
An Estimation of the Burden of Sports Injuries among African Adolescents
- DOI
- 10.2991/j.jegh.2017.10.010How to use a DOI?
- Keywords
- Sports; injury; adolescent; Africa
- Abstract
The extent to which sports injuries contribute to the burden of injury among adolescents in low- and middle-income countries (LMICs) is unknown. The goal of this study was to estimate the incidence of sports injuries among adolescents in Africa. Data from the World Health Organization Global School-Based Student Health surveys were used to estimate the annual number of African adolescents sustaining sports injuries. Gender-stratified injury rates were calculated and applied to every African country’s adolescent population to estimate country-specific and continent-wide injury totals. A total of 21,858 males and 24,691 females from 14 countries were included in the analysis. Country-specific annual sports injury rates ranged from 13.5% to 38.1% in males and 5.2% to 20.2% in females. Weighted average sports injury rates for males and females were 23.7% (95% CI 23.1%–24.2%) and 12.5% (95% CI 12.1%–12.9%), respectively. When these rates were extrapolated to the adolescent populations of the African continent, an estimated 15,477,798 (95% CI 15,085,955–15,804,333) males and 7,943,625 (95% CI 7,689,429–8,197,821) females sustained sports injuries. Our findings suggest that over 23 million African adolescents sustained sports injuries annually. Further work will help to more precisely define the burden of sports injuries in LMICs and the role that surgery can play in mitigating this burden.
- Copyright
- © 2018 Atlantis Press International B.V.
- Open Access
- This is an open access article under the CC BY-NC license (http://creativecommons.org/licences/by-nc/4.0/).
1. INTRODUCTION
Adolescent health is a pressing yet neglected issue in global health policy [1,2]. Investing in adolescent health can have long-term impacts on adult health, quality of life, and economic productivity [3,4]. Injuries comprise a major portion of the global burden of disease among adolescents [1,2,5]. Injuries sustained while playing sports – whether organized or non-organized recreational activities – are extremely common in this population [6]. However, the extent to which sports injuries contribute to the global burden of injury is poorly documented. Large school-based cohort studies, injury databases, and surveillance systems have provided some information on the incidence of sports injuries in high-income countries (HICs) [7–12], but comparable studies from low- and middle-income countries (LMICs) are lacking [6,13].
Given the paucity of information on sports injuries in LMICs, especially those affecting adolescents, we sought to estimate the burden of sports injuries among adolescents in Africa using existing survey data from schoolchildren in several African nations. Estimating the burden of sports injuries across countries and regions is uniquely challenging given the wide country-to-country variability in types of sports played, the existence of organized versus non-organized sports, and different rates of sports participation across gender, age, and socioeconomic strata. Furthermore, it is important to note that there are virtually no high-quality data on sports injuries in LMICs; therefore, despite significant methodological limitations, the work presented here may serve to guide further studies to better describe and quantify the true burden of sports injuries in Africa and other LMICs.
2. MATERIALS AND METHODS
2.1. Description of Survey and Study Population
This study relied on publicly available data from the World Health Organization (WHO) Global School-Based Health Survey (GSHS) (accessible at http://www.who.int/chp/gshs/en/). The GSHS is a school-based surveillance project whose aim is to assess behavioral risk factors and protective factors among young people aged 13–17 years old. The survey methodology has been extensively described elsewhere [14]. To summarize, survey data were collected via a two-stage cluster sample design. Schools within each surveyed country were initially selected with a probability proportional to their reported enrollment size. Classes were then randomly selected and all students in selected classes were eligible to participate. Self-administered questionnaires were completed during one classroom period under the supervision of trained survey administrators.
