
Change in the structures, dynamics and disease-related mortality rates of the population of Qatari nationals: 2007–2011
- DOI
- 10.1016/j.jegh.2014.04.002How to use a DOI?
- Keywords
- Qatar; Qatari nationals; Disease-related mortality; Public health
- Abstract
Background: Developing effective public health policies and strategies for interventions necessitates an assessment of the structure, dynamics, disease rates and causes of death in a population. Lately, Qatar has undertaken development resurgence in health and economy that resulted in improving the standard of health services and health status of the entire Qatari population (i.e., Qatari nationals and non-Qatari residents). No study has attempted to evaluate the population structure/dynamics and recent changes in disease-related mortality rates among Qatari nationals.
Objective: The present study examines the population structure/dynamics and the related changes in the cause-specific mortality rates and disease prevalence in the Qatari nationals.
Methods: This is a retrospective, analytic descriptive analysis covering a period of 5 years (2007–2011) and utilizes a range of data sources from the State of Qatar including the population structure, disease-related mortality rates, and the prevalence of a range of chronic and infectious diseases. Factors reflecting population dynamics such as crude death (CDR), crude birth (CBR), total fertility (TFR) and infant mortality (IMR) rates were also calculated.
Results: The Qatari nationals is an expansive population with an annual growth rate of ∼4% and a stable male:female ratio. The CDR declined by 15% within the study period, whereas the CBR was almost stable. The total disease-specific death rate, however, was decreased among the Qatari nationals by 23% due to the decline in mortality rates attributed to diseases of the blood and immune system (43%), nervous system (44%) and cardiovascular system (41%). There was a high prevalence of a range of chronic diseases, whereas very low frequencies of the infectious diseases within the study population.
Conclusion: Public health strategies, approaches and programs developed to reduce disease burden and the related death, should be tailored to target the population of Qatari nationals which exhibits characteristics that vary from the entire Qatari population.
- Copyright
- © 2014 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
A clear understanding of population structure, dynamics, disease frequency and causes of death is critical for developing and implementing effective public health policies and strategies for interventions [1]. However, a few countries in the world have estimates of cause-specific mortality rates that can be reliable to develop evidence-based public health actions [2]. This shortage in health-related information is primarily common in the developing world [3] where the disease burden is related to both communicable and non-communicable diseases and injuries. This is in contrast to the notable changes in demographic and epidemiological factors and risk patterns across the world over the past few decades that led to the transition from infectious to chronic non-communicable disease in the developed world. The developing countries also experience a shortage of medical personnel to record details of deaths together with poor quality information on the causes of deaths [4].
The State of Qatar has undergone major social and economic changes resulting in rapid urbanization and a shift into a more sedentary lifestyle and unhealthy dietary practices with a consequent increase in the burden of non-communicable diseases and injuries over the infectious disorders [5–7]. In agreement, a recent study has shown that ischemic heart disease and road traffic accidents are the two leading causes of burden of diseases in Qatar in 2010 [8]. The study utilized the mortality data for the year 2010 according to the International Statistical Classification of Diseases and related health problems, tenth revision (ICD-10) coding system. The study did not assess the cause-specific morality rates, but rather the disability adjusted life years (DALYs), total years of life with disability (YLD), years of life lost and percent of total DALYs, and did not distinguish between the disease burden within the homogenous Qatari nationals and the heterogeneous dynamic non-Qatari population. It is known that the vast majority of the population in Qatar is composed of expatriates that – although increasing – continually change [9]. The populations of the Qatari nationals and non-Qataris exhibit diverse socioeconomic and cultural differences that ought to reflect in discrepancy in their disease prevalence rates. No study has examined the changes in the cause-specific mortality rates and disease burden among the Qatari nationals, particularly over the past few years. This is despite the fact that the State of Qatar prospectively monitors numerous demographic events within the entire population and can thus provide accurate cause-specific mortality rates that should assist in developing effective public health policies and actions specifically suitable for the Qatari nationals.
The United Nations Millennium Development Goals (MDGs) are eight goals that all the 191 UN Member States have agreed in the year 2000 to try to achieve by the year 2015. Reducing child mortality, improving maternal health and combating a range of diseases were among these goals [10]. The midpoint assessment of MDG achievement, published in 2007 [11] has shown that the countries from the Western Asia, including Qatar, are on track to accomplish the MDGs [11]. Additional effort to further improve the health status in Qatar and reduce the burden of diseases remains and requires to be designed to meet the local needs and conditions. The present study was undertaken, therefore, in an attempt to examine the structure and dynamics of the population of Qatari nationals over the past few years (2007–2011), i.e., since the MDG midpoint assessment, and to evaluate the related changes in the cause-specific mortality rates and disease burden. This effort may contribute to generating evidence-based priorities for health interventions particularly tailored to the Qatari nationals.
2. Methods
2.1. Study population and source of data
The present study evaluates the changes in the disease-related mortality rates only in the population of Qatari nationals. This is a homogenous, gender-balanced (M:F ratio of ∼1:1, Fig. 1) and steadily growing population that is in contrast to the non-Qatari nationals. The latter is a heterogeneous, dynamic population that is predominantly males (M:F ratio of ∼3:1; Fig. 1) and exhibits an economic-dependent growth pattern. A retrospective, analytic descriptive analysis was conducted covering a period of 5 years (2007–2011) and utilized a range of secondary data sources available in the public domain as well as data from the Supreme Council of Health (SCH) published Annual Health Reports (2007–2010) [9] and data from the Health Information Intelligence Unit, Department of Public Health, SCH [for the year 2011]. Permission to use these data was obtained from the Qatar Statistics Authority. Data collected for the present study included demographic surveillance, records of births, deaths, Qatari population estimates, age- and gender-stratified population records, and proportionate mortality and disease-related mortality rates according to the ICD-10 WHO classification system. A garbage code was assigned in the original mortality data prior to the analysis. However, the garbage code was not utilized in the data analyzed here.
