
Assessment of vitamin D levels, awareness among Lebanese pharmacy students, and impact of pharmacist counseling
- DOI
- 10.1016/j.jegh.2016.09.001How to use a DOI?
- Keywords
- Awareness; Counseling; Pharmacist; Vitamin D
- Abstract
Vitamin D inadequacy, frequently underdiagnosed, affects people of all age groups worldwide. This prospective study aims at determining the percentage of inadequate vitamin D levels among students and evaluating the impact of pharmacist counseling on raising the awareness of the importance of sun exposure and adequate vitamin D intake. A total of 160 university students were recruited. Blood samples were taken to check the vitamin D, calcium, and phosphorous levels. Vitamin D levels ⩽30 ng/mL were defined as inadequate. Scores were given to the questions and aimed at gathering patient knowledge about vitamin D before and after pharmacist counseling. A total of 115 (71.87%) patients had vitamin D levels <30 ng/mL, with a mean vitamin D serum level of 16.80 ± 5.85 ng/mL. The mean level of calcium was 9.51 ± 1.23 mg/dL and, of phosphorus 3.62 ± 0.95 mg/dL. The mean difference in the knowledge score of the recommended daily amount of vitamin D before and after pharmacist counseling was 2.81 versus 5.88 (p < 0.001). Concerning patient education for diseases and drugs that affect vitamin D levels, pharmacist counseling was effective in raising the awareness (p < 0.001). Given that vitamin D inadequacy is linked to many disease progressions, it is important that health professionals provide interventional strategies and education measures to correct inadequate levels in patients of all age groups.
- Copyright
- © 2016 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Vitamin D, the sunshine vitamin, plays a physiological role in maintaining the extracellular calcium ion levels in the body. Extracellular calcium is essential for the functioning of many metabolic processes and neuromuscular activities. Vitamin D influences calcium levels by controlling its absorption from the intestine, through direct effects on bone and also through its effects on parathyroid hormone secretion [1,2].
Vitamin D plays an essential role in various metabolic processes and neuromuscular activities [3–6]. Bones constitute an important part of the skeletal system that requires a balanced store from vitamin D, calcium, and phosphorus. It plays an important role in promoting enterocyte differentiation and the intestinal absorption of calcium and phosphorous, thereby promoting bone mineralization. Vitamin D is not an essential vitamin because it can be obtained through nutrition or by endogenous production through the cutaneous involvement under the action of sunlight [7]. Vitamin D3 or cholecalciferol, after formation in the skin, and vitamin D2 (ergocalciferol) or D3, either from dietary sources or supplements, undergo first hydroxylation in the liver, to form 25-hydroxyvitamin D3 [25 (OH) D], and then the second hydroxylation in the kidneys to form 1,25 dihydroxyvitamin D3 (activated form), which is responsible for exerting the biologic actions. Vitamin D3 is more potent than D2 because the latter has lower affinity to the binding proteins and thus has rapid clearance. Therefore, the recommendation is to prescribe Vitamin D3 to effectively increase the serum levels. Among the various forms of vitamin D, the level of 25 (OH) D is the best indicator of vitamin D stores, since it is the major circulating form of vitamin D and has a half-life around 2–3 weeks.
The normal vitamin D range varies between populations and is dependent upon many factors. Total body vitamin D stores can be assessed by measuring the serum concentration of total 25 (OH) D. In adults, vitamin D deficiency is defined as a serum 25 (OH) D level <20 ng/mL, insufficiency as a serum 25 (OH) D level of 20–30 ng/mL, and sufficiency levels above 30 ng/mL [8]. The clinical presentation of vitamin D deficiency occurs when the levels are <25 ng/mL, which can cause bone pain, fracture, and muscle weakness. The 25 (OH) D cut-offs to define this condition vary and have recently been defined as desirable level at 20 ng/mL (50 nmol/L), and the Endocrine Society Guidelines set at 30 ng/mL (75 nmol/L) [9,10].
Vitamin D inadequacy is due to many factors such as age (80 years), race (nonwhite), body mass index >30 kg/m2, limited exercise, inadequate sun exposure, poor diet, drugs that affect vitamin D metabolism, and diseases that interfere with its absorption [9]. Vitamin D inadequacy, emerging as a major health problem globally, is a highly prevalent condition, affecting people across all age groups [12–14]. Despite the adequate sunshine in Middle Eastern countries and more particularly in Lebanon, the incidence of hypovitaminosis D is high in all age groups, even in young individuals [15,16].