2.2. Data Collection
For the purposes of this study, only GSHS data on unintentional injuries and violence were considered. Specifically, data on two questions were abstracted. For the first question, study participants were asked, “During the past 12 months, how many times were you seriously injured?” A “serious injury” was defined as an injury that caused the child to miss at least one full day of usual activities (such as school, sports, or a job) or required treatment by a doctor or nurse. Participants were able to indicate either “no times,” “one time,” “two times,” continuing up to “twelve or more times.” For the second question, study participants were asked, “During the past 12 months, what were you doing when the most serious injury happened?” Eight options were provided, including: “playing or training for a sport” and “walking or running, but not as part of playing or training for a sport.” Of note, this question only referred to the “most serious” injury among all the possible serious injuries sustained by each child. Thus, it is possible that a child’s sports injury would be unrepresented by this question if it were not the most severe injury sustained over a one year period. Although these questions were the same across surveys whenever they were posed, some country surveys did not ask questions related to injury.
Survey codebooks from all available African nations were reviewed to identify whether surveys collected data on injury etiology. We included all surveys that collected data on serious injuries and their etiologies and excluded those that did not. In cases of multiple surveys conducted over different years, the most recent survey was used.
We obtained raw data files from every included African country. Data on the numbers of males and females sustaining at least one serious injury, and the subset of those that were attributable to sports, were abstracted. Individuals who did not report gender were excluded from analysis. Country-specific sports injury rates – the proportion of “most serious” injuries attributable to sports – were calculated and stratified by gender. These rates were then weighted by the sample size of each survey to obtain a sample-weighted continent-wide estimate for both male and female adolescents. These estimates were then extrapolated to the male and female populations aged 13–17 for each country in Africa. Population data were obtained from the United Nations Population Division 2015 estimates.
