
Incidence of acute-onset atrial fibrillation correlates with air temperature. Results of a nine-year survey
- DOI
- 10.1016/j.jegh.2013.12.003How to use a DOI?
- Keywords
- Atrial fibrillation; Acute-onset atrial fibrillation; Climate; Temperature; Humidity
- Abstract
Some diseases, such as renal colic, stroke, and myocardial infarction, correlate with seasonality and microclimatic variations. Although evidence is limited and controversial, a correlation between acute-onset atrial fibrillation (AAF) and seasonality has been previously reported. In order to elucidate the possible correlations between weather and incidence of AAF in a country with a temperate climate, the influence of day-by-day climate changes was analyzed based on the number of visits for AAF (defined as onset of symptoms within 48 h) in a large urban Emergency Department (ED) of northern Italy. All the episodes of AAF were retrieved from the hospital’s electronic database during a period of 3287 days (January 2002 to December 2010). Only the cases whose onset occurred within 48 h from the ED visit were selected. The total number of ED visits was 725,812 throughout the observational period. Among these, 3633 AAF cases were observed, 52% of which were males. A slight but significant negative linear correlation was found between the number of AAFs and the daily temperature (R = −0.60; p = 0.001). No correlation was found between the number of AAFs and the daily humidity (R = −0.07; p = 0.2).
- Copyright
- © 2014 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Several lines of evidence indicate that the incidence of some cardiovascular diseases, such as myocardial infarction, heart failure and stroke, is correlated with seasonality and microclimatic variations [1–3]. Additional data seem to demonstrate a climate-dependency of different conditions, such as syncope, psychiatric emergencies, trauma, and, most notably in children, asthma [4–8]. The existence of a strong association between air temperature, relative humidity, and the number of episodes of renal colic in a region with continental, temperate climate has been previously demonstrated [9,10]. At variance with urolithiasis, this seasonal pattern is characterized by a winter peak and a summer trough for cardiovascular diseases. Some other influences attributable to various risk factors are the subjects of ongoing investigation, including environmental, neuroendocrine, metabolic and lifestyle changes. Atrial Fibrillation (AF) is the most common severe cardiac arrhythmia, which requires early and appropriate management for the elevated cardiovascular mortality and morbidity. It has been clearly established that AF is characterized by a progressively increasing incidence within the ageing population. In a large population study from Denmark, Frost et al. [11] found a significant correlation between the incidence of AF and seasonality, with a higher incidence during the winter. A smaller but well-designed study from Israel by Viskin et al. confirmed the influence of the seasonality, also showing a clear circadian variation [12]. In a 24-h Holter-based study, Watanabe et al. confirmed a similar seasonal variation in a Japanese population [13]. Like other cardiovascular disorders, seasonality seems to be compellingly emerging as an evocative risk factor for atrial fibrillation. Unfortunately, data reported in the literature are still limited and often controversial, showing a high variability among climatic characteristics of different countries [14–17]. In a recent study in hospitalized patients with acute ischemic stroke, Fustinoni et al. showed a higher frequency of AF during colder seasons, with a correlation with the day of ischemic stroke onset. This study has shown very strong data supporting the correlations between air temperature and AF, although limited to a cohort of hospitalized patients [18]. Actually, a variety of different mechanisms may be elicited by cold exposure and hence involved in the triggering of AF, but at present the complex interactions involved need further investigations to be explained. Moreover, low temperature exposure might indirectly decrease the levels of physical activity, induce behavior changes (e.g., increased drinking of alcohol and cigarette smoking), as well as enhance the susceptibility to infections and respiratory diseases. Air pollution has also been associated with the risk of AF, but data are still controversial [19–21]. A single Polish study found a lower incidence of Paroxysmal AF (PAF) in females when sunshine levels were the lowest [22]. It is noteworthy, however, that in Poland sunshine levels are lower in those months when the temperature is also colder.
In order to better elucidate the potential correlations between weather and incidence of Acute-onset Atrial Fibrillation (AAF) in a country with a temperate climate, the influence of day-by-day climate changes was analyzed based on the number of visits for AAF (defined as the onset of symptoms within 48 h) in the large Emergency Department (ED) of the Academic Hospital of Parma, northern Italy. It is noteworthy that “temperate”, as referred to climate, generally means that the changes in these regions between summer and winter are relatively moderate, rather than extremely hot or cold. Temperate latitudes of the globe lie between the tropics and the Polar Regions. The North Temperate Zone extends from the Tropic of Cancer to the Arctic Circle. The South Temperate Zone extends from the Tropic of Capricorn to the Antarctic Circle. Continental zones are usually located inland, with warmer summers and colder winters. The vast majority of the human population reside in temperate zones (if defined as comprising the subtropics as well), especially in the northern hemisphere because of its greater mass of land [23].
