
Where Should Mobile Health Application Providers Focus Their Goals?
 , Kuo Du1, Keyu Zhu1, *, , Shen Xu1, Shanshan Zhang2, 3
, Kuo Du1, Keyu Zhu1, *, , Shen Xu1, Shanshan Zhang2, 3- DOI
- 10.2991/ijcis.d.210305.001How to use a DOI?
- Keywords
- Service evaluation; Mobile health application; Domain-adaptive; Machine learning; Delphi
- Abstract
In the context of “Internet +” medical treatment, mobile health applications provide services for people in a new way, making it possible for people to carry out health management anytime and anywhere. According to the survey data, the most powerful consumers in the field of mobile health applications are those aged 24 to 35. Thus, it is particularly important to study the preferences of young people for mobile health applications. Therefore, this study established a domain-adaptive mobile health application evaluation model based on users' experience, and used an interactive algorithm combining machine learning and Delphi method to calculate the weight distribution of evaluation factors. Compared with previous studies, the evaluation index based on user experience of youth group is established. On the one hand, we have a targeted understanding of the use characteristics of the youth group and subdivide the market of mobile health applications; on the other hand, we establish evaluation indexes based on user experience, which is more in line with the customer-oriented product service concept. At the same time, the mobile health application evaluation system established in this study adopts human-computer interaction, which can not only ensure efficiency, but also add expertise in the field to make the results more accurate.
- Copyright
- © 2021 The Authors. Published by Atlantis Press B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
This study was conducted by a health management company that recently plans to develop a mobile health app specifically for young people. Mobile health applications are apps that are installed on small mobile devices such as tablets or smartphones. It can interact with users through contact-based interface to realize health management anytime and anywhere, which makes it an important part of modern medicine [1]. In order to take advantage of the development of the Internet and obtain lasting competitiveness, it is necessary to develop mobile health application. For the sake of confidentiality, we use the fictitious name mobile health management (MHM) instead of the company.
MHM is a company in the growth stage, mainly providing nutrition and health consulting, health maintenance services and consulting, weight loss services, etc. It takes “Identify problems earlier; Solve problems more effectively; Change health management more innovative” as service tenet and is committed to providing a high-level health management service to meet customers' needs. Although the MHM was founded only 5 years ago, it has achieved good development.
According to their 5-year experience in service, senior managers perceive that the youth market is a “fat sheep,” and that this generation of young people is significantly different from previous generations in the standard of appraising mobile health applications. Accordingly, they decide to use Target Focus Strategy, which means focusing on the youth market to provide mobile health services in line with the characteristics of contemporary youth and striving to gain competitive advantage in the local market.
In order to achieve this goal, it is particularly important to understand the factors that affect the level of evaluation of mobile health application by young people. It is also of great importance to know the necessity of each influencing factor. Therefore, based on users' experience, we evaluate acceptance of mobile health application by young people from cognitive and emotional perspectives. After reading the literature and making appropriate adjustments according to the requirements of this study, we determined the evaluation indexes [2]. In this study, 870 young people were selected for questionnaire survey, including 452 men and 418 women from 8 different provinces including Beijing, Hebei, and Anhui, etc. Among them, there were undergraduates, postgraduates, teachers, civil servants, and enterprise employees. Different questions are set for each evaluation factor and the acceptance of mobile health applications.
The acceptance degree implies the information about the distribution of evaluation factor weight, because users rate mobile health apps based on their experience. Since machine learning algorithm can automatically learn the implicit weight distribution information in sample data set to calculate the weight of evaluation factors, we use it to calculate the weight of indicators. However, an unavoidable problem with the data obtained from the survey method is that it relies too much on the subjectivity of the respondents, so the survey error will be relatively large. Considering that in the domain-adaptive evaluation algorithm, the final index weight is calculated by multiplying the index weights at all levels, we use the prior knowledge of experts to assign weights to the first- and second-level indexes, so as to reduce the influence of subjectivity of questionnaire data and make the weight calculation more accurate.
Our contributions of this paper are mainly reflected in two aspects. On the one hand, in terms of evaluation indexes, the current evaluation models of mobile health application use evaluation factors unrelated to service fields, which cannot comprehensively measure users' requirements for the quality of mobile health application (APP) service. In this study, evaluation indexes are set from the perspective of users' experience, which can better reflect users' recognition degree of mobile health application. On the other hand, in terms of evaluation methods, an interactive algorithm combining machine learning and Delphi method is adopted to calculate the weight distribution of evaluation factors. This algorithm is proved not only to speed up the calculation process of weights, but also to improve the accuracy of weight distribution. Meanwhile, the evaluation framework of this study supports adding the feedback of the results into the new sample set, in order to realize the dynamic adjustment of weight distribution, and adjust the evaluation index with the knowledge of domain experts to realize the dynamic evaluation.
The paper is organized as follows. In Section 2, we review the literature. In Section 3, we describe the implementation framework of the model. In Section 4, we introduce data collection and evaluation indicators system. In Section 5, we introduce method of evaluation. In section 6, we show the results and our analysis of them. Finally comes our conclusion.
2. LITERRATURE REVIEW
2.1. The Use of Mobile Health Apps
Mobile health apps can support continuous health monitoring at the individual and population level, encourage health behaviors to prevent or reduce health problems, support self-health management, increase knowledge, and reduce healthcare visits [3,4]. It has been proved to be beneficial to people's health in many aspects, in psychology, disease management, and healthcare [5,6].
In psychology, mental health apps have potentials in improving the monitoring and management of mental health symptoms or disorders [7]. For example, studies show that low-intensity mindfulness intervention through the use of mobile health apps can effectively improve the psychological distress (depression, anxiety, stress) and sleep dysfunction (subjective sleep quality, sleep latency, habitual sleep efficiency) of Chinese college students [8].
In disease management, mobile health apps can improve education and self-care for patients with complex conditions [9]. It has achieved good results in improving the metabolic index of diseases and strengthening self-management and shown overall positive results in improving physical deficiencies in hypertension, weight, tobacco smoke, diabetes, dyslipidemia, etc [10]. For example, brown demonstrated the feasibility and usability of an interactive, immersive 3d iPad health game for cancer patient disease management through experiments [11]. Baker developed a new medical non-contact control system, which greatly helped patients with physical disabilities. To realize the function of calling nurses and the effect of controlling hospital equipment [12].
In healthcare, satisfactory treatment compliance and subsequent health maintenance can be achieved with a high level of exposure to mobile health applications [13]. Some apps may have positive benefits when used to deliver exercise or gait training interventions, as self-management systems, or as measurement tools [14]. They are also effective adjuncts to the improvement and maintenance of weight loss after bariatric surgery [15].
Mobile health apps play an important role in improving or maintaining people's physical health, but the quality of mobile health apps on the market today varies greatly. Therefore, it is necessary to evaluate them and design applications that are more acceptable to users, thus bringing greater convenience to people.