2.3. Statistical Analysis
Descriptive statistics were used to present sample characteristics. A Pearson’s chi-square test was used to determine associations between gender and injury rates among each sample. All tests were two-sided tests with a level of significance of α ≤ 0.05. Data analyses were performed using STATA 14.1 (StataCorp, College Station, TX).
3. RESULTS
3.1. Overview of Surveys
GSHS data were available from 22 African countries (Algeria, Benin, Botswana, Djibouti, Egypt, Ghana, Kenya, Libya, Malawi, Mauritania, Mauritius, Morocco, Namibia, Senegal, Seychelles, Sudan, Swaziland, Tanzania, Tunisia, Uganda, Zambia, and Zimbabwe). Of these, 14 included data on serious injuries attributable to sports (Botswana, Djibouti Egypt, Ghana, Kenya, Libya, Mauritius, Morocco, Swaziland, Tanzania, Tunisia, Uganda, Zambia, and Zimbabwe). The surveys in Africa were conducted over the years 2003–2014. Survey data from these countries represented a total of 21,858 males and 24,691 females, with an additional 888 individuals excluded for not reporting gender (Fig. 1).
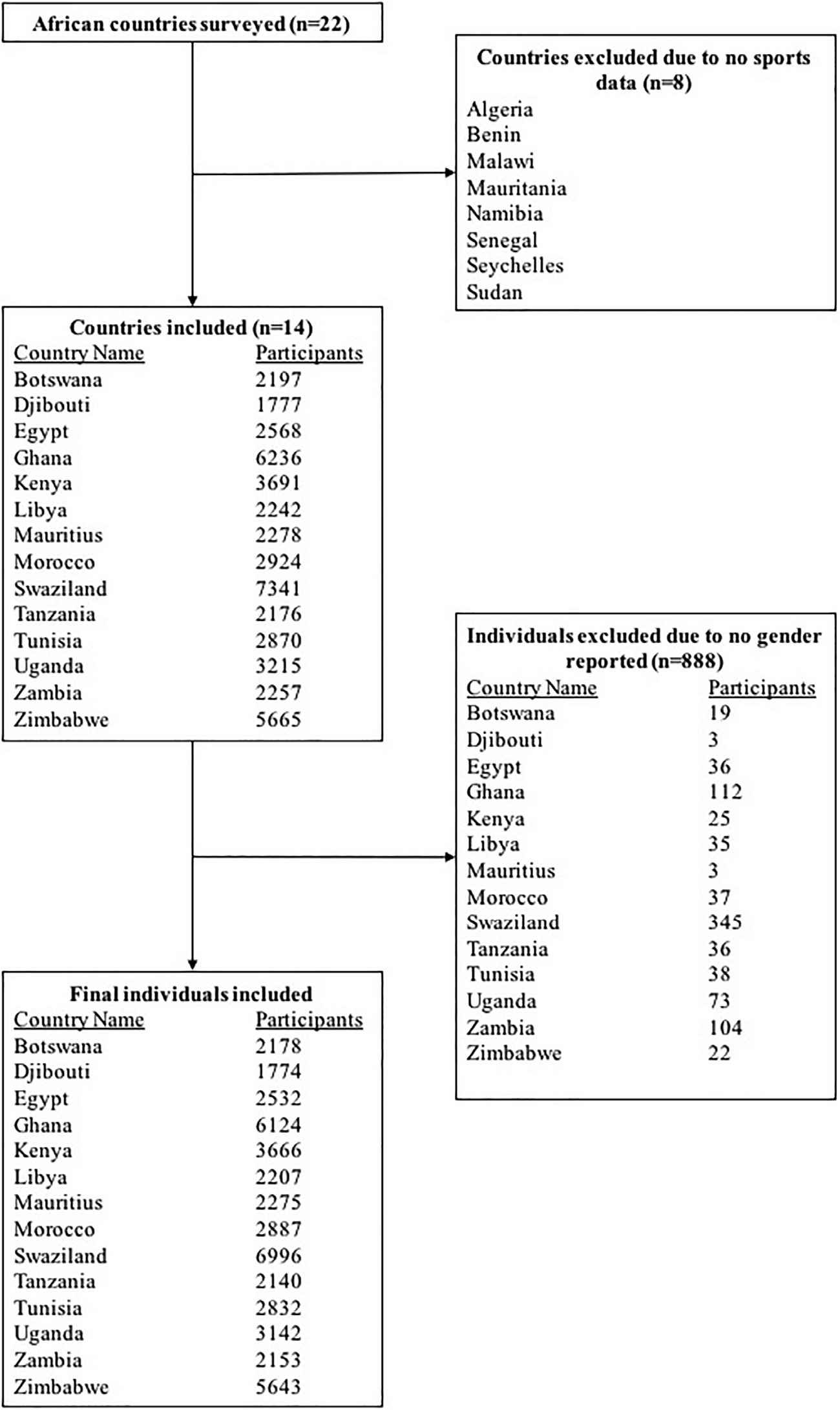
Study flowchart demonstrating numbers of countries and participants included.
3.2. Sports Injury Rates
Gender-stratified sports injury rates for the 14 included countries are summarized in Table 1. The percentage of individuals sustaining at least one serious sports injury ranged from 13.5% to 38.1% for males and 5.2% to 20.2% for females. Males were more likely than females to sustain at least one serious sports-related injury in 13 of the 14 sampled countries (P < .01 for all but one country). Weighted average rates of sustaining at least one serious sports injury for males and females were 23.7% (95% CI 23.1%–24.2%) and 12.5% (95% CI 12.1%–12.9%), respectively. When these rates were applied to the adolescent populations of every African country, an estimated 15,477,798 (95% CI 15,085,955–15,804,333) males and 7,943,625 (95% CI 7,689,429–8,197,821) females in Africa sustained at least one serious sports injury per year. In total, an estimated 23,423,181 (95% CI 22,546,829–24,353,815) adolescents in Africa sustained at least one sports injuries over a one-year period. A sensitivity analysis was also performed by excluding countries with surveys prior to 2007 and found no significant differences in the injury estimates.