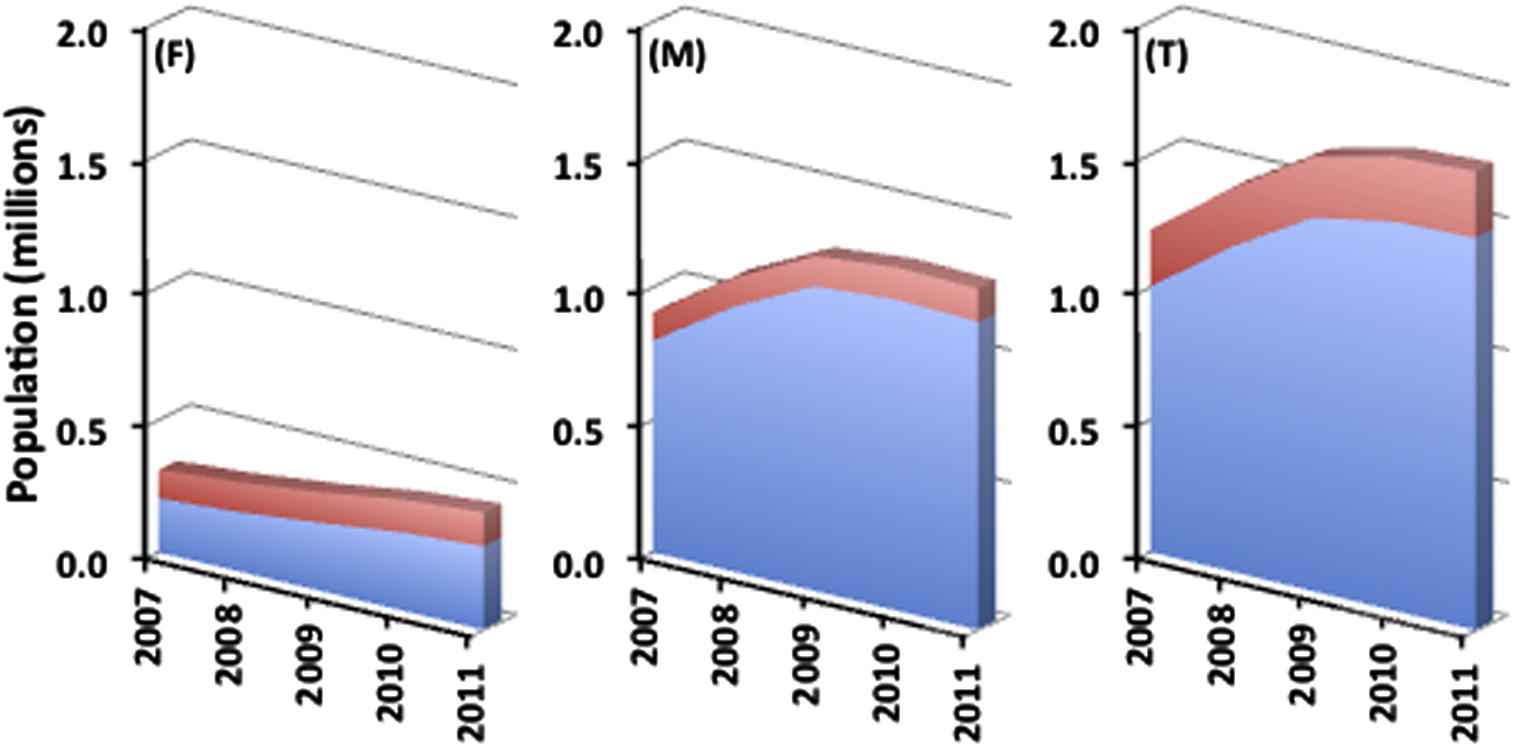
Change in the Qatari national population structure between 2007 and 2011. Figures represent the changes in the populations of Qatari nationals (red) and non-Qatari (blue) in females (F), males (M), and the total population (T).
Data related to the prevalence of chronic diseases in Qatar were obtained from the WHO Qatar STEPS Survey 2012 [12]. The STEPS survey of chronic disease risk factors in Qatar is a population-based survey of adult Qatari nationals (n = 2,496, 18–64 years old, and response rate 88%). This survey was conducted between March and May 2012 and has a multistage cluster sampling design. Socio-demographic and behavioral information was collected first (Step 1), followed by some anthropometric and blood pressure measures (Step 2). The biochemical measures, e.g., fasting plasma glucose (FPG) and total cholesterol were collected at the last stage (Step 3). The female to male ratio among the responders was 1.37 (57.8% females and 42.2% males). For both sexes, the age distribution of the participants was predominantly between 18 and 44 years (69.3%) that is 2.26-fold higher in proportion than the 45–64 age group (30.7%). The weights in the STEPS survey post stratify the examined samples directly to the Qatari population based on the 2010 census data for Qatari nationals although only a portion of the 2496 participants have had blood biochemical measures. This may have led to an overestimation of some chronic conditions. The 2006 World Health Survey (WHS) that included a representative sample of a total of 29,338 people [13] (both Qatari nationals and non-nationals) from 4800 households in Qatar was also utilized. The change in the chronic disease and risk factor prevalence rates in Qatari nationals was compared between the 2006 (WHS) and 2012 (STEPS) surveys.