2.2. Evaluation Index of Mobile Health Application
At present, many researches have been carried out in the field of mobile health application evaluation, and scholars have proposed different evaluation indexes.
We can use perceived usefulness to measure attitude, perceived ease of use to measure satisfaction, and behavioral intention to measure interest and importance to evaluate mobile health applications [16]. Awareness of devices and health information plays an important role in influencing how users rate mobile health applications [17]. Flexibility; performance; competency; learnability; completeness; information; other outcomes; error prevention; flexibility can be used to evaluate the usability of mobile health applications [18]. It has been proved that the quality of information and the credibility of sources played a great role in the evaluation of mobile health applications [19]. Privacy also plays an important role, patients want hospitals to assist them with high efficiency without revealing patients' identities [20].
We can evaluate applications by using the following criteria: cost (free or paid); content (medical information, symptom log, etc.); relevant public or private healthcare; target audiences healthcare and non-healthcare professionals; validity (citing medical information that has been peer-reviewed or otherwise verified); and average user ratings (from 1 to 5 stars) [9]. Georgsson puts forward a multilevel evaluation model: level 1 is the target system specification, which is used to understand user tasks for system development. Level 2 is a test of task performance to evaluate system validation and human-computer interaction in a laboratory environment. Level 3 aims to combine environmental factors to determine the impact of the system in the real environment [21]. According to the above research results, evaluation indexes are mostly specified from the application itself. Although they are important for evaluating mobile health applications, they mostly use indicators unrelated to the mobile health application service field. Therefore, we add indicators starting from users' experience, which can better reflect the “user-centered” concept.
2.3. Evaluation Method of Mobile Health Application
In the evaluation method of mobile health application, it can be roughly divided into two categories. One is to conduct relatively simple statistical analysis of the data by designing questionnaires, the other is to build a model and then analyze the data.
Brown uses Dedoose qualitative data analysis (QDA) software, a web-based qualitative and hybrid data analysis program, to analyze collected data and visualize the results to evaluate mobile health applications [18]. Battle uses a comprehensive analysis, which combine qualitative and quantitative methods to evaluate mobile health applications. In the qualitative part, data are collected by means of targeted sampling and Emi-structured interview, then they do thematic analysis. In the quantitative part, data are collected, calculated with SAS 9.2, and then analyzed and compared [22]. Liu estimated the influence of each quality dimension on continuous use intention, by statistical analysis of the survey responses of 191 users [23].
Meng combined health awareness with refined likelihood model to test people's daily willingness to use mobile health applications [19]. Mattias puts forward a method to enhance cognitive roaming (the Cognitive walkthrough (CW)), which means take the user as the center of the CW (UC—the CW) when solve defects that have been found in the original technology, and verify by thinking about the statement agreement. In order to assess the effectiveness, efficiency, and self-management of mobile health applications among users with diabetes [21]. Mattias tested the usability of mobile health applications by using the framework analysis (FA) approach and usability issues taxonomy (UPT). It is also shown that using this method can help identify usability problems, especially initial usability problems [24]. Paulo used a mixed method of partial least squares and fuzzy set qualitative comparative analysis to evaluate the number of causal condition combinations that promote mHealth adoption [25].
After the above summary, we can find that the current evaluation methods are mainly simple statistical analysis, or the establishment of simple qualitative and quantitative methods to analyze the obtained data, which are traditional and do not reflect intelligence, and do not consider the authenticity of the data.
Therefore, this paper proposes a mobile health application evaluation model based on user experience, which uses ontology language to describe the relationship between concepts in the evaluation model, makes different evaluation factors through domain experts, and calculates the weight distribution of evaluation factors, according to the knowledge collected by the user system, by machine learning algorithm meanwhile it supports optimize the weight by the prior knowledge of the domain experts through Delphi method.
3. FRAMEWORK OF MOBILE HEALTH APPLICATION EVALUATION
In order to build the evaluation model of mobile health application, we design a system as the prototype system of the evaluation model mentioned above. We call it mobile health application evaluation system (MHAES), which can dynamically adjust the evaluation model according to specific conditions.
As shown in Figure 1, MHAES is mainly composed of three parts. They are the data part, the expert part, and the user part. The first part is the data part, including ontology query/storage engine and relational database, which are used to query and store ontology data. The second part is the expert part, including evaluation model manager, evaluation category constructor, evaluation factor constructor and weight algorithm engine, which is used to construct evaluation model, evaluation category and evaluation factor, and calculate the weight distribution of evaluation category and evaluation factor. The third part is the user part, including data receiver, result publisher, data preprocessor and evaluation engine for evaluating mobile health applications.
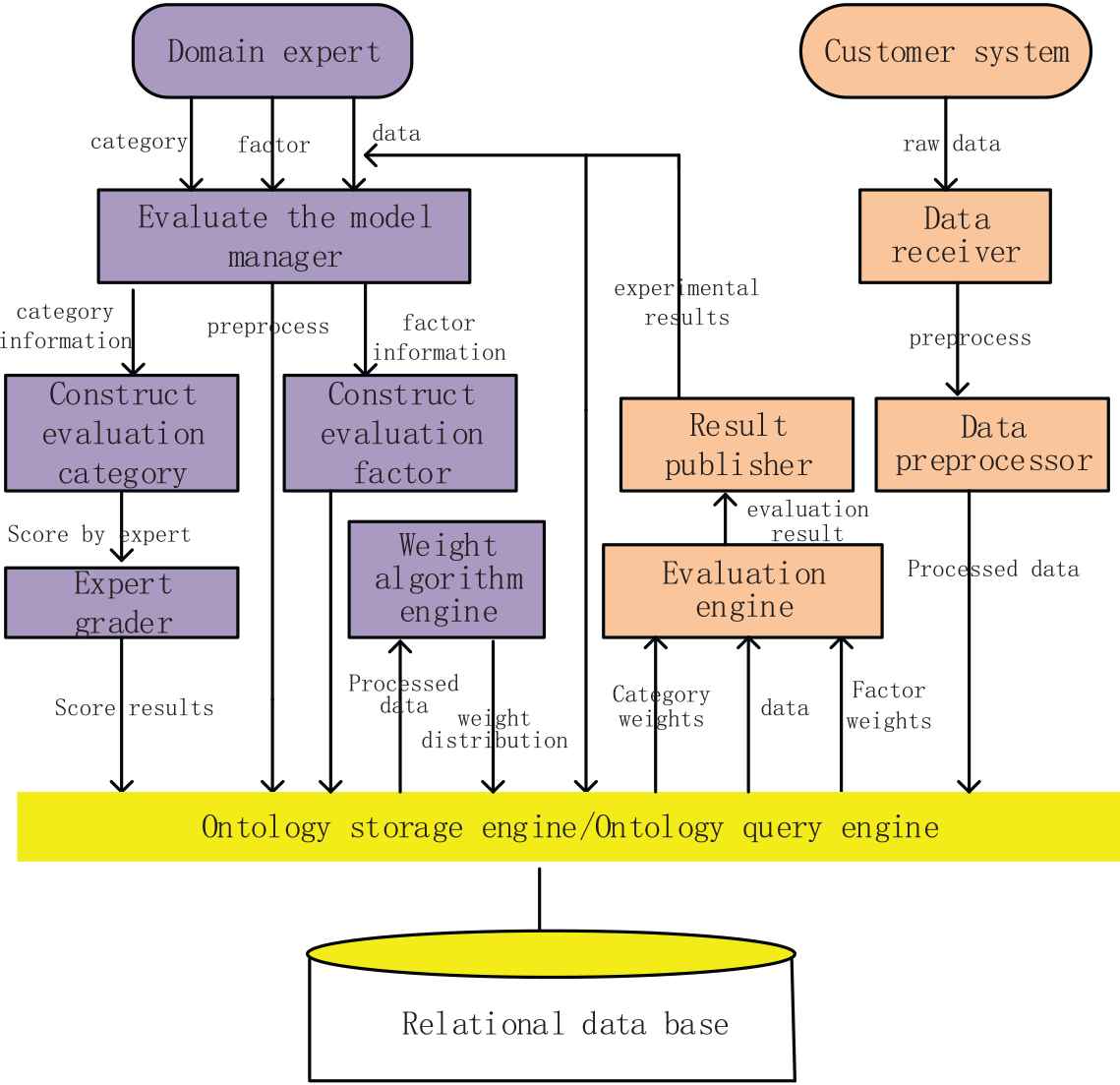
Mobile health application evaluation system (MHAES).
