
Evaluation of home respiratory therapy delivered to patients in the Ministry of Health’s Home Medical Program (HMP) and administered through the Madinah HMP Center, Kingdom of Saudi Arabia, 2013
- DOI
- 10.1016/j.jegh.2015.07.006How to use a DOI?
- Keywords
- Effectiveness; Evaluation; Home healthcare; Respiratory therapy; Saudi Arabia
- Abstract
This was an evaluation of home respiratory therapy (HRT) services administered through the Madinah Home Medical Program (MHMP) Center of the Ministry of Health (MoH), Kingdom of Saudi Arabia (KSA). Using a retrospective design and descriptive analyses, we analyzed 83 patient records for the clinical care received, outcomes, and patient satisfaction. We also assessed a subset from an economic perspective. Demographically, 72% were >60 years of age, 80% were female, and 90% were Saudi. Asthma accounted for 34% of the diagnosed respiratory diseases, followed by chronic obstructive pulmonary disease (11%). Most patients (71%) required two or three respiratory modalities: 94% used oxygen therapy and 14% were on mechanical ventilation. A full 90% of HMP patients expressed a high level of satisfaction with the HMP overall care, and 43% saw an improvement in their condition. The MHMP lowered healthcare costs for HRT-receiving patients by decreasing the frequency of emergency room (ER) and outpatient visits by 50.8% from 59 to 30 visits. HRT administered through the MHMP Center improved clinical outcomes and increased patient satisfaction while reducing hospital utilization and associated costs. A prospective study is recommended to assess HMP services in comparison with hospitalization.
- Copyright
- © 2015 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/)
1. Introduction
The Ministry of Health (MoH) of the Kingdom of Saudi Arabia (KSA) has made several attempts to address the increasing costs and the problem of high bed occupancy [1] while providing better quality services and more effective utilization of resources. These programs include the 1-day operation program, more participation from the private sector in funding healthcare services, and the establishment of home healthcare (HHC) facilities.
One of the most cost-effective ways to lower the hospital occupancy rate is by providing HHC services, which is like having a hospital at home [2,3]. HHC is a comprehensive, regulated program operated by a multidisciplinary team of healthcare professionals in the patient’s home [4,5].
The various benefits of incorporating HHC in the health system are known worldwide [6]. The services provided through HHC programs are different from country to country, but most programs are community-based, staffed mainly by professional nurses, and regulated by standard guidelines, which reflect the standard of care for all home health agency interactions [4].
In March 2009, the MoH launched a General Administration of Home Medical Program (HMP) which would operate all over the KSA. KSA’s HMP is government run, and healthcare services are provided by a multidisciplinary team of professionals working in a patient’s home [7].
Currently, the MoH operates the HMP in each region of the Kingdom; the Madinah HMP (MHMP) Center, which is the focus of this study, was the kingdom’s original HHC center and remains unique, handling the majority of home health patients in that city [8].
There is evidence that HHC services relieve bed over-occupancy and offer a reasonable alternative to hospital stays [2], but 6 years after the establishment of the HMP Center in the KSA, it remains unclear if the program is achieving its aims of reducing hospital admissions, lowering bed occupancy rates, and promoting patient-centered treatment by maintaining the same or better level of care with more satisfaction and better health outcomes than traditional hospital-based care.
Internationally, respiratory therapy is considered one of the most important HHC services, thought to be more cost-effective than hospital care [3,9]. Despite the importance of this subject and the need to study it, there are no previous studies that estimate the costs of respiratory therapy or any other HMP service in the KSA.
To assess the achievement of the HMP’s goals for patients needing respiratory therapy through the MHMP Center, we have to evaluate the performance and impact measures for home respiratory therapy (HRT) in the center. In this study, we will use impact evaluation to assess the outcome measures. As part of the evaluation, we will perform an economic evaluation as a pilot study in a subset of HRT patients.
2. Methods
Using a retrospective design and descriptive analyses, we evaluated HRT delivered through the MHMP Center. First, this study describes the characteristics of patients who were receiving HRT through the HMP Center, and second, it describes the clinical care they received through the HMP and the outcomes. Finally, we present a cost assessment of a subset of 30 patients for the economic evaluation.
2.1. Study area
The study was conducted in Al Madinah Al Munawarah, which is situated in the Hejaz region in western KSA, with a population of 1,180,770 (2010 estimate) [10]. Madinah is home to the kingdom’s first HMP Center. It remains unique among HMP centers, serving as KSA’s main training center and a model for the home care program in the KSA: whatever is implemented at this center is disseminated throughout the KSA.