2.2. Data analysis
Depicting the age and sex distribution of the Qatari national population was carried out graphically by generating a population pyramid for each of the studied years [14]. Factors related to the population dynamics, such as crude death (CDR), crude birth (CBR), total fertility (TFR) and infant mortality (IMR) rates, were all calculated as previously described [15]. The CDR is defined as the total number of deaths in Qatari nationals divided by the total population at the mid-point of a calendar year and expressed per 1000 subjects. The CBR, however, was defined as the number of live births during one calendar year divided by the total population at the mid-point of the same year and expressed per 1000 Qataris. Although CBR can reflect the fertility in a population, a more standardized way that accounts for the percentage of women of reproductive age is the TFR; it is the average number of children that would be delivered by Qatari females if all women lived to the end of their childbearing years (i.e., 15–44 years old). The IMR was calculated by dividing the number of infant deaths during one calendar year by the number of live births during the same time period and expressed per 1000 Qataris. To assess the changes in the disease-specific mortality rates over the five-year study period, trends were calculated using linear regression analysis. In their analysis of causes of death, to determine the global burden of disease in 2010, Murray et al. [16] used the Cause of Death Ensemble model strategy to develop ensembles of the best performing models that met two plausibility criteria. The first is that the direction of the regression coefficient for a covariate is in the expected direction. The second, however, is that the coefficient has a p value of less than 0.05. In our analysis, only the second criterion of Murray et al. [16] was employed. The linear regression approach was utilized taking into consideration the change of the mortality rates within the study period. Data for chronic disease prevalence were obtained from the Fact Sheets of the WHO Qatar STEPS Survey 2012 [12] whereas the rates of infectious diseases were calculated from the Vital Health Statistics Annual Reports of the SCH [9] and the information obtained on the Qatari national population estimates.
3. Results
The changes in the population of the Qatari nationals within the study period (2007–2011), shown in Fig. 1, reveal a 17.3% increase in the total population. This increase was almost equal in both males and females. The annual growth rate of the population was approximately 4% over the study period. The overall M:F ratio was stable at 1.02 during the five-year period. The increase in the total population in Qatar was linked to the overall reduction by 14.6% in the percentage of the Qatari nationals to the total population. The age structure diagram of 2007–2011 (Fig. 2) shows that the population of Qatari nationals has a standard-shaped pyramid characterized by a broad base. This expansive population pyramid represents greater number of people in the younger age categories.
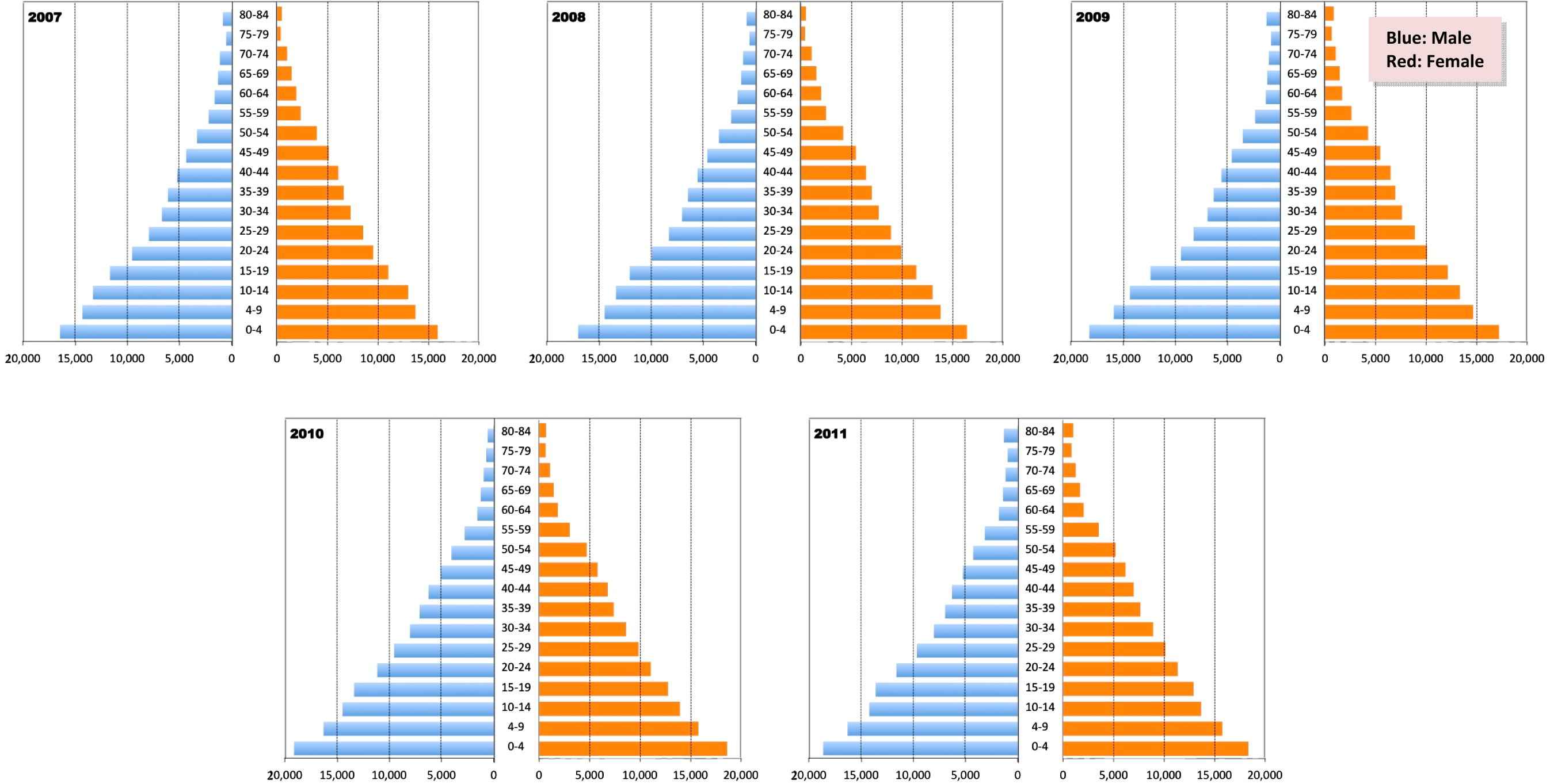
The population pyramids of the Qatari nationals from 2007 to 2011.