2. Material and methods
All episodes of AAF (both first-diagnosed AF and PAF) were retrieved from the electronic database of the hospital during a period of 3287 days (January 2002 to December 2010). Only the cases whose onset was recorded within 48 h from the ED visit were selected. The patients were residents in town or the immediate neighborhood, i.e., within a 10-km radius from the weather monitoring station. Urban and rural populations were represented in an approximately equal percentage, according to the distribution of the population in the province. The Academic Hospital of Parma is a 1250-bed teaching general hospital, serving a population of about 430,000, and is the only hospital in the area. This hospital has a level 2 Trauma Center and a referral center for stroke and myocardial infarction cases. As such, the ED provides acute cardiac and stroke care as well as trauma care. The population of the region is relatively stable, with the only exception of immigration causing a gain of approximately 0.5% per year. For all the 3287 observed days, the meteorological data referred to the Parma Province were obtained from the ARPA (Agenzia Regionale Prevenzione e Ambiente; Environment and Climate Regional Agency, http://www.arpa.emr.it/sim/?osservazioni_e_dati/dexter) of the Region Emilia Romagna. The site of measurements, located in the town of Parma, was at 10.330313 longitude; 44.808064 north latitude; height 54 mt above sea level. The climate at that site is considered typical of the central-southern Pianura Padana area (the Po river valley): continental with 777 mM precipitation per year, peaking in fall and spring; the peak of the rainy season is in October (averaging 110.2 mM per day), while the driest month is July (averaging 37.6 mM per day). The summer is hot and humid, with peak temperatures of 30–35 °C, whereas the winter is cold, with minimum temperatures seldom being below −20 °C. The mean estimated temperature (with standard deviation) was 13.5 °C (±8.64). The number of days with temperature comprised within one standard deviation was 1902 (i.e., 57.9%). The relative mean humidity in this area was 71% throughout the study period (minimum 28.2% on March 3, 2009 and maximum 99.8% on January 12, 2005) (Fig. 1) [24].