The expert part of MHAES realizes the construction of the evaluation model, which mainly uses the prior knowledge and sample data acquired by experts to construct the evaluation model. The construction process can be divided into the following steps: (a) The domain experts create the evaluation factor in the evaluation model manager. Construct new evaluation factor through the valence factor constructor according to the information contained in the evaluation results output by the user part. Then save them in the data part by the ontology query engine. (b) Experts score the evaluation categories to obtain the scoring results. Preprocessed the experts' scoring data and sample data and store them in data part by ontology query engine. (c) The weight algorithm engine obtains expert scoring data and sample data from the ontology query engine to calculate the weight of each evaluation category and evaluation factor, and store the calculated results in the ontology storage engine.
The user part of MHAES implement the function of evaluating mobile health applications. Specifically, the original data used for evaluation is obtained from the user system, and the evaluation engine is used to calculate the quality of mobile health application service, and the evaluation results are given. The data receiver obtains the data provided by the evaluation user system, the data preprocessor completes the preprocessing of the original data, and the evaluation engine obtain the evaluation factors and the pre-processed evaluation data from the ontology storage engine. After all these preparatory activities are completed, the evaluation engine uses the obtained information to evaluate, then store the results in the database. At the same time, the result publishing module can receive the results and publish them to decision makers, this information can help them improve the functions of the APP. Meanwhile, it can feed back to experts, so that they can dynamically adjust the evaluation model according to the changes of user experience, in order to make the evaluation standard more reasonable.
4. DATA COLLECTION AND EVALUATION INDICATORS SYSTEM
4.1. Data Collection
870 young people were selected in this study for questionnaire survey, which includes 452 men and 418 women from 8 different provinces. Among them, there were undergraduates, postgraduates, teachers, civil servants and enterprise employees. At the same time, it is necessary to introduce the evaluation experts in Delphi method. It is composed of 20 experts with rich experience in mobile health application, including experts from Hefei university of technology (5 people), Hebei university (3 people), Beijing University of Technology (5 people), and employees from mobile health apps company (7 people). Some of the data used to support the findings of this study are included within the article.
4.2. Evaluation Indicators System
In order to facilitate readers to better understand the content of expert-level evaluation model in mobile health application evaluation model, this part will explain the definitions of the terms involved in the model and the relationship between them.
Evaluation Factor: Evaluation factor is a basic evaluation unit extracted from users' experience (including cognition and emotion), which is composed of a binary group:
In this paper, reliability is an important aspect to describe users' experience and influence users' evaluation of APP, which can be defined as the evaluation factor of mobile health application. Domain experts can customize various types of evaluation factors in this model. To facilitate the use of prior knowledge to calculate the weight of evaluation factors, we give the concept of evaluation categories.
Evaluation Category: Evaluation category represents a conceptual clustering of evaluation factors, which is composed of triples:
In this paper, cognition-based information quality evaluation can be used as an evaluation category
Evaluation Concept Tree: Evaluation concept tree T is a tree structure composed of evaluation factors and evaluation categories as nodes. Evaluation categories are internal nodes of evaluation concept trees and evaluation factors are leaf nodes of evaluation concept trees. The hierarchy of evaluation concept tree is composed as follows: Each element in the set item of evaluation category s is the child node of evaluation category s; all nodes have a unique parent except for the evaluation category at the root node. Meanwhile, the weights of nodes in the evaluation concept tree have the following constraints:
The weight of root node is 1.
The weight of any evaluation class node s is the sum of all the weight of its children.
In this paper, Figure 2 shows the evaluation concept tree of this study. The root node of the evaluation concept tree has two sub-evaluation categories (based on cognition and based on emotion), which contain different sub-evaluation categories. These two indicators were chosen because of what Christina Chick CF found in his research that clinical research across the developmental spectrum increasingly reveals the nuanced ways in which emotion and cognition can work to either support or derail rational (i.e., healthy or goal-consistent) decision making [26]. Weights start at the root node and are distributed layer by layer to the lower nodes and end at the leaf node. Different weight distribution of evaluation factors reflects different evaluation standards of users. Since different types of mobile health applications have different evaluation concept trees, it is necessary for domain experts to customize evaluation concept trees for mobile health applications in this field.