Several studies conducted all over the world, and particularly in Middle Eastern countries, mainly Lebanon, have shown low vitamin D levels in school children and postmenopausal women [17–19]. There is a high risk of low vitamin D levels in the Lebanese population since there is a lack of vitamin D fortified food. The supportive evidence indicates that low vitamin D levels are associated with increased rates of rickets, osteomalacia, and altered bone mass. Because of the lack of data on vitamin D status in Lebanese pharmacy students and limited evidence of the effectiveness of pharmacist counseling, this study was conducted to assess both vitamin D levels and awareness in healthy university pharmacy students and to evaluate the impact of pharmacist intervention on raising the awareness.
2. Methods
2.1. Study design and study population
This is an observational prospective multicenter study conducted at the Lebanese International University, a private university, in Beirut. The information was obtained from the students at each site. Institutional review board approval from the involved site was obtained. All participants gave informed consent for the enrollment prior to study conductance.
In this study, 250 pharmacy students aged >18 years were approached and screened for eligibility via mails and flyers; posters were also used as recruitment tools. The participants needed to be healthy with no signs and symptoms of low vitamin D levels. Furthermore, those with musculoskeletal pain, malignancy, pregnancy and lactation, intestinal malabsorption, intake of medications that affect vitamin D (supplements, enzyme inducers), or any evidence of liver, kidney, or gastrointestinal disease were excluded from the study.
2.2. Data collection and measurement
One peripheral nonfasting blood sample was taken from each participant by a professional medical laboratory technician. The serum was collected in special tubes, separated after complete centrifugation within 1 h of puncture and stored in a cooler to be sent for serum 25 (OH) D measurements. Only one sampling was performed for each individual. Serum calcium and phosphorous levels were also measured. The serum 25 (OH) D levels were measured using the enzyme-linked immunosorbent assay technique. For staging serum 25 (OH) D, cut-off values <30 ng/mL were defined as inadequate. A questionnaire seeking demographics on patients’ weight, height, social history, and lifestyle practice was completed. Life style habits that were assessed included exercise type and duration, duration of sun exposure, application of sunscreens, consumption of food rich in calcium including the type and frequency, and the intake of any supplement. The questionnaire also included assessment of the patient’s knowledge about the factors that ensure adequate vitamin D levels. The participants responded to the questionnaire without any outside interference initially where a score was given to each correct answer. The areas of assessment were mainly centered about the recommended daily allowance, food enriched with vitamin D, factors that interfere with adequate vitamin D activation, and metabolism. A second assessment was then done on the same individuals to evaluate patient knowledge about the same areas after the pharmacist counseling. Moreover, the strategy was followed after counseling where a score was assigned to each correct response. The counseling performed by the pharmacist was given to all participants in one group and aimed at raising the patient’s knowledge and awareness about factors that affect vitamin D levels.
2.3. Statistical analysis
The statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) (version 21.0), IBM, New York, USA. Descriptive analysis was done for demographic data. Continuous variables were expressed as mean ± standard deviation and categorical variables as numbers and percentages. Paired sample t test was used to compare the scores between the pre- and post-pharmacist counseling. Results were considered statistically significant for a p value <0.05. For multivariate analysis, a stepwise backward likelihood ratio logistic regression was performed for vitamin D level categories as the dependent variable, and the assessed social habits such as alcohol history, smoking history, water pipe smoke, exercise, sun exposure, and use of sunscreen as independent variables.
3. Results
3.1. Sociodemographic results
Out of the 250 questionnaires distributed, 160 were collected back (64%) with an age range between 21 years and 24 years. Sociodemographic factors are summarized in Table 1. The mean age of participants was 23.24 ± 4.24 years and 56.9% were males. The body mass index was categorized into 16.3% underweight, 43.1% normal, 21.9% overweight, and 18.8% obese, as illustrated in Fig. 1. For allergies, two (1.25%) patients reported an allergy to penicillin. Around half of the participants were active smokers having the lowest level of measured vitamin D of 10.54 ng/mL, whereas previous alcohol intake participants had the highest levels of 21.78 ng/mL (Table 2).
| Characteristics | No. (%) |
|---|---|
| Total | 160 |
| Gender | |
| Male | 91 (56.9) |
| Female | 69 (43.1) |
| Age (y), mean ± SD | 23.24 ± 4.24 |
| BMI (kg/m2) | |
| 15–20 | 26 (16.3) (underweight) |
| 20–25 | 69 (43.1) (normal) |
| 25–30 | 35 (21.9) (overweight) |
| >30 | 30 (18.8) (obese) |
BMI = body mass index (calculated as weight in kg divided by the square of height in meters); SD = standard deviation.