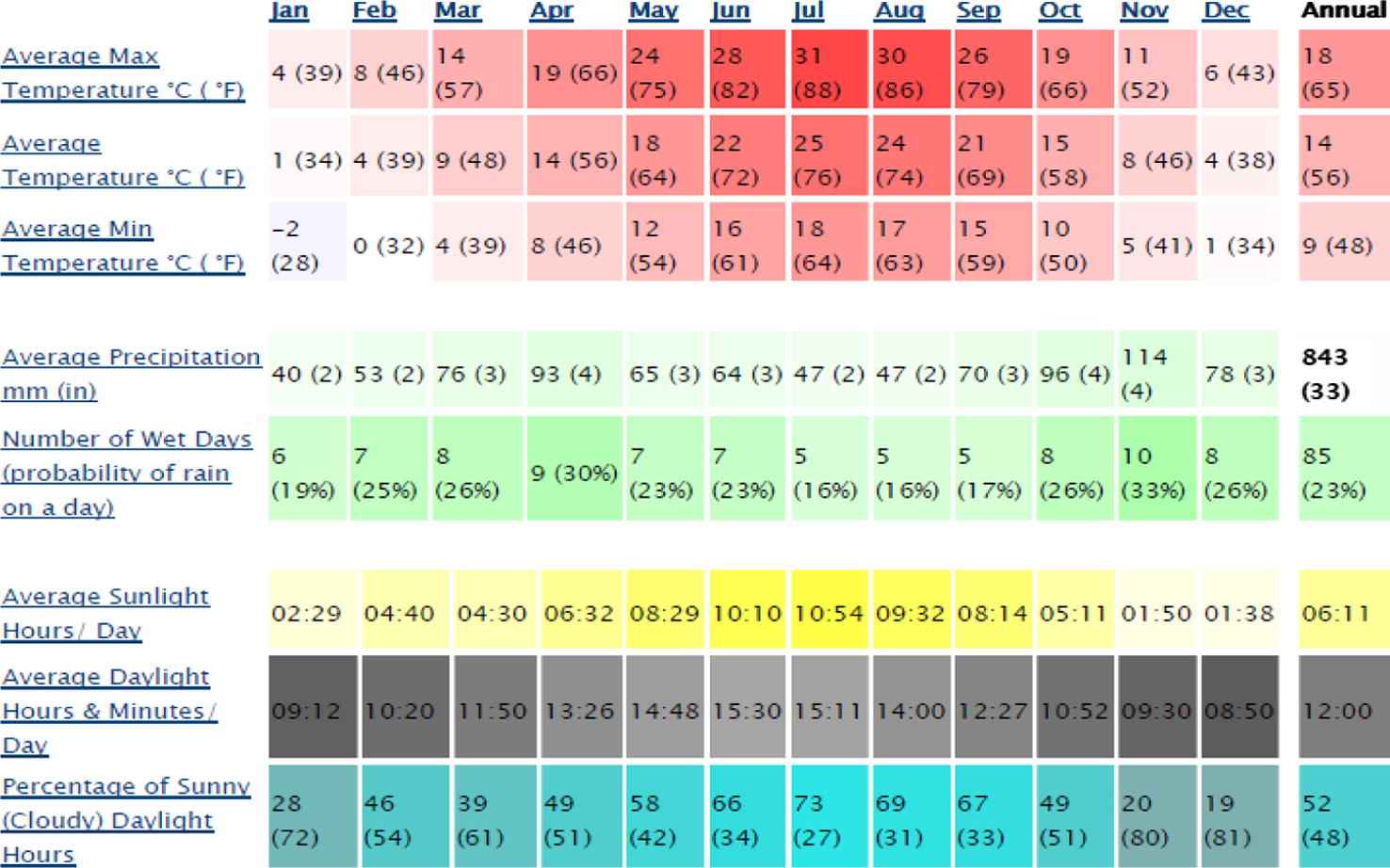
Average weather characteristics of Parma stratified by month [24].
The measurements of air temperature and humidity used for this study were performed on an hourly basis, and the mean temperature and humidity of each single day were then calculated. The chronological data of all visits for AAF were interfaced with the climate data in multiple univariate linear regression analysis, and one multivariate linear regression analysis using the program Mathematica7®. A linear model with assumed independent normally distributed errors was developed, giving a formatted analysis of variance table for the model (ANOVA). The t statistics are the estimates divided by the standard errors. Each p-value is the two-sided p-value for the t statistic and can be used to assess whether the parameter estimate is statistically significantly different from zero. In particular, the following were computed:
- •
The univariate linear regression analysis between the number of visits for AAF and the mean daily temperature (°C).
- •
The univariate linear regression analysis between the number of visits for AAF and the mean daily humidity (%).
- •
The multivariate linear regression analysis among the number of visits for AAF, the mean daily temperature and the mean daily humidity.
All the days were considered for the analysis, including those without recorded episodes of AAF.
3. Results
The ED recorded 725,812 patient visits over the observational period, with an average of 221 patients per day. The total amount of visits increased from 80,538 in 2002 to 83,919 in 2010, thus showing a positive incremental trend. A total of 3633 AAF cases were observed during the study period, 52% males (mean age 63 ± 14 yrs) and 48% females (mean age 71 ± 11 yrs). Considering the whole sample, there were 2.8% of patients that visited more than once, accounting for 12.5% of all visits. The number of patients who were visited for AF showed a similar but larger incremental trend, from 398 in 2002 to 464 in 2010 (with a maximum of 511 in the year 2009), showing some seasonal fluctuation (Fig. 2).