Factors presenting the population dynamics, such as CDR, CBR, TFR and IMR, are shown in Fig. 3 for the Qatari nationals. The five-year change in the CBR has shown a slight non-significant 7% decrease from 2007 to 2011 (from 3.2 to 2.7 per 1000 Qataris). This lowering in the CBR was accompanied by ∼30% decline in the TFR from 2.8 to 2.0 per Qatari woman. The IMR showed almost no change within the study period where the 5-year average of 8, 6.7, and 8.3 per 1000 live Qatari births was recorded for <7 days, <1 year and <5 years of age, respectively.
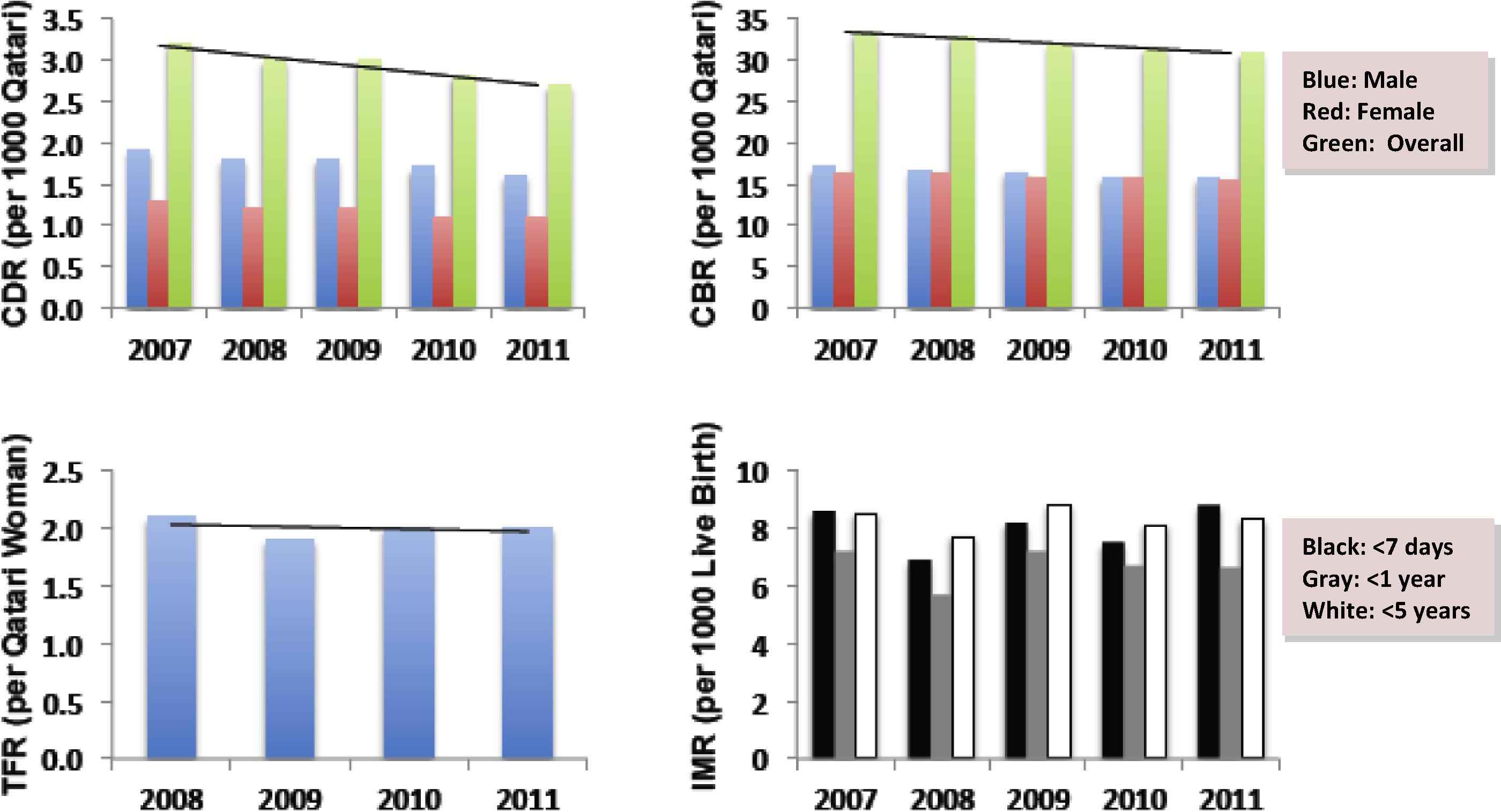
Change in the Qatari national population dynamics between 2007 and 2011. Figures represent CDR, CBR, TFR and IMR. In each of the CDR and CBR, the ratio of males and females was calculated in relation to the total population. In the IMR insert, <7 days also includes perinatal mortality rates from 28 weeks of pregnancy. Dark line represents the trend across the study period. Trends in the CBR and CDR are in relation to the total number of males and females.
The CDR declined by 15% within the study period where it was decreased from 3.2 per 1000 Qataris in 2007 to 2.7 in 2011. The total disease-specific death rate, however, was decreased in the Qatari nationals by 23% as shown in Fig. 4. This overall decline was attributed primarily to a significant reduction in deaths related to blood and immune system diseases (43%), diseases of the nervous system (44%), cardiovascular diseases (41%) and diseases of the skin and subcutaneous tissues (45%), and the external causes of death (e.g., road traffic accidents; 47%). Death rates due to cancer, endocrine, metabolic and nutritional diseases were not changed over the study period.