Demographic characteristics of study participants.
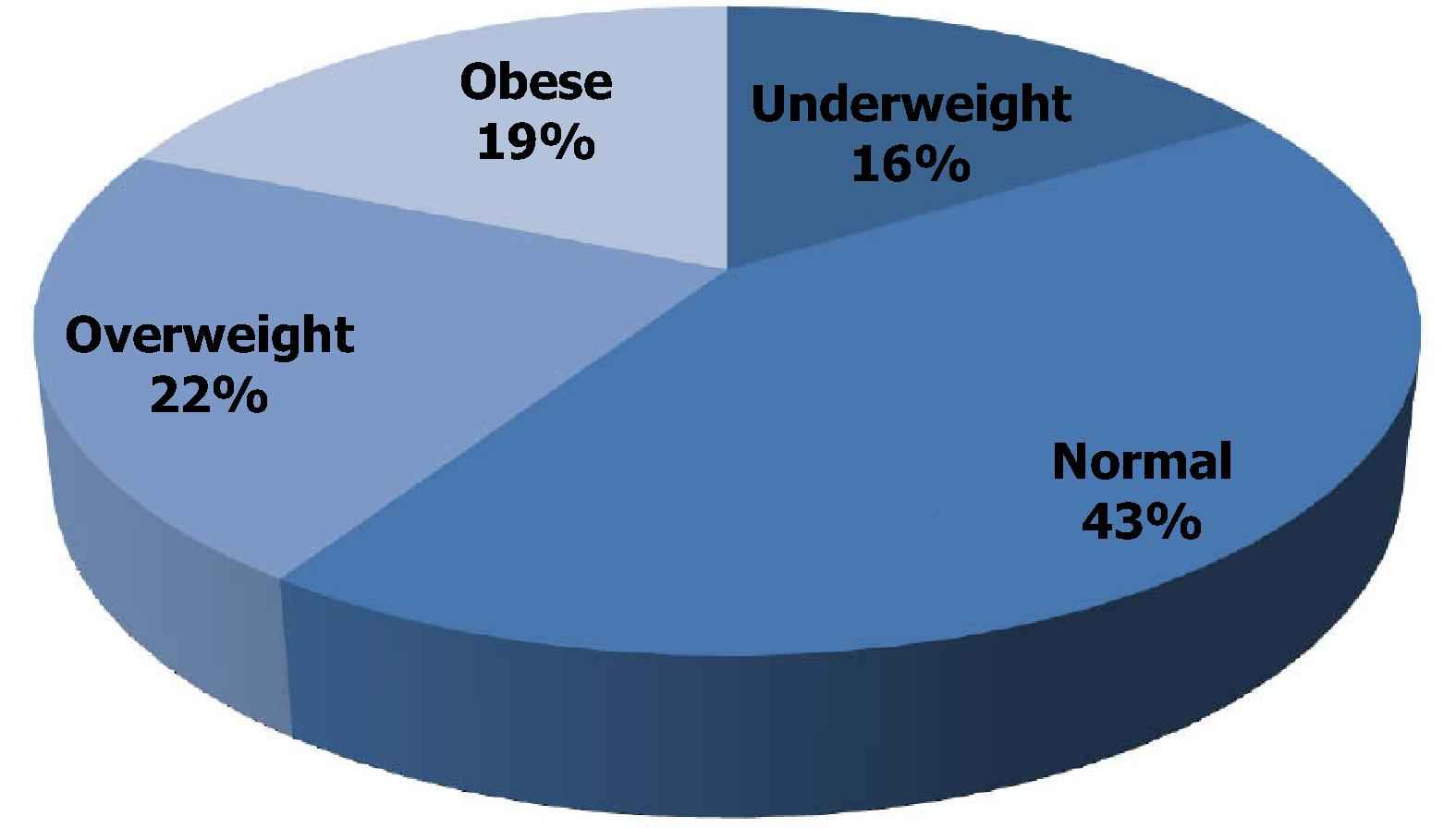
Distribution of Body Mass Index among the participants.
| Social habits | No. (%) | Vitamin D level (ng/mL), mean ± SD |
|---|---|---|
| Previous smoker | 50 (31.25) | 20.98 ± 5.35 |
| Active smoker | 80 (50) | 10.54 ± 2.35 |
| Water pipe smoke | 8 (5) | 12.50 ± 3.54 |
| Previous alcohol intake | 20 (12.5) | 21.78 ± 4.78 |
| Active alcohol intake | 15 (9.38) | 11.38 ± 1.85 |
SD = standard deviation.