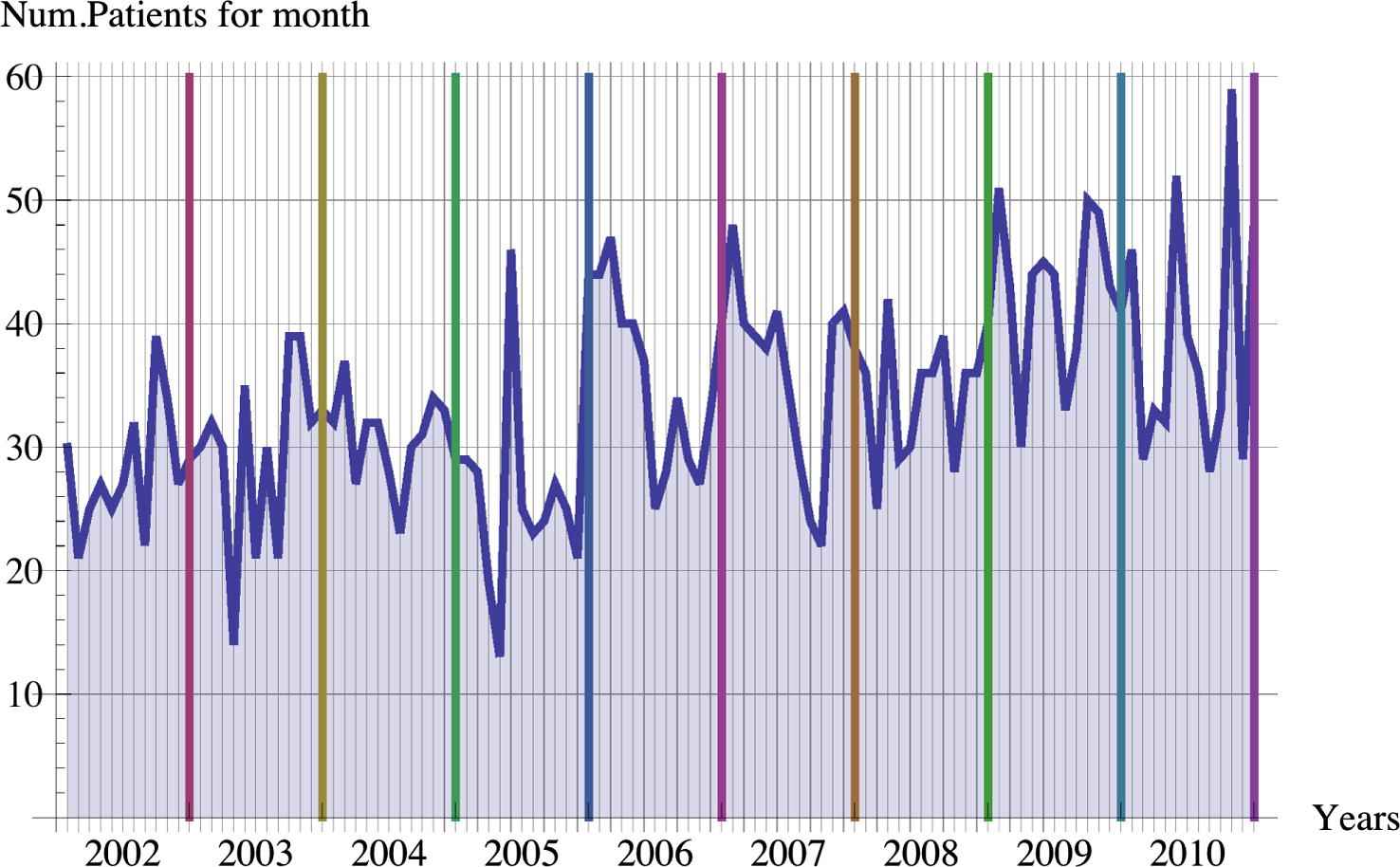
Trend of monthly number of visits for AAF during all the observational periods.
According to the time of day, the peak was observed between 10 and 12 a.m., and the nadir between 5 and 7 a.m. It should be considered, however, that these figures are referred to the presentation time, and not necessarily to the actual onset time of AF. A synthesis of these results is shown in Table 1. A slight but significant negative linear correlation was observed between the number of AAFs and the daily temperature (T) (R = −0.60; p = 0.001). After the study population was partitioned for genders, a similar and significant negative linear correlation was found in males (R = −0.58; p = 0.007), but not in females (R = −0.36; p = 0.060) (Fig. 3). It should be considered that a very limited number of days were characterized by extreme temperatures (i.e., below −5 °C and over 35 °C). This could be a limiting factor for the interpretation of data recorded at those temperature ranges.