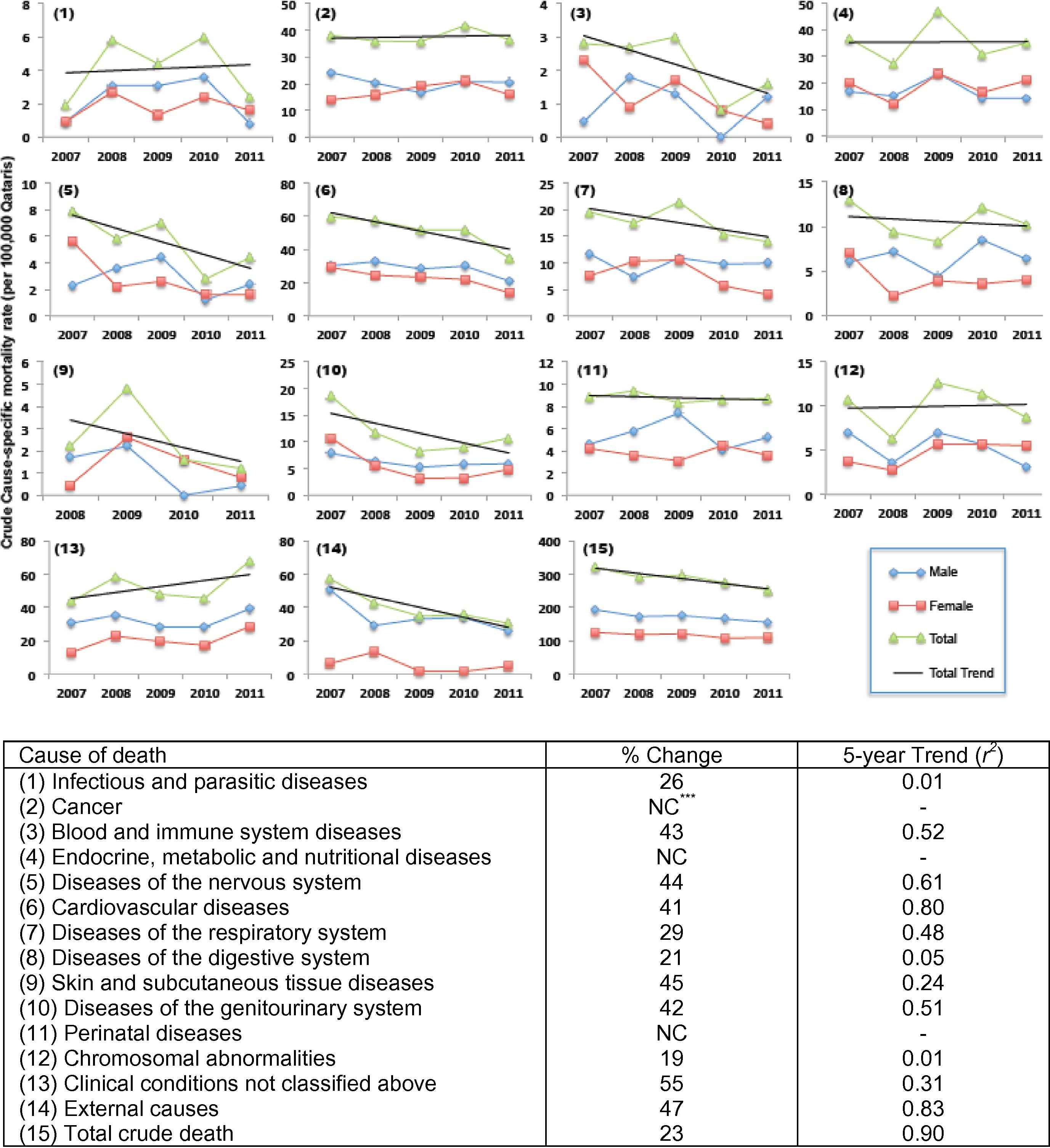
Disease-related mortality rates in the Qatari nationals from 2007–2011. The number in the parenthesis corresponds to the number in the cause of death in the insert below. The change within the study period is presented as % change. The 5-year trend is shown and was calculated using linear regression analysis.
The prevalence rates of selected chronic (Table 1) and infectious (Fig. 5) diseases were also evaluated within the Qatari nationals. The rate of obesity among the studied population reached 41.4% with the rates in females slightly higher than their male counterparts. Prevalence of pre- and type 2 diabetes in the Qatari nationals was 16.7% with females having a slightly higher rate than males. Hypertension, a predisposing condition for cardiovascular diseases was found in about one third of the studied population. These chronic disease prevalence rates were somewhat higher than those predicted from the 2006-WHS study (Table 1). The prevalence of hepatitis A, B and C has shown an overall decline in the Qatari nationals, with hepatitis C rates higher than those of hepatitis B and A combined (Fig. 5). Although the prevalence rates of measles and tuberculosis (TB) infection have not changed over the study period, the total rates of infectious disease prevalence have declined by 27% from 2008 to 2011 (r2 = 0.90, p < 0.05).