Summary of the various social habits with vitamin D levels of the study participants.
In the study group overall, around 90.6% underwent three to five activity sessions per week, and 81.25% for 30–50 min duration in each activity. Almost 62% of the participants had sun exposure of 15–30 min/d. As for the consumption of calcium rich food, only 25% of the study group consumed fish once a day and around 87% vegetables, which was the highest frequency for food consumption (Table 3).
| Lifestyle habits | No. (%) |
|---|---|
| Exercise (/wk) | |
| 3–5 times | 145 (90.63) |
| 30–50 min of exercise | 130 (81.25) |
| Sun exposure of 15–30 min/d | 100 (62.5) |
| Consumption of calcium rich food/d | |
| Fish | 40 (25) |
| Dairy products | 120 (75) |
| Cereals | 100 (62.5) |
| Vegetables | 140 (87.5) |
| Vitamin D supplements | 10 (6.25) |
Summary of the different lifestyle habits of the study participants.
3.2. Biochemical markers
Of all screened patients, 115 had vitamin D levels <30 ng/mL, with a mean serum 25 (OH) D level of 16.80 ± 5.85 ng/mL. Of the deficient patients, 44 (38.26%) were male and 71 (61.74%) female. The mean level of calcium was 9.51 ± 1.23 mg/dL and the mean level of phosphorus was 3.62 ± 0.95 mg/dL, as illustrated in Table 4. The serum levels of calcium and phosphorus were normal in the studied population; the reason for this assessment is that vitamin D level is affected by the level of either mineral alone. However, in this population they were still normal, since only low levels of vitamin D for prolonged periods of time will affect calcium and phosphorus.
| Bio | |
|---|---|
| Vitamin D (ng/mL) | 16.80 ± 5.85 |
| Deficient ⩽20 | 68 (42.50) |
| Insufficient 20–30 | 47 (29.38) |
| Sufficient ⩾ 30 | 45 (28.13) |
| Calcium (mg/dL) | 9.51 ± 1.23 |
| Phosphorous (mg/dL) | 3.62 ± 0.95 |
Data are presented as mean ± SD or n (%).
SD = standard deviation.
Clinical laboratory characteristics of the study participants.