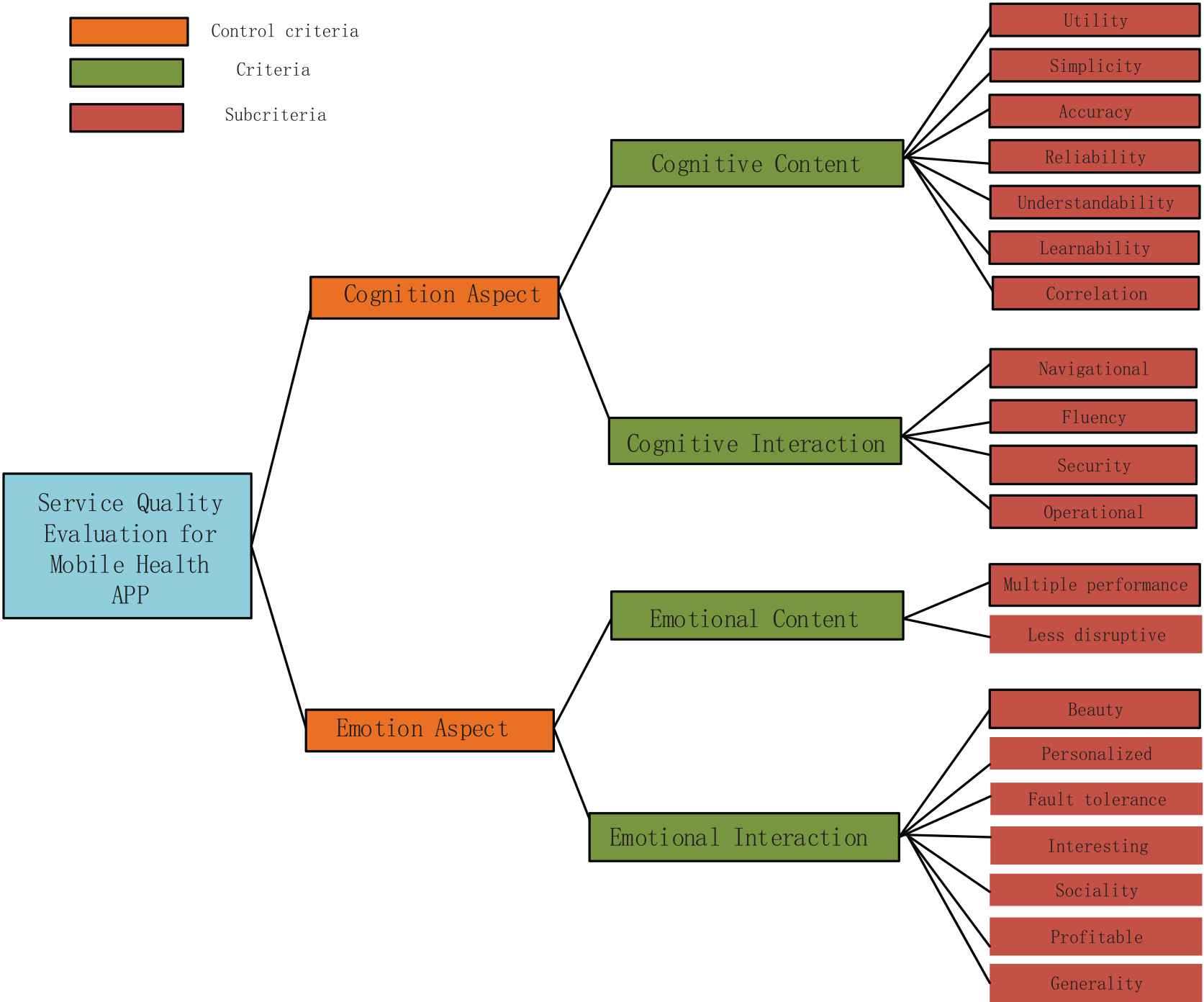
Evaluation concept tree.
4.3. Semantic Description Diagram of Evaluation Indicators System
Mobile health application evaluation model is composed of quintuples
Figure 3 shows the semantic description graph of the evaluation model of mobile health application in this study. Evaluation concept tree represents the tree of evaluation T, category represents the category of evaluation, factor represents the factor of evaluation, and predicate {has Root, consist of} jointly defines hierarchical relation of evaluation concept tree. Survey instance represents the instance of survey SI, data instance represents the instance of data DI, evaluation result represents the result of evaluation ER), predicate {from Tree, has Factor} represents the relationship between Data instance DI and evaluation concept tree T, while predicate from service represents data instance DI from service instance SI and evaluation result ER is evaluation result of service instance SI. O stands for name field and R for cardinality. A cardinality of 1 is numeric, and a cardinality of −1 is non-numeric.
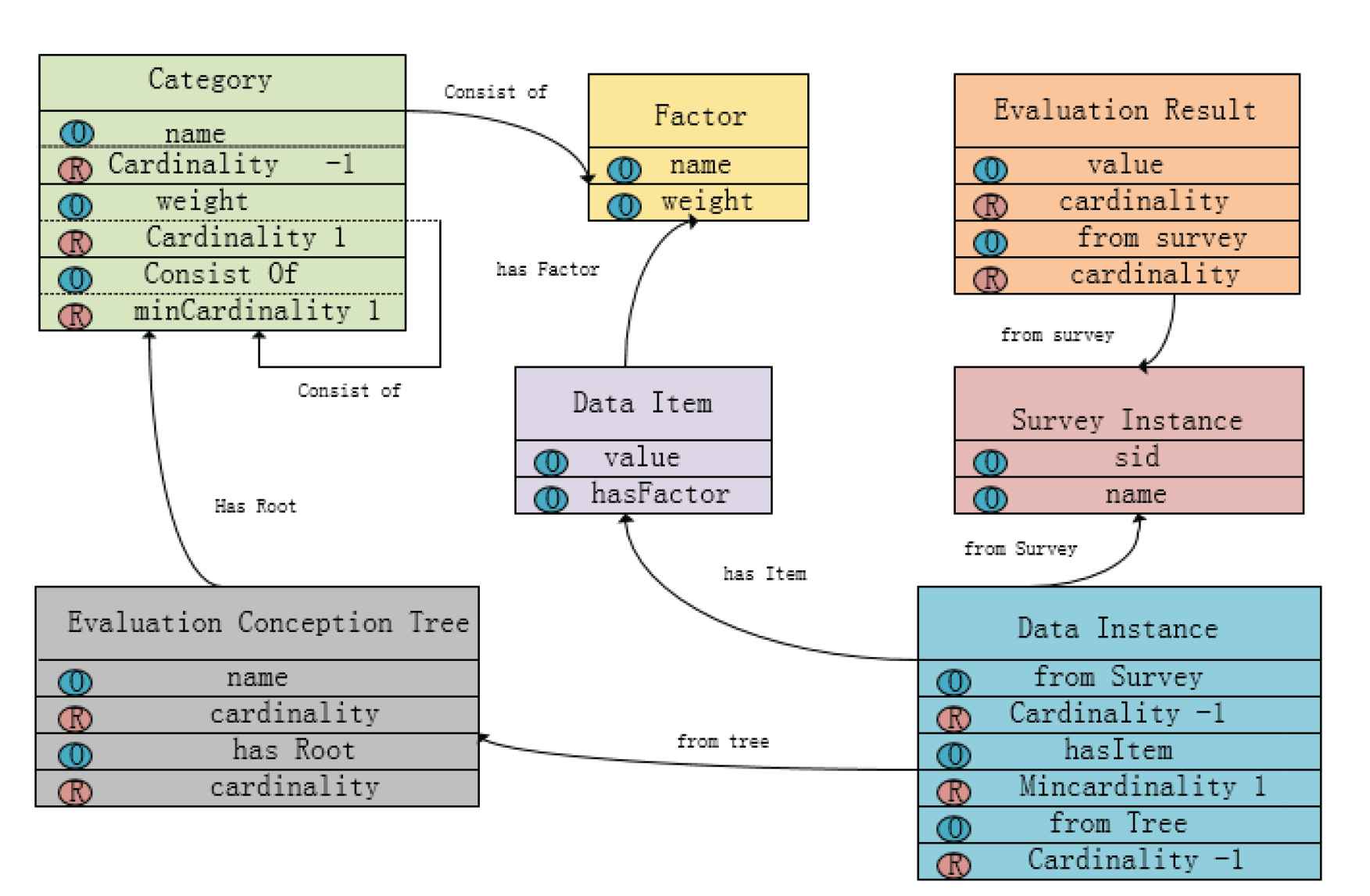
Semantic description diagram of mobile health application evaluation model.