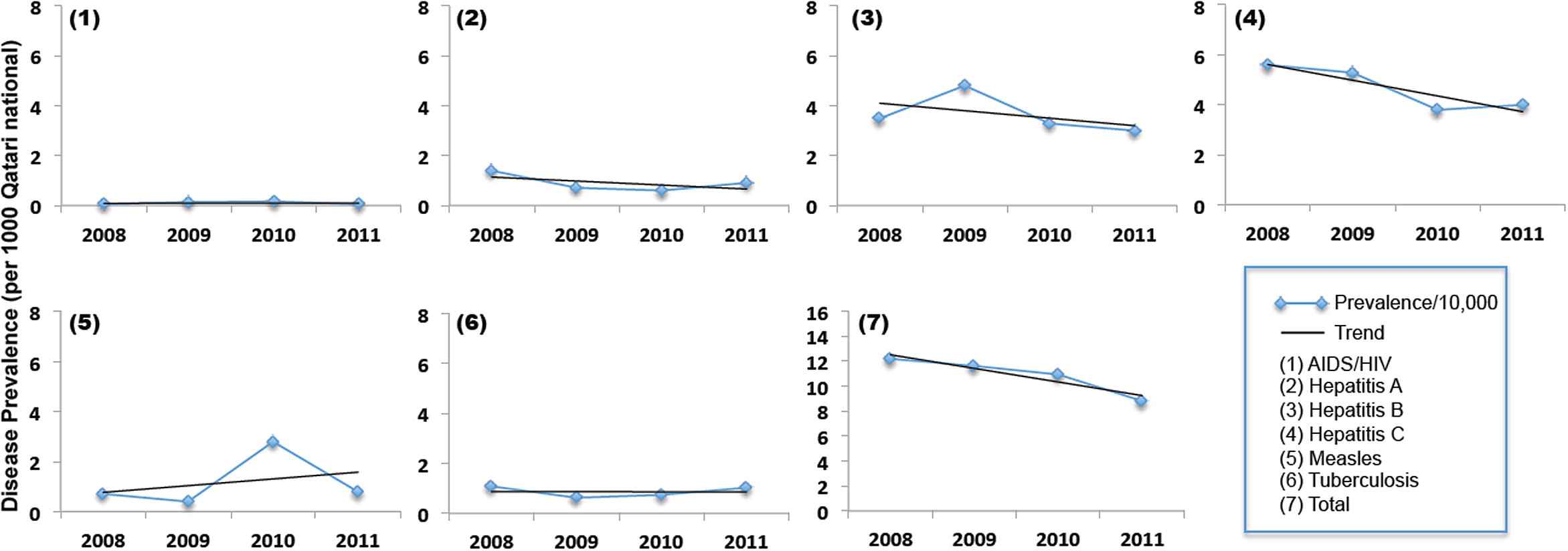
Prevalence rates of a range of communicable diseases in Qatar from 2007 to 2011. The number in the parenthesis corresponds to the number in the cause of death in the insert below. The same scale was retained for all graphs (except the totals) in order to exhibit the relative prevalence of diseases compared with each other. Dark line represents the trend across the study period.
| Disease risk factors | Definition | 2006-WHS overall prevalence (%) | 2012-STEPS prevalence (%) (95% CI) | ||
|---|---|---|---|---|---|
| M | F | Overall | |||
| Obesity | Body mass index (BMI) ⩾30 kg/m2 | 34.2 | 39.5 (35.5–43.6) | 43.2 (35.5–43.6) | 41.4 (38.8–44.0) |
| Pre- and type 2 diabetesa | Fasting plasma glucose (FPG) ⩾6.1 mmol/L or on medication for hyperglycemia | 11.6b | 17.6 (13.1–22.2) | 15.9 (12.4–19.3) | 16.7 (13.7–18.8) |
| Hypertension | Systolic blood pressure (SBP) ⩾140 and/or diastolic BP (DBP) ⩾90 mmHg or on medication for hypertension | 12.9 | 28.0 (24.5–31.5) | 37.7 (33.3–31.5) | 32.9 (30.2–35.9) |
| Smoking | Current tobacco smokers | 10.9 | 31.9 (27.9–35.9) | 1.2 (0.5–1.9) | 16.4 (14.3–18.4) |
| Physical activity | Lack of engagement in vigorous activity | N/Ac | 59.6 (55.4–63.7) | 82.7 (78.3–87.1) | 16.4 (14.3–18.4) |
| Diet | Less than 5 servings of fruit and/or vegetables on average per day | 84.5 | 91.9 (87.8–96.1) | 90.4 (87.8–94.0) | 91.1 (87.7–94.6) |
| Cholesterol | Raised total cholesterol (⩾5.0 mmol/L or ⩾190 mg/dl or currently on medication for raised cholesterol) | 21.4 | 19.1 (14.7–23.4) | 24.6 (20.9–28.4) | 21.9 (18.8–25) |
Pre-diabetic status is considered as impaired fasting glucose (IFG), i.e., FPG >=6.1 mmol/L (110 mg/dL) and < 7 mmol/L (126 mg/dL) in accordance with the WHO 1999 criteria.
Self-reported type 2 diabetes.
Information was not available in the original report.
Incidence rates of selected chronic diseases in the adult population of Qatari nationals from the 2012 STEPS Survey in comparison with the 2006 World Health Survey (WHS) in Qatar.
4. Discussion
Over the past few years, Qatar has undertaken comprehensive development resurgence in areas of economy and construction that surpassed the expected accomplishment rates. Consequently, the individual standard of live has been highly improved together with the health and education services. The rapid transition and development in socioeconomic status and high standard of living have resulted in a substantial improvement in the life expectancy and lifestyle of the people of Qatar. Several studies have assessed the improvement in the burden of diseases, mortality, disability, and disability-adjusted life years (DALYs) within the entire Qatari population, i.e., the homogenous Qatari nationals and the heterogeneous dynamic expatriates [8,9,16,17]. The present study is the first to evaluate the population structure and recent changes in disease-related mortality rates in Qatar in an effort to generate evidence-based intervention strategies that address national health priorities that exist in the population of the Qatari nationals.
The Qatari national population showed a 17% increase from 2007 to 2011 with an approximate equal gender change. This is comparable to the 13% increase noted between the years 2005–2009 among United Arab Emirates nationals [18]. Based on the increase in the population of the Qatari nationals and the crude death and birth rates, it is estimated that the average rate of annual natural increase within the population will be ∼3% (results not shown) – a rate that is also comparable to that observed in the UAE [18]. Although this figure is usually affected by both birth rate and death rate together [19], it can be more influenced by the marked decline in death rates (∼15%) experienced in Qatar within the past 5 years (Fig. 3). Indeed, over the past decade in Qatar there has been a significant effort to introduce effective public health measures such as better nutrition, greater access to medical care, improved sanitation, and more widespread immunization. This effort has culminated into a rapid decline in death rates and in child mortality rates (Fig. 3). The increase in the Qatari national population size over the past 5 years (∼17%) has been accompanied by a great increase in the size of the expatriate population (42%). Such a discrepancy resulted in an under-representation in the Qatari nationals within the total population in Qatar from 17.1% in 2007 to 14.6% in 2011 (i.e., ∼15% decline). The change in the proportion of the Qatari nationals to the total population is primarily due to the increased inward migration to Qatar as a result of the rapid economic growth being experienced in the country over the past few years. Although, to a lesser extent, this change is similar to what has been reported in the UAE where the proportion of the nationals to the total population was decreased from 20% in 2005 to 11.4% in 2009 (i.e., ∼40% decline) [18].
