
Hepatic Artery Aneurysm in Granulomatosis with Polyangiitis
- DOI
- 10.2991/dsahmj.k.211108.001How to use a DOI?
- Keywords
- Hepatic aneurysm; granulomatosis with polyangiitis; embolization
- Abstract
Large vessel involvement and arterial aneurysms are not typically encountered in Granulomatosis with Polyangiitis (GPA), which is a small vessel disease. We report the case of a 70-year-old male presenting with a ruptured hepatic artery aneurysm and elevated Antineutrophil Cytoplasmic Autoantibody, Cytoplasmic (c-ANCA) titer, 9 months after the diagnosis of GPA, while on maintenance therapy with rituximab. The liver aneurysm was successfully treated with coiling and reintroduction of prednisone. Large and medium vessel aneurysms can be seen in the context of GPA, which warrants a low threshold for screening and prompt intervention to prevent life-threatening rupture.
- Copyright
- © 2021 Dr. Sulaiman Al Habib Medical Group. Publishing services by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Systemic vasculitides are a large group of heterogeneous diseases affecting the blood vessels wall. Among them, Granulomatosis with Polyangiitis (GPA; formerly called Wegener’s granulomatosis) is characterized by involvement of the upper and lower respiratory tract with necrotizing granulomatous lesions and the kidneys with rapidly progressive glomerulonephritis [1]. The associated vasculitis involves mainly small- and medium-sized arteries and veins. When inflamed, the blood vessel may become weakened and stretched forming an aneurysm. Aneurysmal formations and involvement of larger arteries are not typically seen in small vessel vasculitis such as GPA. They are pathognomic of medium vessel vasculitis such as Polyarteritis Nodosa (PAN) and Kawasaki disease [1], that do not however present with granulomatous lesions of the respiratory tract nor glomerulonephritis.
We report the case of a 70-year-old man known to have GPA on maintenance therapy with rituximab, presenting with worsening anemia and an incidental finding of a large intrahepatic hematoma related to the rupture of a hepatic artery aneurysm.
To the best of our knowledge, aneurysmal dilatation of the hepatic artery caused by GPA has been reported in only three cases in the literature.
2. CASE REPORT
A 70-year-old obese male with a history of hypertension, atrial fibrillation on oral anticoagulation (warfarin), and benign prostate hypertrophy was admitted at the end of August 2019 for gross hematuria, hemoptysis, lower limbs edema, and intermittent migratory arthralgias for more than 1 month prior to presentation. He was found to have a rapidly progressive glomerulonephritis with a creatinine rising from 1.2 to 6.8 mg/dL within few days, proteinuria of 620 mg/24 h and macroscopic hematuria with dysmorphic red blood cells on urine microscopy. The diagnosis of GPA was established upon this clinical presentation along with the detection of highly positive Antineutrophil Cytoplasmic Autoantibody, Cytoplasmic (c-ANCA) directed against proteinase 3. Kidney biopsy revealed pauci-immune crescentic glomerulonephritis in more than 50% of the glomeruli. The patient received intravenous pulse steroid therapy for 3 days (500 mg methylprednisolone) followed by oral prednisone 1 mg/kg for 6 months and intravenous cyclophosphamide 15 mg/kg. He was concomitantly treated with seven sessions of plasmapheresis, after which we noted a significant improvement in his kidney function with a creatinine nadir of 1.5 mg/dL after 2 weeks of therapy. The induction treatment with cyclophosphamide was continued for a total of six doses, and the maintenance treatment with rituximab 500 mg was started on January 2020.
In May 2020—9 months after the initial diagnosis of GPA and 4 months after his second dose of rituximab—he was admitted for acute prostatitis caused by Escherichia coli (extended spectrum beta lactamase producing). He was hemodynamically stable on presentation, and his initial laboratory workup was notable for mildly elevated liver enzymes and acute anemia. An abdominal ultrasound was performed for further investigation and revealed a large relatively well circumscribed avascular heterogeneous mass in the right lobe measuring 12 × 10.5 cm with no specific characteristics, not present on a previous ultrasound done in November 2019.
Differential diagnoses at that time included anecrotic mass (malignant versus benign), abscess, or hematoma.
An abdominal Magnetic Resonance Imaging (MRI) was done thereafter, revealing a large well-circumscribed heterogeneous liver lesion very likely consistent with a hematoma.