According to the above description of the evaluation model and its components. We assume that the evaluation concept tree T has
Calculation formula of evaluation:
It can be seen from Equation (1) that the evaluation results of mobile health applications are determined by the value of evaluation factors and the weight distribution of evaluation factors. The value of the evaluation factor is derived from user experience, and the weight distribution of the evaluation factor can be calculated according to the user's feelings in the process of use and the prior knowledge of domain experts, which is obtained from the domain experts with the help of the evaluation concept tree. In the next section, we will calculate the weight distribution.
5. METHOD OF EVALUATION
Generally, evaluation factors will have different value ranges. Therefore, in order to ensure the comparability of the weights of evaluation factors, it is necessary to preprocess the evaluation data and adjust the range of all evaluation factors to a uniform interval. However, in this study, due to the scale used in the survey, the number of each evaluation factor is between 1 and 5, so the weight can be calculated directly without standardization.
In the weight calculation, to make the weight distribution of evaluation factors close to the evaluation standard of users, we not only used the machine learning algorithm to calculate the weight of each evaluation factor, but also introduced the prior knowledge of experts by Delphi method to optimize the weight distribution.
5.1. Machine Learning Algorithm
The machine learning algorithm can automatically learn the implicit weight distribution information in sample the data set to calculate the weight of the evaluation factors.
In this study, 870 young people were selected for the questionnaire survey, and the options were set for each evaluation factor and the acceptance level of the mobile health application. Because users rate mobile health apps based on their experience, the acceptance degree implies the information about the weight distribution of the evaluation factor. We represent a group of sample data as a binary group:
Set
Equation (4) can be used to calculate the information gain of each evaluation factor, and Equation (5) calculates the weight of each evaluation factor based on Equation (4):
By calculating the information gain of the evaluation factors, we can learn the weight distribution of each evaluation factor from the sample set. After sorting out the data of 870 questionnaires, we divide the data set into two categories according to the attitude of the respondents toward the mobile health application: attitude ratings of 4 and 5 are placed in one category, and those from 1 to 3 are placed in another category. According to the machine learning algorithm, the weights of third-level indexes are calculated, and the results are shown in Figure 4. To make the picture look simpler. CC is short for cognitive content, CI is short for cognitive interaction, EC is short for emotional content, EI is short for emotional interaction.
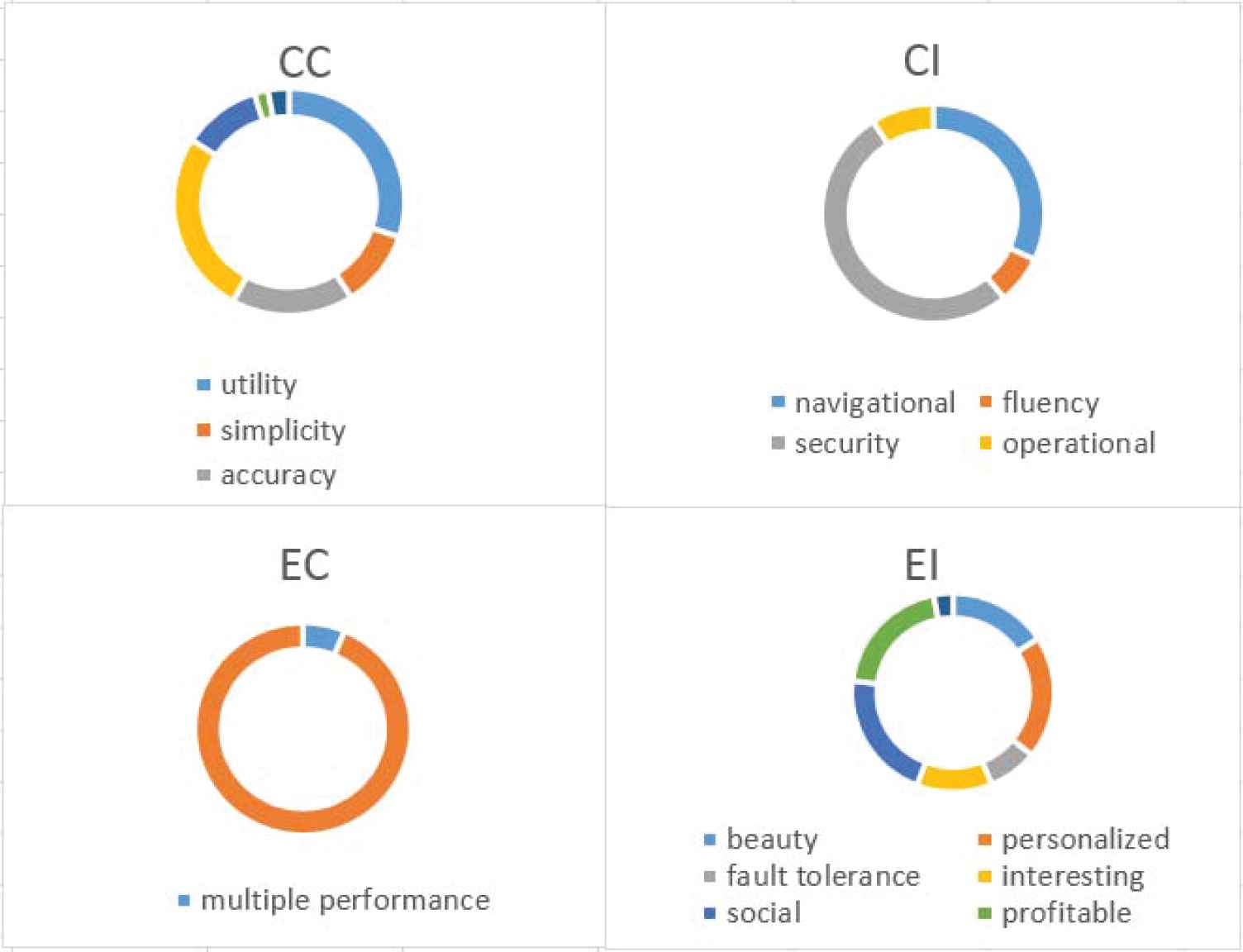
Weight distribution of secondary indicators.