The expansive symmetrical population pyramids shown for the Qatari nationals (Fig. 2) implicate that there is larger number of the population in the younger age groups, with each age group greater in size or proportion than the one born before it and with an almost equal male to female ratio at the different age groups [14,15]. This indicates that the growth of the studied population is rapid. The shape of the population pyramids for the Qatari nationals contracts sharply with that of the entire Qatari population (i.e., nationals and expatriates). The latter exhibits a constrictive asymmetrical population pyramid and a negative growth and displays a lower number of younger people [8]. The population pyramid of Qatar is also characterized by a demographic anomaly and a bump showing more males (20–40 years old) than females [20]. This bump, however, does not travel onward because the larger number of working age men in the Qatari pyramid implies a migrant workforce.
The CDR is known to be influenced by the age structure and can accurately indicate the effect of mortality on the population growth [21]. According to the United Nations, Department of Economic and Social Affairs, Population Division, the CDR in the entire Qatari population between 2005 and 2010 was 1.6 [22], a figure that is about 2-fold lower than the CDR in the Qatari nationals that range from 3.2 (in 2007) to 2.7 (in 2011) with a 5-year average of 2.94 (Fig. 3). The worldwide CDR is 8.4 between 2005 and 2010 [22,23], which is markedly higher than that in Qatar. Similarly, the CBR in the Qatari nationals varies from 33.4 (in 2007) to 31.0 (in 2011) with a 5-year average of 32.2, a figure that is about 2-fold higher than that of the entire Qatari population (14.1 between 2005 and 2010) and 1.6-fold higher than the world rate of 20.0 [22,23]. This apparent discrepancy between the Qatari nationals and the entire Qatari population is principally due to the large number of migrant workforce members. Expatriates represent the vast majority of the entire Qatari population – mostly single male laborers. This sub-population is significantly lowering both the CDR and the CBR on the level of the entire population residing in Qatar.
The TFR is known to be a more direct measure of the level of fertility than the CBR, since it refers to births per woman. This indicator shows the potential for population change in a country [21]. In the Qatari nationals, the TFR varied from 2.8 to 2.0 children per woman between 2007 and 2011 (Fig. 3). A rate of two children per woman is considered to be the replacement rate for a population, resulting in a relative stability in the total population [21]. This is in agreement with the outcome predicted from the population pyramid as discussed above. The TFR in the entire Qatari population is estimated as 2.3 children per woman between 2005 and 2015 [22], which is comparable to the world rate of 2.5 within the same period [23]. It should be noted that the contribution of the expatriates in modifying the TFR in Qatar is minimal since the largest proportion of the non-Qataris is single male workers who do not influence the fertility rates in the country. Since the TFR can be used as an estimate of the fertility growth factor in a population, e.g., whether the childbearing population is replacing itself or not, the rate in the Qatari nationals in 2011 indicates that couples are producing at least two children to replace themselves if all other factors affecting the population remain constant, such as death rates and migration.
As a standard indicator of population health, the IMR was examined in the Qatari nationals. The average national IMR between 2005 and 2010 was about 8 per 1000 live births [23,24]. This figure is markedly lower than the world rate of 42 within the same time period [23]. Similar to the TFR, the influence of the migrant workforce is minimal in modulating the IMR since the Qatari nationals had an IMR (in <5 years old children) that is slightly higher than 8 per 1000 live births (Fig. 3). The lower CDR and relatively stable TFR and IMR reflect an enhanced health status of women and infants within the Qatari national population as well as their access to medical care, socioeconomic conditions and the recent effectiveness of the public health practices in Qatar. As infant mortality is often used as an indicator of overall development of a nation, it may be relevant to mention that Qatar now is among the lowest 50 nations in terms of rates of infant death, a figure that reflects the major social, economic and health care advances the country is currently experiencing [25].
Data of the present study showed that there is a slight decline in the total disease-related deaths over the past five years (Fig. 4) that is attributed primarily to the reduction in what is usually regarded as the major causes of death [26]. In the Qatari nationals, apart from the external causes of death (e.g., road-traffic accidents) and unidentified clinical conditions, diseases of the circulatory system, cancer, and metabolic disorders are in order the three chief causes of death. Over the study period (2007–2011), the rates of death related to diseases of the blood and immune system, nervous system, cardiovascular system, and the skin, subcutaneous tissue and genitourinary system were declined by ∼40% in 2011 compared with the rates of 2007 (Fig. 4). External causes of death have declined by ∼50% within this period. These findings concur with those reported recently by Bener et al. [8] showing that non-communicable diseases and road traffic accidents were a significant cause of health burden in Qatar. Specifically, this study revealed that the burden of disease in Qatar originates primarily from ischemic heart disease, road traffic accidents and birth asphyxia and trauma, as these diseases were the major causes of lost years of healthy life as measured by DALYs. The decline in the rates of death related to these conditions reflects the substantial investments in health care infrastructure in Qatar over the past decade, building hospitals and clinics and promoting a more modern approach in tackling the infectious diseases and developing and implementing programs for chronic disease treatment and prevention [25].
Death related to cardiovascular diseases (Fig. 4) can be associated with the increased disease prevalence reported recently in Qatar [8] that was proposed as a consequence to the high prevalence of obesity and type 2 diabetes mellitus together with the limited physical activity and the excessive consumption of saturated fats [27] as well as the aging of the population of Qatari nationals. Indeed, a recent study was developed in Qatar in collaboration with the WHO [12] to provide a better understanding as to the prevalence of a range of chronic diseases and their risk conditions in the Qatari nationals in order to deliver the knowledge needed to make informed choices about health in Qatar (the STEPS Survey). As indicated in Table 1, obesity was prevalent in about 40% of the Qatari nationals, whereas pre- and type 2 diabetes frequency reached >16%. Approximately one-third of the studied population suffers from hypertension, a predisposing condition for cardiovascular diseases. These rates are somewhat higher than those reported in 2006 from the WHS (Table 1).