| Country | Survey year | Total number of surveyed males | Total number of surveyed females | Percentage of males sustaining at least one sports injury | Percentage of females sustaining at least one sports injury | P value |
|---|---|---|---|---|---|---|
| Botswana | 2005 | 979 | 1199 | 25.5 (22.8–28.4) | 17.6 (15.5–19.9) | <.0001 |
| Djibouti | 2007 | 1013 | 761 | 20.6 (18.2–23.3) | 14.7 (12.3–17.4) | .001 |
| Egypt | 2011 | 1182 | 1350 | 38.1 (35.3–40.9) | 15.2 (13.3–17.2) | <.0001 |
| Ghana | 2007 | 3207 | 2917 | 28.8 (27.2–30.4) | 20.2 (18.7–21.7) | <.0001 |
| Kenya | 2003 | 1784 | 1882 | 22.6 (20.7–24.6) | 16.2 (14.6–17.9) | <.0001 |
| Libya | 2007 | 948 | 1259 | 19.5 (17.0–22.2) | 7.8 (6.4–9.4) | <.0001 |
| Mauritius | 2007 | 1118 | 1157 | 22.9 (20.5–25.5) | 7.6 (6.1–9.3) | <.0001 |
| Morocco | 2010 | 1514 | 1373 | 20.3 (18.3–22.5) | 5.2 (4.1–6.5) | <.0001 |
| Swaziland | 2003 | 2526 | 4470 | 19.7 (18.2–21.3) | 6.9 (6.2–7.7) | <.0001 |
| Tanzania | 2014 | 1026 | 1114 | 13.5 (11.5–15.8) | 9.8 (8.1–11.7) | .007 |
| Tunisia | 2008 | 1379 | 1453 | 18.5 (16.5–20.6) | 6.1 (4.9–7.5) | <.0001 |
| Uganda | 2003 | 1615 | 1527 | 30.4 (28.2–32.7) | 18.0 (16.1–20.0) | <.0001 |
| Zambia | 2014 | 1052 | 1101 | 22.0 (19.5–24.6) | 19.4 (17.1–21.9) | .149 |
| Zimbabwe | 2014 | 2515 | 3128 | 22.7 (21.1–24.4) | 13.0 (11.9–14.2) | <.0001 |
| Total | 21858 | 24691 | 23.7 (23.1–24.2)* | 12.5 (12.1–12.9)* |
Calculated as weighted averages based on relative sample sizes of country surveys.
Overview of included surveys and gender-stratified numbers of adolescents sustaining at least one sports injury over a one year period.
4. DISCUSSION
In this modeling study based on WHO GSHS survey data, we estimated that over 23 million African adolescents between the ages of 13 and 17 years old sustained at least one serious sports injury over a one-year period. Although this study is purely descriptive, it quantifies a significant burden of disease due to sports injury and highlights an area where additional research is needed to more precisely define this burden.
Our findings highlight three key points. First, the injury incidence due to sports among African adolescents is high, with over 23 million adolescents sustaining at least one serious sports injury over a one-year period. This is consistent with evidence from past studies demonstrating that sports are the most common cause of injury in adolescents in LMICs and HICs [14,15]. Second, injury frequency varies significantly between males and females. In fact, the weighted average sports rates of at least one serious sports injury among males were nearly twice the rates among females (23.8% versus 12.4%). Moreover, males were significantly more likely than females to sustain at least one sports injury in all but one of the surveyed countries. This is consistent with another study that found that boys had a higher all-cause injury rate in 40 of 47 LMICs [6]. Third, injury rates vary widely between countries. For example, in Tanzania, the rates for males and females were 13.5% and 9.8% while comparable rates in Uganda were 30.4% and 18.0, respectively.
The nature of sports injuries in LMICs is likely different from that in HICs. One study of adolescent injury in four LMICs across three continents suggested that sports-related injuries in LMICs are unique from sports injuries in HICs because they are influenced by poor infrastructure (e.g., children playing sports on uneven terrain may get injured more easily) and compounded risks (e.g., roads are common places for children to play non-organized sports in LMICs, thereby increasing the risk of motor vehicle accidents) [16]. Additionally, due to the limited availability of appropriate and timely medical care, the impact of a given sports injury in a low-income country may be more severe than that in a high-income country. For example, a tear of the anterior cruciate ligament (ACL) – a common injury among adolescents in competitive sports – often requires surgical repair and extended knee immobilization, followed by physical therapy [10]. Without appropriate surgery and follow-up, the injured adolescent may become permanently disabled, thus less able to attend school and/or provide needed labor to support a family [17].