5.2. Delphi Method
Because the information used to construct the sample set is gained by using the knowledge generated from the data collected from the survey, the evaluation result depends heavily on the size of the sample set and the quality of the sample. Therefore, the evaluation effect obtained is somewhat accidental. In fact, the domain experience of domain experts also implies the information of the weight distribution of the evaluation factors; as a result, adding the domain expert's prior knowledge to the calculation not only accelerates the calculation of the weight but also improves the accuracy of the weight distribution. The prior knowledge referred to in this study is the empirical knowledge of domain experts of the importance of different evaluation categories, which can be used to calculate the weight distribution of the evaluation factors. Therefore, we adopt the Delphi method to introduce the knowledge of experts.
We score the indicators by sending emails to experts and then process the scoring results by using a statistical approach. In the expert questionnaire, the importance degree is assigned based on the five subscales method. Because the familiarity of the experts with the five-subscale index varies and because the bases for their judgments are inconsistent, we need to use the degree of familiarity and the basis of judgment to distinguish the authority of experts; namely, the authority coefficient is equal to the average degree of familiarity and determines the arithmetic coefficient. The authority coefficient of experts is generally required to be larger than 0.7, and the degree of expert authority in this study meets this requirement. See Table 1.
| Degree of Familiarity (Cs) | Criterion (Ca) | Authority Coefficient (Cr) | |
|---|---|---|---|
| First round of inquiry | 0.88 | 0.865 | 0.8725 |
Authority of expert.
In this study, experts were consulted mainly on the weight of the first- and second-level index. Because of the small number of indicators and the low decision-making complexity, 20 experts are enough. The specific steps were as follows: the questionnaire was developed based on the literature research and evaluation indexes determined by experts in previous fields. After the Delphi questionnaire was collected, the questionnaire was analyzed. The Kendall coordination coefficient of the first-level index in the first round of the letter consultation was 0.716
| Control Criteria | Weight | Criteria | Weight |
|---|---|---|---|
| C | 0.52 | CC | 0.31 |
| CI | 0.21 | ||
| E | 0.48 | EC | 0.19 |
| EI | 0.29 |
The weight of primary and secondary indicators.
5.3. Interactive Algorithm Combining Machine Learning and the Delphi Method
To effectively use prior knowledge, we define the local weight of the nodes in the evaluation concept tree. The local weight
Definition 1.
If the node
In Definition 1, if the node
Definition 2.
The weight of node N is equal to the product of the nearest local weight of each node in the path from node N to the root node.
Set the node sequence on the path from any evaluation factor to root of the root node of the evaluation concept as
From Definition 2, it can be concluded that the weight of the evaluation factor is
By substituting Equation (6) for Equation (7), a new formula for calculating the weight of the evaluation factors can be obtained:
Equation (8) gives a new method to calculate the weight of the evaluation factor: If the nearest local weight of the first k ancestor nodes of the evaluation factor and a local weight of the evaluation factor are calculated, the weight value of the evaluation factor can be obtained. The nearest local weight of the k ancestor nodes before the evaluation factor can be calculated by the prior knowledge of domain experts, while the local weight of the subtree with the ancestor node of the k layer as the root node can be calculated by machine learning algorithm.
A detailed description of this method is given below. In this model, by referring to the Delphi method, we determine the weights of the first- and second-level indexes by consulting 15 experts by letter. Importance was rated on a five-level scale: 1 means “very unimportant”; 2 means “not important”; 3 means “important”; 4 means “more important”; and 5 means “very important.” Under the condition that the degree of coordination of opinions of all items meets the requirement (Kendall coordination coefficient >0.7), the average value assigned by each expert for each indicator is calculated as the basis for determining the weight. The average score of each indicator is divided by the average score of all indicators at the same level as the weight. Set the child nodes of node N as
Algorithm implementation:
Step 1: Initialization, node variable v = root, current level counting variable c = 0, add to H;
Step 2: If ((c < k) inverted v (v is not an evaluation factor))
Domain experts set the importance level for each child node of v, and calculate the nearest local weight of each child node by Equations (9) and (10). Traverse each child node of V;
Repeat step 2;
Else {under the subtree T with v as the root node, machine learning algorithm is adopted to calculate the local weight of each evaluation factor on T'}
6. ANALYSIS AND DISCUSSION
6.1. Experimental Results
According to the analysis, the weight distribution of indicators at all levels is obtained, as shown in the table below. See Table 3
| Control Criteria | Weight | Criteria | Weight | Subcriteria | Weight |
|---|---|---|---|---|---|
| Based on cognition | 0.52 | Cognitive content | 0.31 | Utility | 0.093 |
| Simplicity | 0.034 | ||||
| Accuracy | 0.053 | ||||
| Reliability | 0.081 | ||||
| Understandability | 0.034 | ||||
| Learnability | 0.006 | ||||
| Correlation | 0.009 | ||||
| Cognitive interaction | 0.21 | Navigational | 0.067 | ||
| Fluency | 0.015 | ||||
| Security | 0.109 | ||||
| Operational | 0.019 | ||||
| Based on emotion | 0.48 | Emotional content | 0.19 | Multiple performance | 0.012 |
| Less disruptive | 0.178 | ||||
| Emotional interaction | 0.29 | Beauty | 0.046 | ||
| Personalized | 0.058 | ||||
| Fault tolerance | 0.023 | ||||
| Interesting | 0.035 | ||||
| Sociality | 0.061 | ||||
| Profitable | 0.058 | ||||
| Generality | 0.009 |
Weight distribution of each indicator.
To show the results of the weights more clearly and compare the weights of each index more intuitively, the results are expressed in the form of a rectangular tree graph. See Figure 5 for details.