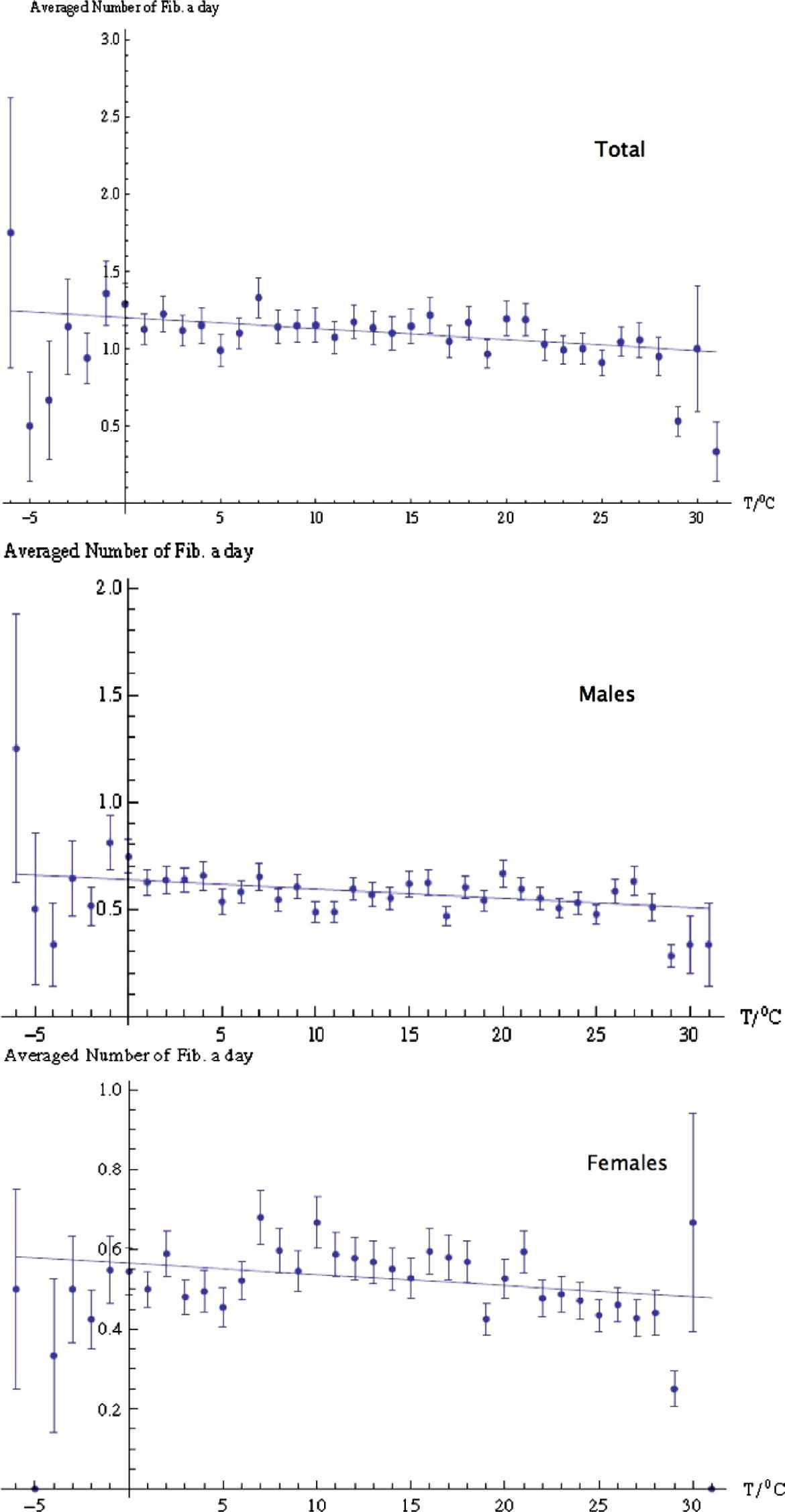
Correlations between episodes of AAF and mean daily temperature, represented separately for the whole sample, for males only and for females only.
| Temperature | Humidity | |
|---|---|---|
| Total | R = −0.60; p = 0.001 | R = −0.07; p = 0.2 |
| Males | R = −0.58; p = 0.007 | R = −0.22; p = 0.99 |
| Females | R = −0.36; p = 0.06 | R = 0.14; p = 0.08 |
Correlations between number of visits for AAF, mean temperature and mean humidity, represented separately for the whole sample, for males only and for females only.