Further workup was obtained including inflammatory markers (C-reactive protein and procalcitonin) and tumor markers [carcinoembryonic antigen, CA 19-9, and alpha-fetoprotein], which were all unremarkable. Echinococcal cyst was ruled out by negative serologies. However, his c-ANCA titer was notably increased from 12 AU (Arbitrary Units)/mL, 2 months after treatment, to >200 AU/mL with a stable creatinine at 1.7 mg/dL and absence of microscopic hematuria, suggestive of quiescent disease. His hemoglobin remained stable at about 9 g/dL.
The patient was discharged home with the presumed diagnosis of a spontaneous liver hematoma of unknown etiology while being kept on oral anticoagulation due to his congestive heart failure, hypertension, age, diabetes, previous stroke/transient ischemic attack–vascular disease, age, sex category score of 2. Oral prednisone therapy was resumed at 0.5 mg/kg/day for maintenance of remission of his GPA. He was advised to get serial hemoglobin checks in the outpatient setting and to report back to the emergency room should he develop any signs of acute bleeding.
A follow-up abdominal MRI was performed a month later showing a slight decrease in the size of the previously seen liver hematoma. In addition, a small (10 mm) focal aneurysmal vascular dilatation was noted adjacent to the mass. These findings suggested that the hematoma could be the result of a ruptured aneurysm. The patient underwent a successful embolization by coiling of the intraparenchymal hepatic artery aneurysm (Figure 1). His hemoglobin progressively improved and was stable at 10.5 g/dL after 3 months.
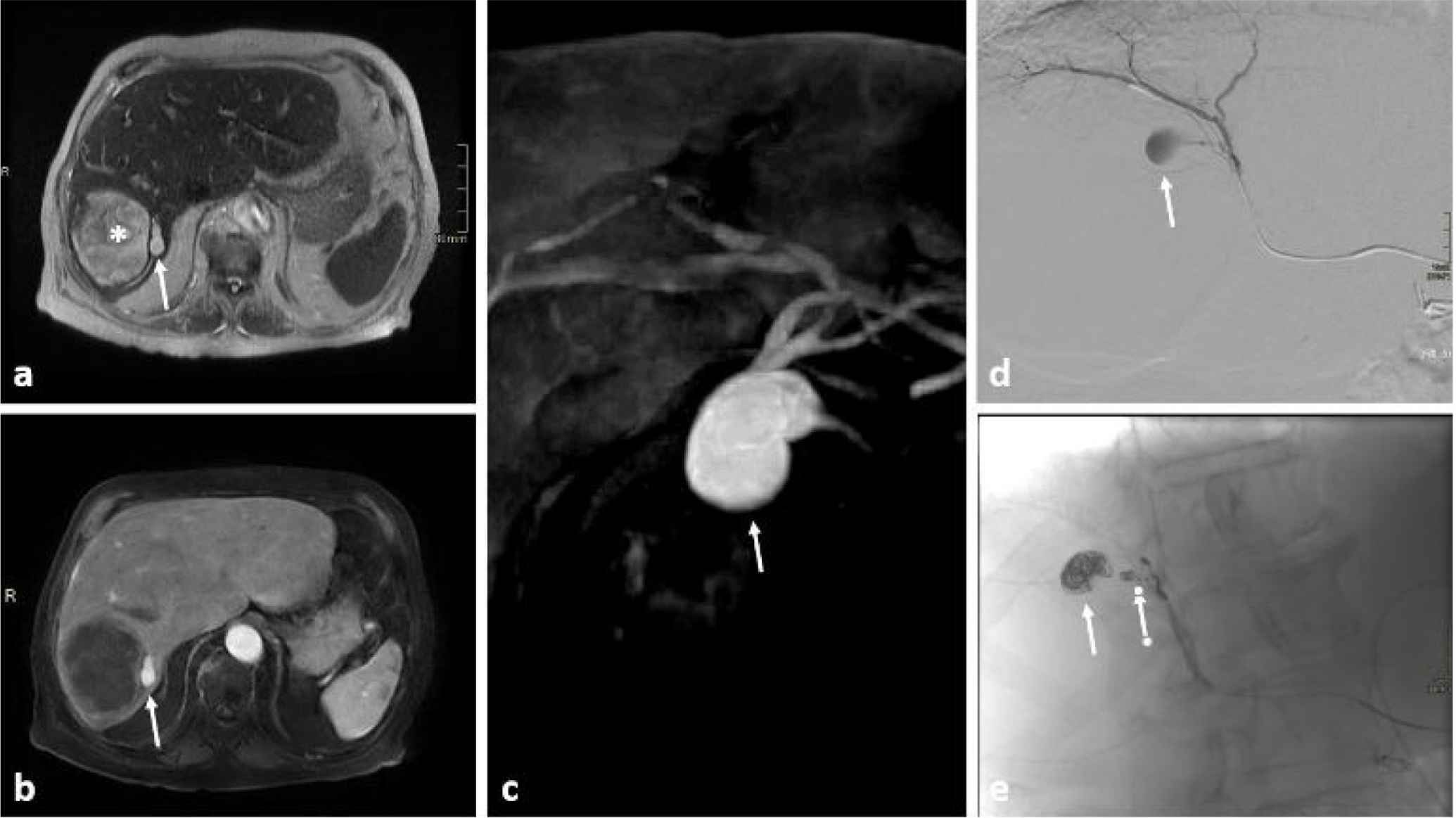
Abdominal MRI sequences (a–c) and arterial hepatic angiography (d and e). Axial T2 image of the midportion of the liver (a) showing a large heterogenous formation between segment VI and VII (asterisk) with an adjacent small ovoid formation of intermediate signal (arrow). The large formation is not enhancing in axial T1 image post contrast injection (b) while the ovoid formation is vividly enhancing on the arterial phase (arrows in b and c) denoting its very probable aneurysmal origin (c: oblique maximal intensity projection reformatting of T1 sequence post contrast administration in the arterial phase). Selective hepatic catheterization and angiography confirming the presence of the aneurysm (arrow in d) that was successfully embolized with its branch by multiple coils (arrows in e).
Oral prednisone was discontinued after 6 months, and he remained on rituximab maintenance therapy. He received his last dose of rituximab in February 2021, at which time his creatinine was stable at 1.7 mg/dL with negative c-ANCA titer. At the time of this report, the patient remains symptom-free with evidence of full clinical remission.
3. DISCUSSION
This case illustrates a hepatic artery aneurysm in a 70-year-old male with GPA while on maintenance therapy, that was complicated by rupture and subsequent large hepatic hematoma.
Only three cases [2–4] of hepatic artery aneurysms were reported in the literature among a total of 19 cases describing medium and large vessel aneurysms related to GPA (Table 1).