Our study has multiple limitations. The GSHS surveys do not capture type of sport played, type of injury, how the injury was managed, or type of school (e.g., public, private, urban, rural, etc.). They also represent a limited sample: of over 50 diverse African countries with different socioeconomic backgrounds, schooling patterns, and sports practices, GSHS surveys were performed in 22 countries and only 14 of those reported data on injuries attributable to sports. The remaining 8 surveyed countries did not collect any information on sports-attributable injuries. Eastern Africa and Northern Africa are relatively well represented compared to West Africa and Central Africa. Additionally, the numbers of students surveyed in each country are not proportional to the adolescent populations of the countries or their respective rates of school attendance, so these surveys may not be representative of the entire countries. The survey period is also wide – from 2003 to 2014 – so injury results from different time periods may not be directly compatible due to geopolitical and socioeconomic changes over time. In summary, consolidating these data into an aggregate pool to create sample-weighted sports injury rates carries significant risk of oversimplification of a complex estimation; however, the limited available data precluded the use of a more rigorous method of modeling incidence rates such as multivariable Poisson regression based on multiple relevant covariates. Therefore, the results in this study serve as a first step in better understanding the burden of sports injuries among adolescents in Africa.
Our study may also be subject to information bias. In the WHO GSHS survey, the question assessing whether an injury was due to sports was: “What were you doing when you were injured?” It is also important to note that the survey relied on a student’s recall over one year, even though longer recall periods are associated with a higher rate of underestimation and misreporting of serious injuries [18]. Additionally, some students may overreport or underreport injuries due to a variety of social factors.
Due to the nature of the WHO GSHS surveys being conducted among schoolchildren aged 13–17, our study may be subject to selection bias. Specifically, if school attendance is associated with a different risk of injury compared to not attending school, then selection bias may affect the validity and generalizability of our findings. Moreover, school attendance may also be associated with a different risk of playing sports which may further contribute to selection bias.
Lastly, our study should not be interpreted as an estimate of cumulative incidence or incidence rate. These datasets report whether a given child experienced at least one serious injury, with the most serious being attributable to sports. They do not report the number of injuries sustained within a given year and do not account for the possibility of multiple injuries. Moreover, they do not report the cause of every serious injury; rather, they only report the cause of the most serious injury.
Although this study is subject to substantial methodological limitations, it is important to note that there are virtually no high-quality data that describes the extent of sports injuries in African countries or other low-income regions. This study serves as an important initial step that can guide additional studies assessing the burden of sports injuries in LMICs. The objective of this study is not to guide resource allocation or policy recommendations; rather, it is to highlight the lack of useful data on sports injuries and the need for additional studies with more rigorous data.
5. CONCLUSIONS
Our study sought to estimate the number of adolescents in Africa sustaining at least one serious sports-related injury over a one year period. Despite methodological limitations, our study suggests that over 23 million African adolescents experience a sport-related injury on a yearly basis. These findings highlight the absence of useful data on sports injury epidemiology in Africa and provide a foundation upon which additional research can be performed.
ACKNOWLEDGEMENT
None.
REFERENCES
Cite this article
TY - JOUR AU - Drake G. LeBrun AU - Julius del Rosario AU - John D. Kelly AU - Sherry M. Wren AU - David A. Spiegel AU - Nyengo Mkandawire AU - Richard A. Gosselin AU - Adam L. Kushner PY - 2018 DA - 2018/12/31 TI - An Estimation of the Burden of Sports Injuries among African Adolescents JO - Journal of Epidemiology and Global Health SP - 171 EP - 175 VL - 8 IS - 3-4 SN - 2210-6014 UR - https://doi.org/10.2991/j.jegh.2017.10.010 DO - 10.2991/j.jegh.2017.10.010 ID - LeBrun2018 ER -