For a typical day, with a temperature close to 13.5 °C (i.e., the mean T recorded in this region), the average number of visits for AAF was 1.094. The variation of mean temperature influenced the number of visits for AAF, i.e., for winter days with a temperature close to 0 °C, the averaged number of AFs per day was 1.2, while on a hot summer day with temperatures close to 30 °C, the averaged number of AAFs a day was 0.98, with a relative decrease of 17.5%. The multiple linear regression between the mean temperature of the day before the AAF episode and the second up to the 30th day preceding the AAF episode (i.e., correlation of each single AAF episode with the mean temperature of the period of d-days before the event, where d = 0 [corresponding to the same day of the visit], 1 [the day before the visit], 2,…, until 30 [30 days before the visit]) is shown in Fig. 4, in which each point (with the relative one sigma error bars) is produced by the linear regression between the number of cases of AAF and the relative d-day averaged temperature (Td). In order to test this relationship for each value of d (ranging from 0 to 30), the relative average temperature Td (obtained performing the average over all temperatures in the d-days before the event) was further computed for each AAF episode. As such, the cases of AAF were correlated with the past averaged temperature to obtain information over the time scale of the AAF episode. The overall decrease in the incidence of cases of AAF was 21.5% when the difference of temperature is maintained for 14 days.
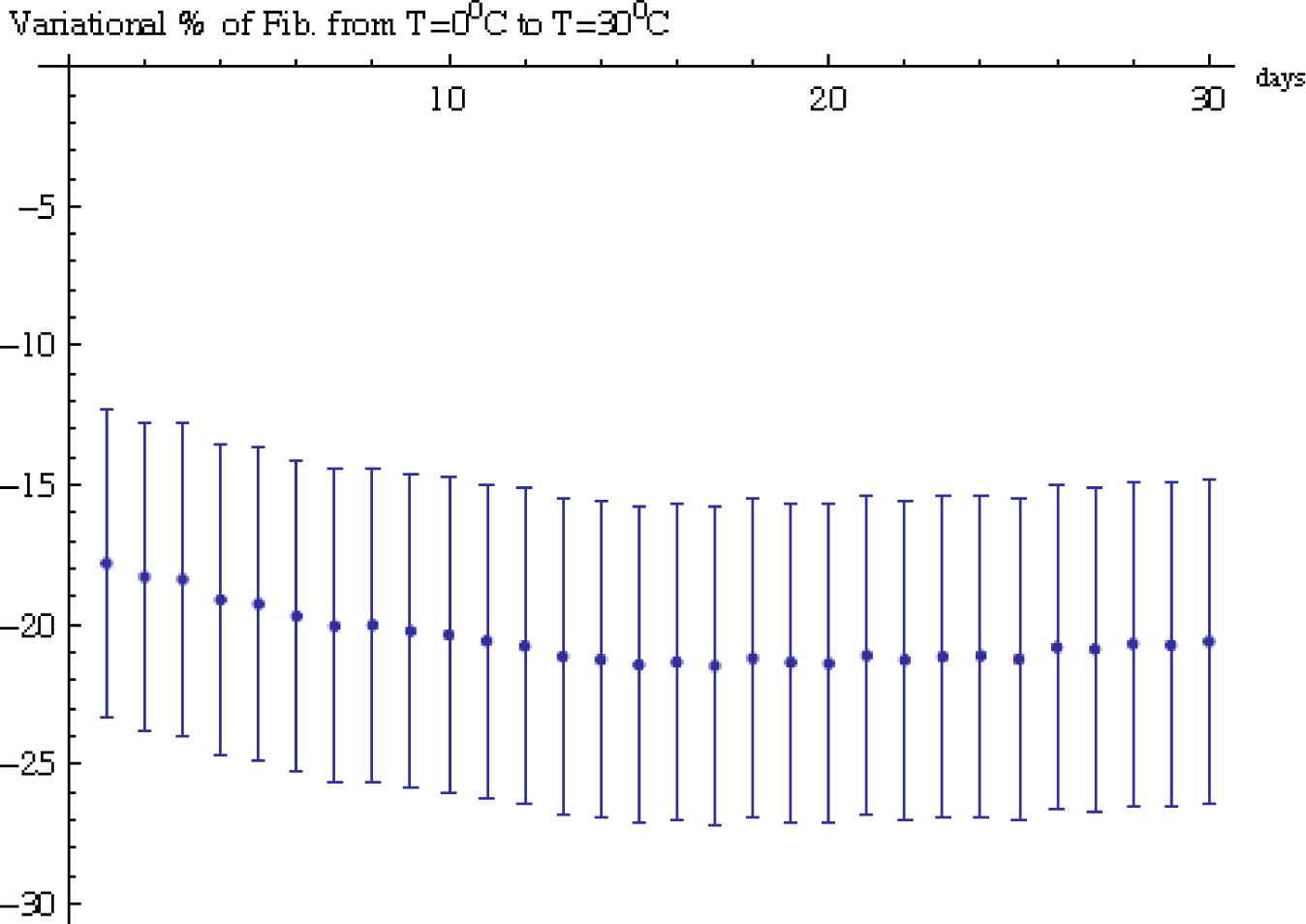
Correlation between the % decrease in cases of AAF and the mean temperature of d-days before the visit, with d going from 0 (correlation with the mean temperature of the same day of the admission) to 30 (correlation with the mean temperature of 1 month before the admission). Black circle points are the % decrease (with relative one sigma error bars) in cases of AAF when the temperature is going from 0 to 30 °C.