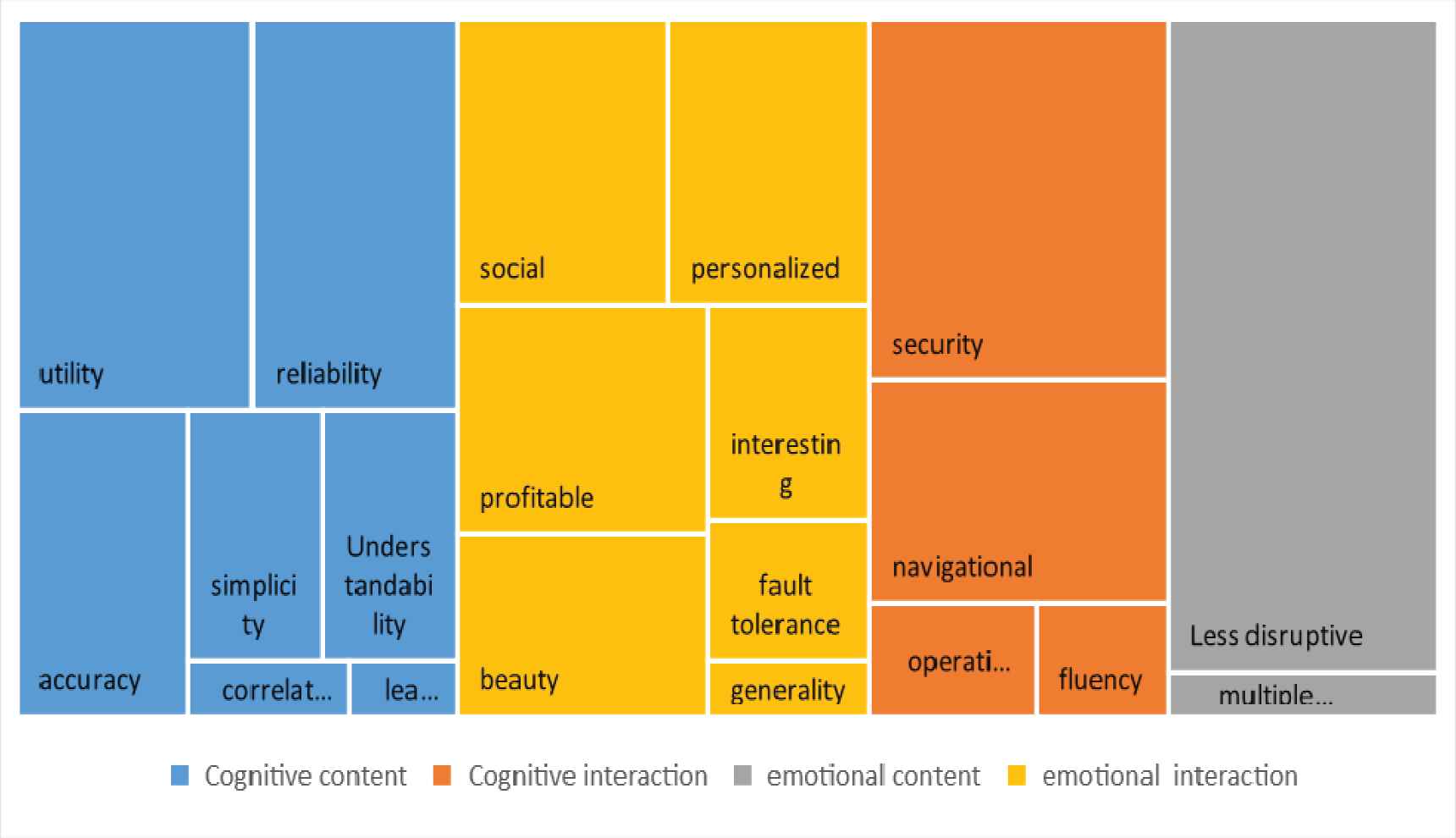
The weight distribution represented by the rectangular tree graph.
6.2. Results Analysis
Different weights represent different degrees of importance. Next, we will analyze the results from the perspective of three levels of indicator results. The first section of the analysis identifies the importance of two primary indicators. Both cognitive and emotional information are important in influencing users' evaluation of mobile health apps. The cognitive level of information (which was 0.52) was only four percentage points higher than the emotional level (which was 0.48).
The mobile health application designed for the youth group shows that we should consider not only users' cognitive needs but also their emotional needs. Therefore, on the one hand, we need to be able to cognitively provide users with information that is as they would expect it to be: accurate, reliable, easy to understand, concise, and effective in problem solving. On the other hand, we need to provide users with information that is expressed, as they would expect, in various forms according to different needs. This is a chance to design an app according to users' preferences and that provides information that indeed provides real benefits to users.
In the second part of the analysis, the importance of four secondary indicators is determined. The effects of content information on cognition, interaction information on emotion, interaction information on cognition, and content information on emotion are, in order of importance, 0.31, 0.29, 0.21, and 0.19, respectively. At the cognitive level, content information is more important than interactive information. At the emotional level, interactive information is more important than content information. Therefore, when designing mobile health applications, different indicators should be emphasized at different levels.
In the third portion of the analysis, to better understand the results, we consider it necessary to explain each indicator in detail (see in Appendix A). The importance of 20 three-level indicators is determined. These indicators, in descending order of importance, are as follows: less disruptive (0.178), security (0.109), utility (0.093), reliability (0.081), navigational (0.067), sociality (0.061), personalized (0.058), profitable (0.058), accuracy (0.053), beauty (0.046), interesting (0.035), simplicity (0.034), understandability (0.034), fault tolerance (0.023), operational (0.019), fluency (0.015), multiple performance (0.012), correlation (0.009), generality (0.009), and learnability (0.006). The weight distribution is relatively concentrated, with the weight ratio of the first 10 indicators exceeding 0.8 and that of the first 5 indicators exceeding 0.5. Therefore, when designing mobile health applications, it is necessary to pay special attention to the key indicators.
Somewhat surprisingly, user's value having fewer distractions the most. However, because young people are very averse to being interrupted by useless information, it is reasonable that having fewer distractions is such a high priority for them. Therefore, efforts should be made to ensure that there is no distracting information (advertisements, ambiguous information, etc.) in the content provided. If such information must be added because of commercial interests, we should consider the form of the advertising and try our best to add only a small amount of soft advertising.
The second most important indicator is security. Therefore, developers need to take effective measures to protect the privacy of users. Developers should reduce system vulnerabilities, improve security, and prevent the system from being breached by criminals.
The third most important indicator is utility, which provides information to solve problems faced by users and provides reliable suggestions to users. Utility is the most basic requirement for mobile health apps. If a mobile health app does not have utility, it does not matter how well the app performs in other respects. Therefore, enterprises need to integrate internal and external high-quality resources to improve service quality.
The fourth most important indicator is reliability: the source of content must be authoritative and reliable and must clearly label who is the diagnostician and whether that person has the relevant qualifications. Reliability is the basis for achieving utility. Only information provided from a reliable source can instill in users a sense of security and help them find the right professional in case of an accident.
The fifth most important indicator is navigability: the system should have a simple navigation bar or other convenient navigation mode to help users quickly find the information they need.
In this study, we also found that the weights assigned to the four secondary indicators—sociality, personalized, beauty and interesting—accounted for a significant proportion of the total weights assigned, thus exceeding our expectations. The significance of these four secondary indicators is also an important finding of this study and provides a new direction for the design of mobile health applications aimed at young people. Concerning sociality, special modules can be set up in the app to provide opportunities for users to communicate through the app and bridge the communication between users, patients, and other relevant persons. “Personalized” indicates that the service and interface of the system can be personalized and optimized according to users' preferences so that users can participate in the design of the interface and information architecture and have some control over the system. Personalization is the embodiment of young people's pursuit of individuality. “Beauty,” indicates that the system interface and information presentation mode are aesthetically rich. Meanwhile, it is also of great importance that color, font, and graphics are used in the proper proportions; beautiful formats are designed so that information can be presented through pictures, cartoons, and other interesting forms. “Interesting” indicates that the design and operation mode of the system is interesting and that the makers of the app avoided creating a rigid design and an outdated interaction mode. Makers of interesting apps appropriately adjust and update the system promptly and follow development trends. Meanwhile, the research results also show that the importance of universality and learnability is very low, thus indicating that the first generation of young people to grow up with the Internet has no difficulty using mobile health apps. Young people do well in using different apps, so they pay less attention to versatility and learnability.