| References | Age (years)/sex | Artery | Manifestation | Duration between GPA diagnosis and aneurysm | Therapy | Outcome |
|---|---|---|---|---|---|---|
| Baker and Robinson [1] | 24/male | Intrarenal | Perinephric hematoma | Concomitant | Gel foam embolization; prednisone and cyclophosphamide | Recovery |
| Arlet et al. [2] | 29/male | Branches of hepatic and renal | Abdominal Pain (intestinal ischemia) | 5 years (4 months after severe poorly controlled relapse) | Endovascular coiling with immunosuppressive treatment | Recovery |
| den Bakker et al. [3] | 55/male | Hepatic | Abdominal pain, hemorrhagic shock | Concomitant | Methylprednisolone, cyclophosphamide | Death |
| Shitrit et al. [4] | 58/female | Subclavian | Ischemic hand | 9 days | Thrombolytic therapy, anticoagulation and stent insertion; high dose prednisone and cyclophosphamide | Recovery |
| Carels et al. [5] | 63/male | Aorta | Back pain | Concomitant | Methylprednisolone, surgery | Recovery; relapse after 6 years |
| Famaluro et al. [6] | 67/male | Superior pancreatic—duodenal | Abdominal pain and shock (ruptured aneurysm) | Concomitant | Surgical repair | Death as a result of multiorgan failure |
| Aoki et al. [7] | 56/male | Left gastric | Hemorrhagic shock | Concomitant | Not stated | Death |
| Carron et al. [8] | 79/male | Intrarenal | Incidentally on arteriography | Concomitant | Plasmapheresis, cyclophosphamide and prednisolone | Not stated |
| Durai et al. [9] | 33/male | Aorta | Abdominal discomfort | Concomitant | Surgical repair; prednisolone and cyclophosphamide | Recovery |
| Kim et al. [10] | 71/male | Intrarenal | Incidentally on contrast enhanced US | Concomitant | Cyclophosphamide and steroids | Disappearance of microaneurysms |
| Luebke et al. [11] | 67/male | Superficial femoral | Aneurysm (pulsatile mass) | 5 years | Surgical resection and bypass with graft | Recovery |
| Moutsopoulos et al. [12] | 30/male | Intrarenal | Incidentally on angiography | 4 months | None | Not stated |
| Moutsopoulos et al. [12] | 53/female | Intrarenal | Incidentally on angiography | 1 months | None | Not stated |
| Mozaffar et al. [13] | 49/female | Celiac trunk and superior mesenteric | Abdominal pain | 2 years | Surgical bypass grafting; methylprednisolone and cyclophosphamide | Recovery |
| Musuruana et al. [14] | 25/male | Coronary | Myocardial infarct | Concomitant | Steroids with cyclophosphamide | Resolving of aneurysms |
| Senf et al. [15] | 35/male | Renal, splanchnic and hepatic | Hemorrhagic shock | 24 days | Supportive therapy | Not stated |
| Takei et al. [16] | 34/male | Anterior choroidal | Subarachnoid hemorrhage | One month prior to diagnosis | Clipping surgery | Recovery |
| Tomosugi et al. [17] | 57/male | Accessory left gastric | Abdominal pain | 11 days | Surgery; prednisone and cyclophosphamide | Recovery |
| Unlu et al. [18] | 43/male | Aorta | Abdominal pain | 9 years | Aorto-iliac Dacron inlay graft; steroids and mycophenolate acid | Recovery |
Large and middle size vessels aneurysms in GPA: review of literature
Prior to the year 2000, the cases were described as a vasculitis overlap syndrome [3] because the presence of multiple visceral aneurysms was pathognomonic of middle vessel vasculitis such as PAN [1].