Several studies have reported that Qatar has one of the highest prevalence rates of obesity among all the Gulf Cooperation Council (GCC) countries and sixth globally [28]. It has the highest rate of obesity among boys in the Middle East and North African region [6,29]. Furthermore, high prevalence rates of hypertension (32%), metabolic syndrome (27%), hyperglycemia (13%), diabetes, and cardiovascular diseases (∼240 cases/100,000 for both conditions) were reported recently from Qatar [5–8,29–32]. Additionally, recent reports stated that non-communicable diseases account for 63% of all classified deaths in the Qatari general population [20]. Recently, Badawi et al. reported a high frequency of micronutrient deficiency (vitamin D) in Qatar (>90%) that may exasperate the elevated frequencies of chronic conditions in the population [27].
Cardiovascular diseases, diabetes, cancer and respiratory conditions account for ∼50% of all disease-related mortalities. Qataris have a higher rate of death due to chronic diseases than non-Qataris (62% vs. 49%) primarily due to the different characteristics of two populations and the aging of the Qataris whereas non-Qataris tend to be younger and healthier [20]. In general, the CDR of the total population of Qatar in 2011 was 1.12 per 100,000 with Qataris having a rate of 2.67 compared with 0.85 for non-Qataris. The large proportion of the disease-related mortalities (the present study) and the extent of the disease burden [8] ascribed to non-communicable conditions in Qatar confirm the growing importance of these conditions into the Qatari population health. It also highlights the critical need to implement a range of population-based prevention strategies in addition to tailoring health planning and priority setting in the health sector to combat chronic diseases.
Efforts to reduce the burden of non-communicable diseases in Qatar have to be accompanied by and in conjunction with similar efforts to combat the communicable diseases. Some of the communicable diseases targeted globally include HIV/AIDS, measles, TB and hepatitis [10,11]. Apparently, hepatitis C and B have the highest prevalence rates among the other targeted communicable diseases within the Qatari nationals (Fig. 5). Despite the fluctuating prevalence rates of measles and TB, the overall rates of infectious disease prevalence have declined by about one-third from 2008 to 2011, perhaps due to the decreased prevalence of hepatitis C during the study period. The rates of hepatitis C and A observed among the Qatari nationals represent 10% of what has been reported on the national level (i.e., for the entire Qatari population), whereas hepatitis B rates were comparable between the two populations. Measles rates among the Qatari nationals were twofold lower than the rates observed in the entire Qatari population. The discrepancy in the rates in communicable diseases between the entire Qatari population and the Qatari nationals can be attributed to the size of the latter compared to that of the expatriates (Fig. 1). Furthermore, there is a significant inflow of predominantly young male laborer migrants from South Asia (e.g., India, Pakistan, Bangladesh and Nepal), Southeast Asia (e.g., Philippines and Indonesia) and the Middle East and North Africa [20]. A number of these laborers may have encountered some of the infections in their country of origin prior to residency that adds to the overall national levels of disease frequency. Furthermore, this influx of young male laborers significantly alters the age structure of the population where more Qatari nationals are in the older age groups and, subsequently, have a lower immune system.
Based on the morbidity and mortality data related to infectious diseases in Qatar, including HIV/AIDS, these conditions do not seem to be a major health burden in the country. Indeed, a significant effort, through immunization and screening of immigrants, is undertaken, leading to achieving and sustaining this low prevalence of infectious diseases. In Qatar all expatriate workers are screened for selected communicable diseases prior to entry, an approach that has maintained TB and HIV/AIDS at a very low frequency in the country in spite of the increasing flow of workers over the past decade [20].
This study addresses the need for a better health information system in Qatar to improve mortality data, hospital discharges, outpatients’ data, pharmacy records, and lab reporting. It is also essential to generate follow-up studies in order to assess the risk factors and related associations with morbidity and mortality among the Qatari population. Qatar has the adequate resources and means to integrate all of its health data to maximize their utility for planning and evaluation. Such an approach will ultimately lead to developing more effective programs for disease prevention and mitigation in the country which will consequently reduce the burden of disease-related mortality. Furthermore, public health strategies, approaches and programs, developed to reduce disease burden and the related deaths, should be tailored to target the population of Qatari nationals since this population exhibits characteristics that vary from the entire Qatari population. Additionally, as the Qatari population ages, there will be more demand on medical and healthcare, an issue that has to be considered in future healthcare strategies in Qatar.
Author’s contribution
A.B. conceived the study idea, performed the data analysis and wrote the manuscript. S.A.K carried out data extraction. E.S., A.-A.A.-T., M.H.A.-T. and S.S. provided input into the study and evaluated its significance to Qatar. All authors critically reviewed the manuscript and approved the final draft.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
Work in this study was supported by the Supreme Council of Health, Qatar (E.S., A.-A.A.-T., S.S. and S.A.K., M.H.A.-T.). The authors would like to thank S. Al-Kuwari and M.S. Al-Boainain, Qatar Statistics Authority for their suggestions and input into the study.
References
Cite this article
TY - JOUR AU - Mohamed H. Al-Thani AU - Eman Sadoun AU - Al-Anoud Al-Thani AU - Shamseldin A. Khalifa AU - Suzan Sayegh AU - Alaa Badawi PY - 2014 DA - 2014/06/02 TI - Change in the structures, dynamics and disease-related mortality rates of the population of Qatari nationals: 2007–2011 JO - Journal of Epidemiology and Global Health SP - 277 EP - 287 VL - 4 IS - 4 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2014.04.002 DO - 10.1016/j.jegh.2014.04.002 ID - Al-Thani2014 ER -