7. CONCLUSION
This paper adopts a comprehensive evaluation method to help a mobile health application company to determine the indicators that should be focused on in the development of mobile health applications targeted at youth. The research methods and ideas in this paper are of great significance and inspiration for other enterprises to make similar decisions. Most of the current studies focus on the analysis of the therapeutic effects of mobile health applications for one or several diseases, and most of them are targeted at patients. One part of the study was a group experiment in different populations to demonstrate the effectiveness of mHealth applications for one or several diseases. Such as Brian C, Anjani K. Singh, etc., demonstrated the effect of mobile health applications on asthma by following 39 patients and assessing their impact on asthma-related emergency room visits, hospitalizations, and oral prednisone [27]. XiaodanZhu, MinLi demonstrated mobile health applications can improve compliance with antipsychotic medications in patients with schizophrenia, by grouping 84 discharged patients from the Mental Health Center in Yinchuan, Ningxia hui Autonomous Region, China [28]. There are also a few indicators from the perspective of user experience, but the evaluation is not comprehensive enough. Such as LamyaeSardi, AliIdri, etc., use privacy, security, usability, and internationalization as indicators to evaluate the effectiveness of mobile health applications for postpartum healthcare [29]. DianaJ. LuMD, MinaGirgisBSb, etc., use engagement, functionality, aesthetics, and information to evaluate the effectiveness of mobile health applications in cancer patients [30]. MHM intends to provide focuses on providing health management services, and the target population is not only the sick population, but also the user experience, that is, more willing to use the application if those conditions are met. The evaluation index system based on user experience established in this study better reflects the service concept of “user-centered,” which is more suitable for MHM company's target positioning. Information is collected from both experts and users, and an interactive algorithm combining machine learning and the Delphi method is adopted to assign weights to the established indicators to correct errors in user data by using the prior knowledge of experts. We were surprised to find that the weights assigned to sociability, personalization, aesthetics, and interestingness accounted for a significant proportion of the total weights assigned; however, universality and learnability were poorly weighted. These results have important reference value for the development of mobile health applications.
Our study also has some limitations. First, in terms of indicators, we set only 20 indicators and asked respondents to score based on the existing indicators; however, the target valued by the user may not appear in the selected option. Second, in terms of data volume, we collected only 870 questionnaires, so the dataset is not large enough. If existing software data are used to analyze big data, the results will be more accurate. We expect people with access to big data to study these issues in the future and provide better advice for developers, so that they can create more user-friendly products.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
AUTHORS' CONTRIBUTIONS
XJW, KD and SSZ conceived of this study and participated in the design and administration of the study. WX and SSZ contributed to data acquisition. WQX and YXG analyzed the data and the results. XJW and KD drafted the manuscript. SSZ, WX and WQX supervised the work and revised the results critically. All authors read and approved the final version of the manuscript.
ACKNOWLEDGMENTS
This work was supported by a grant from the Key Disease of Diabetes Mellitus Study Center at the National Chinese Medicine Clinical Research Base, the China Scholarship Council, the National Natural Science Foundation of China Grant No. U2001201, 61876055, 71101041, and the National Statistics Research Projects Grant No. 2013LZ07 and National Steering Committee for Graduate Education of Chinese Medicine and Traditional Chinese Medicine Grant No. 20190723-FJ-B39.
APPENDIX
| Name | Meaning |
|---|---|
| Utility | Whether the content provided by APP can be defined as high-quality information depends first on whether it can solve the problems faced by users, that is, how useful the information is, and whether the information that can help users solve practical problems has utility. The better the problem is solved, the more effective the information will be. |
| Simplicity | The content provided by the APP is concise, without redundant information, and the amount of information is moderate. |
| Accuracy | The content provided by APP is expressed accurately and without ambiguity, grammar and logic errors. |
| Reliability | The source of the content is authoritative and reliable, including who the diagnostic personnel are, whether the relevant qualifications. |
| Understandability | Content is easy to understand, can be obtained when the content of information system provides information beyond the cognitive ability of the user, the user will think that this information is of little value, even is of no value, information quality is reduced, so convenient user cognitive information expression for information quality evaluation is very important, which requires the information content on the cognitive level of the target user optimization, ensure the information can be understand by user. |
| Learnability | Easy to operate and learn. |
| Correlation | Information that can meet the needs of users and meet the needs of users. |
| Navigation | The system has a simple navigation bar or other convenient navigation methods to help users quickly find the information they need. |
| Fluency | The system operates smoothly, responds quickly and has no lag. |
| Security | The system has few vulnerabilities, high security level, and is not easy to be breached by criminals. The information in the system is backed up, not easy to lose, not easy to be tampered with. The system is viral-free, which can effectively protect the privacy of users. |
| Operational | From the perspective of human-computer interaction, the system operation conforms to the cognitive law of people, which is natural for users. The system is easy to use, and the operation is simple and convenient, with few steps. |
| Multiple performance | The expression form of information also affects users' emotions. Different users tend to have different expression forms under different needs. When content information can be conveyed to users in a variety of expression forms according to users' needs, it will bring better emotional experience to users. |
| Less disruptive | There is no distracting information in the content, such as advertising information and ambiguous information |
| Beauty | System interface and information presentation is full of beauty, color, font, graphics and other reasonable collocation, beautiful layout design. |
| Personalized | The service and interface of the system can be personalized and optimized according to users' preferences, allowing users to participate in the design of the interface and information architecture, so that users have some control over the system. |
| Fault tolerance | The system should be tolerant of users' operational errors, allowing users to undo wrong operations, avoiding irreversible operations in the system, allowing users to explore boldly, without worrying about irreparable operational results. |
| Interesting | The design and operation of the system should be interesting and avoid rigid design and outdated interaction. |
| Sociality | Through APP communication, information can be obtained through conversations with patients and other relevant personnel. |
| Profitable | You get real benefits from using apps. |
| Generality | The interaction mode and operation method of APP should be consistent with the mainstream software, reducing the time for users to learn and use. |
Explanation of Each Indicator
REFERENCE
Cite this article
TY - JOUR AU - Xiaojia Wang AU - Kuo Du AU - Keyu Zhu AU - Shen Xu AU - Shanshan Zhang PY - 2021 DA - 2021/03/12 TI - Where Should Mobile Health Application Providers Focus Their Goals? JO - International Journal of Computational Intelligence Systems SP - 1119 EP - 1131 VL - 14 IS - 1 SN - 1875-6883 UR - https://doi.org/10.2991/ijcis.d.210305.001 DO - 10.2991/ijcis.d.210305.001 ID - Wang2021 ER -