It was only later—with the emergence of more cases—that aneurysm formation of middle and large vessels was directly associated to GPA itself. The most plausible pathophysiology is necrotizing vasculitis of vasa vasorum [5,6] that can lead to necrosis of the arterial media with extension of the process into the intima and adventitia. An aneurysm may ensue with loss of the elastic lamina in focal areas of segmental necrosis [1].
The main concern is rupture of the aneurysm that can be life-threatening, as reported in four cases [3,4,6,7] (all abdominal aneurysms with subsequent fatal hemorrhagic shock). Treatment consisted mainly of immunosuppressive therapy (steroids and cyclophosphamide) along with surgical repair or embolization when feasible.
Interestingly, in our case, we noticed the concomitant increase in c-ANCA titer with the finding of the aneurysm, without any other sign of relapse. With prednisone reintroduction, the c-ANCA titer became undetectable. Therefore, we can presume that our patient had a GPA relapse while on maintenance therapy manifesting solely as a hepatic artery aneurysm with increasing c-ANCA titer.
This should prompt nephrologists to think of middle or large vessel aneurysms as a possible complication of GPA in the context of bleeding, anemia, abdominal pain, or any vessel involvement. The most sensitive tool would be angiography; however, it is not always recommended in case of renal dysfunction. The presence of intrarenal aneurysms (present in seven cases out of 19) [1,2,8,10,12,15] should be considered as well when a kidney biopsy is requested for the diagnosis of GPA. Treatment of aneurysmal vasculitis should combine embolization when feasible, with high-dose prednisone and other immunosuppressive agents to prevent life-threatening rupture.
4. CONCLUSION
This is the fourth case of hepatic artery aneurysm associated with GPA among several other cases of middle and large artery involvement. This raises the question of whether it is worth screening for large vessel aneurysms in any patient diagnosed with small vessel vasculitis. This will help establish the frequency of such findings in cases of small vessel vasculitides and further assess the need for review of the overall classification.
CONFLICTS OF INTEREST
All authors certify that they have no personal financial or institutional interest in the subject matter, materials, or drugs in this report.
AUTHORS’ CONTRIBUTION
All four authors were involved in diagnosing and managing the reported case. SSB and BAK narrated the case and reviewed the literature. CJM selected and described the images. SYT reviewed and corrected the article.
ACKNOWLEDGMENT
We thank Nadeen J. Khoury, MD, for critically reviewing the manuscript.
REFERENCES
Cite this article
TY - JOUR AU - Sora S. Boustany AU - Sammy Y. Tawk AU - Charbel J. Mourad AU - Beatrice A. Karam PY - 2021 DA - 2021/11/16 TI - Hepatic Artery Aneurysm in Granulomatosis with Polyangiitis JO - Dr. Sulaiman Al Habib Medical Journal SP - 140 EP - 143 VL - 3 IS - 4 SN - 2590-3349 UR - https://doi.org/10.2991/dsahmj.k.211108.001 DO - 10.2991/dsahmj.k.211108.001 ID - Boustany2021 ER -