Fig. 2 shows the distribution of serum 25 (OH) D concentrations in the three categories of study participants: 68 cases (42.5%) were deficient, 47 cases (29.38%) insufficient, and 45 cases (28.13%) were found to be sufficient.
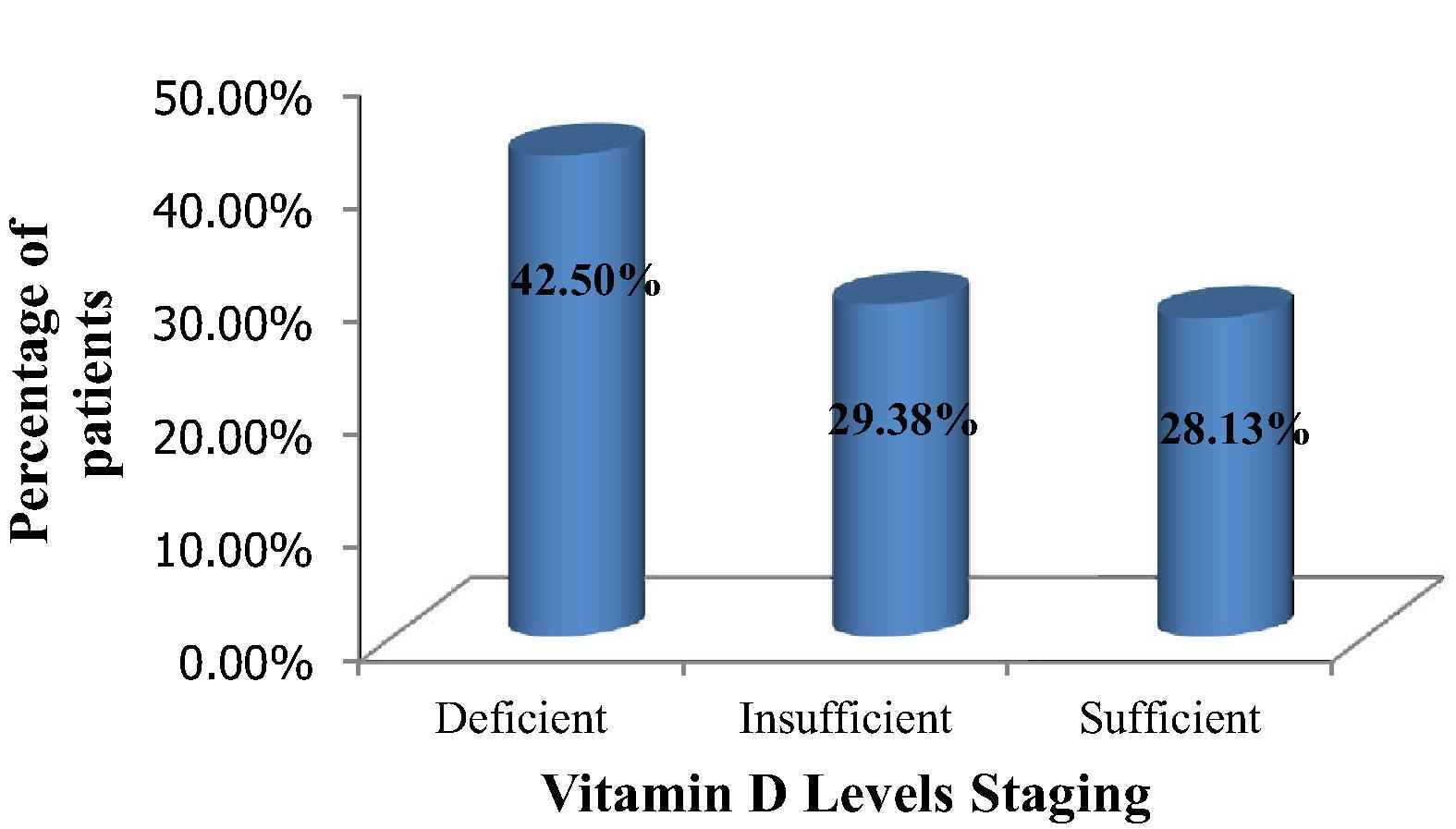
Distribution of the participants according to vitamin D levels.
3.3. Smoking and alcohol characteristics
None of the students smoked cigarettes, however 23.1% smoked water pipes, with a mean of 2.19 ± 0.73 water pipes/d, and a mean duration of 2.64 ± 1.20 years of smoking. Some 5.6% were active alcohol drinkers, with an average of three glasses per week over a mean duration of 6 years.
3.4. Impact of pharmacist counseling on patient education
Patient awareness was first assessed before pharmacist counseling in the following areas: recommended daily allowance, sun exposure per day, types of food rich in vitamin D focusing on dairy products, and fish. Furthermore, patients’ knowledge about vitamin D products, diseases, and drugs that affect vitamin D levels, and factors that limit the effect of sun exposure on vitamin D activation were increased after pharmacist’s counseling and intervention.
Pharmacist counseling was performed to increase patient education and raise awareness; the same questionnaire was distributed 2 months after pharmacist’s counseling following the baseline assessment. Scores were given post counseling and the results are illustrated in Table 5. The difference in the scores obtained before and after pharmacist counseling was significant across all areas of patient education, as illustrated in Table 5.
| Areas of patient assessment | Before pharmacist counseling (mean ± SD) | After pharmacist counseling (mean ± SD) | p |
|---|---|---|---|
| RDA and food rich in vitamin D | 2.8 ± 1.6 | 5.8 ± 2.6 | <0.001 |
| Diseases affect vitamin D | 1.0 ± 1.1 | 2.79 ± 1.6 | <0.001 |
| Drugs affect vitamin D | 0.7 ± 1.0 | 3.1 ± 1.6 | <0.001 |
| Factors affect sun exposure effect on vitamin D | 1.2 ± 1.0 | 2.4 ± 0.7 | <0.001 |
RDA = recommended daily allowance; SD = standard deviation.
Scores obtained both before and after pharmacist counseling.
