christmas 2020, and not because of the vaccinations. Dubai has been open for business since July 2020. The slower falling phase in the UAE is better explained by the lack of a lockdown than the slower vaccination rate, as well as the much lower peak. Epidemic waves are always characterized by peaks, that is, a sequence of growth and falling phases. Attribution of the falling phase in Israel (or the UAE) to the progress of the vaccination campaign is at this stage a very subjective interpretation of the time series. The number of positive cases in Israel is at present less than that in the UAE only as an artifact of the much smaller number of tests. Israel is presently conducting less than one-third of the tests of UAE per 100 people. The positive rate is still higher, more than double. The second wave of Covid-19 in Israel had about the same duration as the latest, ongoing third wave, and it was characterized by a much sharper falling phase.
The Spanish flu [25] lasted from February 1918 to April 1920. It was characterized by the first wave of early 1918, the most deadly second wave of late 1918. The third wave of 1919 was less deadly than the second wave but more severe than the first wave. The fourth wave of 1920 had a much smaller impact. Similarity with the Spanish flu make plausible another wave at the end of this year, and then a mild infection beginning of 2022, following the natural evolution of the virus. Vaccines could spare Israel and the UAE from more severe outcomes from the epidemic in the last half of this year and the first half of the new year.
5. CONCLUSION
Continuous monitoring of the pandemic evolution across the world is of paramount importance to define policies and strategies aimed at the solution of the crisis.
The number of vaccination doses has reached a significant percentage of the population in Israel and the UAE. The positive rate (share of infected between tested) has been growing in Israel at an accelerated rate, rather than reducing. Conversely, in the UAE, it has been growing, and then it started to decline. There are certainly many confounding factors preventing clarification of the effects of vaccines and prior infections on novel infections from the available data.
At the present vaccination rate, it is projected that almost the total population will get vaccinated in these two countries by the beginning of spring.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
AB analysed the data and write the first draft of the manuscript. AB and SA discussed the data, and equally contributed to the writing of the final version of the manuscript.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Alberto Boretti AU - Sarim Al Zubaidy PY - 2021 DA - 2021/05/02 TI - Covid-19 Vaccinated and Positive Rate of Infection in Israel and the United Arab Emirates JO - Dr. Sulaiman Al Habib Medical Journal SP - 78 EP - 82 VL - 3 IS - 2 SN - 2590-3349 UR - https://doi.org/10.2991/dsahmj.k.210427.001 DO - 10.2991/dsahmj.k.210427.001 ID - Boretti2021 ER -