No correlation was found between the number of AAFs and the daily humidity in the whole study population (R = −0.07; p = 0.2), as well as in males (R = −0.22; p = 0.99) and females (R = 0.14; p = 0.08). With multiple linear regression analysis, the correlation between AAF and humidity (p = 0.33) or temperature (p = 0.0018) was slightly weaker than that observed in univariate analyses.
4. Discussion
This report describes the largest study that has correlated the short-term variation of climate and the number of episodes of AAF so far. Indeed, the large size of this sample was possible due to the fact that an electronic database was used. The onset of AF does not occur in a totally randomized manner. In agreement with the study of Frost et al., it was also found that a higher risk of AF occurred during the winter along with an inverse correlation with outdoor temperatures. These results are also in accord with previous findings of an excess risk of AF during the winter, as earlier reported by Viskin et al. [12], as well as during the autumn as reported by Watanabe et al. [13]. It is well known that the atmospheric factor correlating with the incidence of AAF (i.e., air temperature) is somewhat, even if not linearly, associated with sunshine, day length or atmospheric circulation. In this region, for example, day length and sunshine peak at the end of June, while temperature peaks between the end of July and the first 2 weeks of August. On the other hand, day length and sunshine both reach their nadir at the end of December, while temperature reaches its nadir typically 1 month later. It is noteworthy that this study population was mostly based on patients admitted to the ED for symptomatic episodes of AAF, so that asymptomatic episodes could not be included. This study also showed that the incidence of symptomatic AAF is only slightly related to changes of microclimatic variables, most evidently with temperatures. Therefore, the results of the previous studies cannot fully be confirmed, but some differences must be emphasized. For example, in the study of Viskin et al., 79% of their patients had underlying heart disease, while Watanabe et al. reported that only 39% of their patients were symptomatic for AAF. As such, the main strength of this investigation is the large population of patients included, belonging to a large geographical area that has this Hospital as the sole center with an ED. A limiting factor of the study is represented by the inclusion of some repeated visits for recurrent AAF, i.e., 2.8% of patients and 12.5% of all visits. Moreover, it was not possible to record the co-morbidities, such as structural heart disease, thyrotoxicosis, gastroesophageal reflux disease, sepsis, recent surgery, etc., which are all potential sources of AAF. This is an ecological study, and populations or groups of people, rather than individuals, have been analyzed. There are some limitations of these types of studies, but it is accepted that they can focus on important issues that cannot be addressed by other study designs, such as randomized clinical trials [25].
As regards the potential pathogenetic mechanisms linking AAF and low temperature, it seems conceivable that the seasonal incidence (e.g., including acute-onset as well as the reacutization form of AF, both symptomatic and silent) may be at least partially attributed to diseases with a similar seasonal pattern, for example those co-morbidities that prevail during the winter which may be significant triggers of increased sympathetic activity and cardiac arrhythmias, such as pneumonia, exacerbations of COPD, stroke and myocardial infarction.
In conclusion, it was found that in a tempered, continental, climate, AAF incidence is related to air temperature, but not to air humidity.
Conflict of interest
None declared.
Acknowledgements
We acknowledge Dr. Carlo Caccimani, director of ARPA (regional meteorological service of Emilia-Romagna) for the precious contribution in reviewing meteorological issues of the study.
References
Cite this article
TY - JOUR AU - Ivan Comelli AU - Jayme Ferro AU - Giuseppe Lippi AU - Denis Comelli AU - Elisabetta Sartori AU - Gianfranco Cervellin PY - 2014 DA - 2014/01/08 TI - Incidence of acute-onset atrial fibrillation correlates with air temperature. Results of a nine-year survey JO - Journal of Epidemiology and Global Health SP - 151 EP - 157 VL - 4 IS - 3 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2013.12.003 DO - 10.1016/j.jegh.2013.12.003 ID - Comelli2014 ER -