A total of 62 of the vitamin D-deficient patients initiated vitamin D supplementation post pharmacist counseling. After the pharmacist intervention, females scored significantly higher than males for knowledge about the different factors that decrease vitamin D levels (p < 0.001). As for smoking and alcohol consumption, these patients scored significantly higher post pharmacist counseling (p < 0.001).
3.5. Multivariate analysis for vitamin D levels
Backward logistic regression results for vitamin D levels are shown in Table 6. The following variables were assessed: alcohol history, smoking history, water pipe smoke, exercise, sun exposure, and use of sunscreen. These variables were able to explain 23.3% of the model (Nagelkerke R2 = 0.233).
| Social habits | p-value | OR | 95% CI (lower and upper limit) |
|---|---|---|---|
| Smoking history | 0.03 | 3.12 | 1.569–4.715 |
| Alcohol history | 0.001 | 2.33 | 1.59–3.766 |
| Water pipe smoke | 0.002 | 5.43 | 1.488–8.988 |
| Exercise | 0.04 | 0.63 | 0.167–1.377 |
| Sun exposure | 0.05 | 0.54 | 0.148–0.988 |
| Sunscreen use | 0.04 | 1.99 | 0.866–3.978 |
CI = confidence interval; OR = odds ratio.
Multivariate analysis. Linear regression results with vitamin D level taken as dependent variable.
Previous and active alcohol intake were significantly associated with low vitamin D levels, increasing the risk of inadequate levels by more than two times [p = 0.001; odds ratio (OR) = 2.33; confidence interval (CI) 1.59–3.766]. The risk of low vitamin D levels was increased with cigarette smoking and water pipe smoking by more than three times and five times, respectively (OR = 3.125; p = 0.03; CI 1.569–4.715 and OR = 5.43; p = 0.002; CI 1.488–8.988, respectively). Furthermore, the risk of low vitamin D levels was also significantly increased with sunscreen application by almost two times (p = 0.045; OR = 1.99; CI 0.866–3.978).
Regarding exercise and sun exposure, these two factors were shown to be protective against developing inadequate vitamin D levels with an OR = 0.630, p = 0.04; CI 0.167–1.377 and OR = 0.543, p = 0.057; CI 0.148–0.988 respectively (Table 6).
4. Discussion
This study was conducted among university students in Lebanon to assess the prevalence of inadequate vitamin D levels. The incidence of low vitamin D levels is highly prevalent among all populations, as was shown in different studies on the Lebanese population [16,17]. This is in agreement with another study conducted in Europe [20–22]. A study conducted in Beijing showed that vitamin D deficiency and severe deficiency is highly prevalent among females aged <20 years and >80 years [23]. The incidence of low vitamin D level, defined as 25 (OH) D < 30 ng/mL, is high involving 71.9% of this healthy young population who resided in the Middle East at latitude 15°–36° N. The results of this study revealed also that a very high proportion of apparently healthy adults are at risk of developing chronic disease states related to low vitamin D levels. Optimum sunlight exposure and lifestyle modifications can help prevent the deficiency state. Clinical utility of vitamin D supplementations and vitamin D food fortifying programs to avoid complications of this disease would be highly desirable.
A suggested reasonable approach is the annual and serial monitoring of 25 (OH) D concentrations in the healthy adult population for early detection, prevention, and follow-up in deficient individuals after supplementation. Traditional risk groups include young children, pregnant women, and elderly persons.
In Middle-Eastern countries, more particularly Lebanon, several studies have shown a high incidence of vitamin D deficiency in young individuals and school children [5,25]. The reason for the high prevalence of vitamin D deficiency in this population is multifactorial. This study was performed on young people, and the main predictors of the hypovitaminosis were female gender, inadequate vitamin D intake, clothing covering all of the body, and inadequate daily sun exposure. The results of this study showed that females are at a higher risk of developing low vitamin D levels, in line with the results of other studies [19,11], but opposite to other studies where men had a higher prevalence of vitamin D deficiency [26].
This study showed a correlation between positive smoking history and low vitamin D levels. This was expected since smoking is an enzyme inducer that increases vitamin D metabolism in the liver, thereby predisposing to inadequate levels, a fact that was demonstrated in the study of Supervía et al. [27]. Indeed, similar results have been previously described in young adults [26,28–31], possibly reflecting that smoking induces an increased activity of liver enzymes [32]. The same applies for water pipe smoking, a common social habit among university students that caused inadequate vitamin D levels among these students. However, to our knowledge, no study has explored that effect. More studies are needed to explore the water pipe and vitamin D correlation in young adults in particular and the national population in general.
Active alcohol intake also led to low levels of vitamin D, which reflects its potent effect on liver induction activity. Our results are opposite to those of Tønnesen et al. [20] who showed that alcohol intake was found to be positively related to a decrease in the relative risk of vitamin D deficiency and to other studies that showed an apparently beneficial effect of alcohol [33–35]. More studies are needed to explore the effects of alcohol on vitamin D levels in young adults.
Insufficient 25 (OH) D intake is another reason for the high prevalence of 25 (OH) D deficiency in the Lebanese population, which is consistent with results of other studies [25,36]. The high prevalence of 25 (OH) D deficiency in young adults in this study can be explained by their lower consumption of vitamin D containing foods such as dairy products and fish. Exercise was a protective factor against developing inadequate vitamin D levels, which is consistent with the finding of Hoge et al. [18].
Exercise and sun exposure were shown to be protective against developing inadequate vitamin D levels. Our results are in line with similar results which reported showing that increasing the time spent exercising is associated with higher vitamin D status [26,29,33,37]. Similarly, in line with our expectations, exposure to sunlight is the major source of vitamin D and would be favorable in maintaining an adequate vitamin D level. The effect of sunlight on cutaneous vitamin D synthesis can be modified by sunscreen [38], as demonstrated in our results.
These results highlight the fact that pharmacist intervention is an important cornerstone in preventing vitamin D deficiency prevalence and raising patient awareness among the various factors that decrease the levels. The results of this study are in agreement with those of a previous study that showed education and communication improves the appropriateness of the request of vitamin D tests [39]. Pharmacists can have a vital role in providing the necessary counseling issues to patients to raise their awareness about how to prevent the risk of low vitamin D levels through lifestyle modifications. The importance of this study is that it highlights the lack of knowledge among young population, which is consistent with another study that concluded that awareness of vitamin D deficiency should be improved across all age groups [40]. The results of this study made it clear that a pharmacist’s intervention raised patient awareness across all the areas of patient education to minimize the deficiency. Thus, pharmacists play an integral role in educating patients about the ways to minimize risk factors for vitamin D deficiency. Other studies are needed to assess the patients’ post counseling status at a larger scale.
4.1. Limitations
The study has many limitations as it was done on a small sample size, which raises the need to perform studies on a larger sample population. In addition, we did not assess whether the females who participated in the study were veiled or unveiled; this might be a cause of low sun exposure and consequently, a low vitamin D level. In addition, the blood samples were collected only once, due to the limited budget of the study. It would be more useful if patients were evaluated at different times of the year to study the effect of seasonal variation. Selection bias might be present since the study was done in a university setting, where the results cannot be generalized to all of the Lebanese patient population. An information bias is possible since the use of a questionnaire in a young population may not always be accurate, with problems in question understanding, and recall gaps. Moreover, it would be interesting to do further studies to compare the effect of the different risk factors on vitamin D levels.
5. Conclusion
This study shows that there is a high prevalence of low vitamin D levels in a group of healthy adults in Lebanon. There is an urgent need for public education about the vital role of vitamin D to minimize the complications of its deficiency. The results of this evaluation highlighted the importance of a structured approach and screening for vitamin D levels in the Lebanese community and emphasized the need for further assessment and interventions targeted at all patients.
This study raised a health concern for the Lebanese population in general. If healthy adults, living in a country with abundant sunshine, specializing in the pharmacy field have this lack of knowledge about vitamin D deficiency, what can we say about the situation among the Lebanese community overall? Pharmacists have the capacity to use their unique perspective concerning drug therapy and collaborate in a multidisciplinary approach to monitor and optimize vitamin D supplementation in all patients, especially those who are at high risk.
Conflicts of interest
The authors have no conflict of interests to declare.
Acknowledgments
The authors are grateful to all persons who helped in data collection and data entry.
References
Cite this article
TY - JOUR AU - Diana Malaeb AU - Souheil Hallit AU - Pascale Salameh PY - 2016 DA - 2016/10/04 TI - Assessment of vitamin D levels, awareness among Lebanese pharmacy students, and impact of pharmacist counseling JO - Journal of Epidemiology and Global Health SP - 55 EP - 62 VL - 7 IS - 1 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2016.09.001 DO - 10.1016/j.jegh.2016.09.001 ID - Malaeb2016 ER -