2.2. Study population and sample size
In our study, we included any patients with respiratory diseases according to the 10th International Classification of Diseases or needing any respiratory therapy enrolled through the HMP Center in Madinah, KSA, in July 2013. At this time, there were a total of 574 patients actively enrolled in the HMP Center.
A total of 83 patients with respiratory diseases or needing respiratory therapy were enrolled in the MHMP Center and included in the study.
This study has two parts. The first part assesses 83 patients with regard to their characteristics, the clinical care they received through the HMP Center, and the outcome measures. The second part examines 30 randomly selected patients with complete medical records, those having more information about hospital admission before enrollment to HMP, as a pilot study for a cost evaluation of HRT and medical services utilized prior to and subsequent to enrollment in the HMP program, making use of the available pre-enrollment clinical and medical data.
2.3. Study tool
The researcher created and used a database to collect information and the desired data from the groups’ medical records, consisting of the variables below.
2.3.1. Dependent variables
- •
Outcome measures (Table A1-1. in Appendix 1): Outcomes assessed in the study were patients’/care givers’ overall satisfaction toward HMP services: determined from an annual survey that has been conducted since 2008 using the validated instrument Home Care Client Satisfaction Instrument-Revised [11–13].
- •
Hospital utilization: the total of each of the three categories – emergency room (ER) visits, outpatient department (OPD) visits, and readmission after enrollment to HMP – ranging between 0 visits and the maximum number the individual needed.
- •
Clinical progress while enrolled in the HMP (Table A1-1. in Appendix 1): includes the final clinical outcome after enrollment until the time of the study according to clinical judgment; the Glasgow Coma Scale (GCS) is the only objective clinical measure available in the patients’ records. The GCS is useful for the management of patients and helps medical personnel decide what care patients might need; for example, whether medical staff should interact with the patients directly or whether interaction with their caregivers is sufficient. In addition, GCS scores are used to track improvement or deterioration in a patient’s condition, which is also necessary in an HHC setting.
2.3.2. Independent variables
- •
Patient demographic data: age, gender, marital status, and nationality (Table A1-1. in Appendix 1).
- •
Clinical diagnosis: based on the 10th international classification of diseases (Table A1-1. in Appendix 1).
- •
Clinical care utilized through HMP: types of care, services utilized, and respiratory modalities used (Table A1-1. in Appendix 1).
2.4. Data entry and analysis
Collected data were analyzed using SPSS version 20 (SPSS Inc., Chicago, IL, USA) and SAS 9.3 (SAS Institute, Cary, NC, USA). Percentages, mean, and standard deviation (SD) were used as descriptive statistics. Categorical variables were presented as frequency and percentage. The result is considered statistically significant when p < 0.05. Associations between the demographic variables, clinical diagnosis, HMP medical care, and outcome measures were operated statistically using the Chi-square test for categorical variables or the two sample t test for continuous variables. For the 30 patients, we used the paired t test before and after variables (ER visits, OPD visits, and GCS).
3. Results
3.1. Patient characteristics
3.1.1. Demographic data
Out of 83 patients studied, about three-quarters (72%) were >60 years old. Most of them were female (80%) and of Saudi nationality (90%), and over half (56%) were not married (single, divorced, or widowed) (Table 1).
| Characteristics | n (%) |
|---|---|
| Age | |
| 18–60 y of age | 18 (22) |
| 61–80 y of age | 37 (45) |
| >80 y of age | 27 (32) |
| Missing | 1 (1) |
| Sex | |
| Female | 66 (80) |
| Male | 17 (20) |
| Nationality | |
| Saudi | 74 (90) |
| Non-Saudi | 8 (9) |
| Missing | 1 (1) |
| Marital status | |
| Nonmarried | 46 (56) |
| Married | 26 (31) |
| Missing | 11 (13) |
| Total | 83 (100) |
Characteristics of patients needing respiratory therapy enrolled in the Home Medical Program (HMP), Madinah HMP Center, Kingdom of Saudi Arabia, 2013.
3.1.2. Patient diagnosis
The top three clinical diagnoses among this study’s patients were respiratory diseases (91.6%), cardiovascular diseases (89.2%), and endocrine diseases (65.1%) (Fig. 1). Those receiving HMP respiratory services enrolled with multiple clinical diagnoses per patient (Fig. 2).
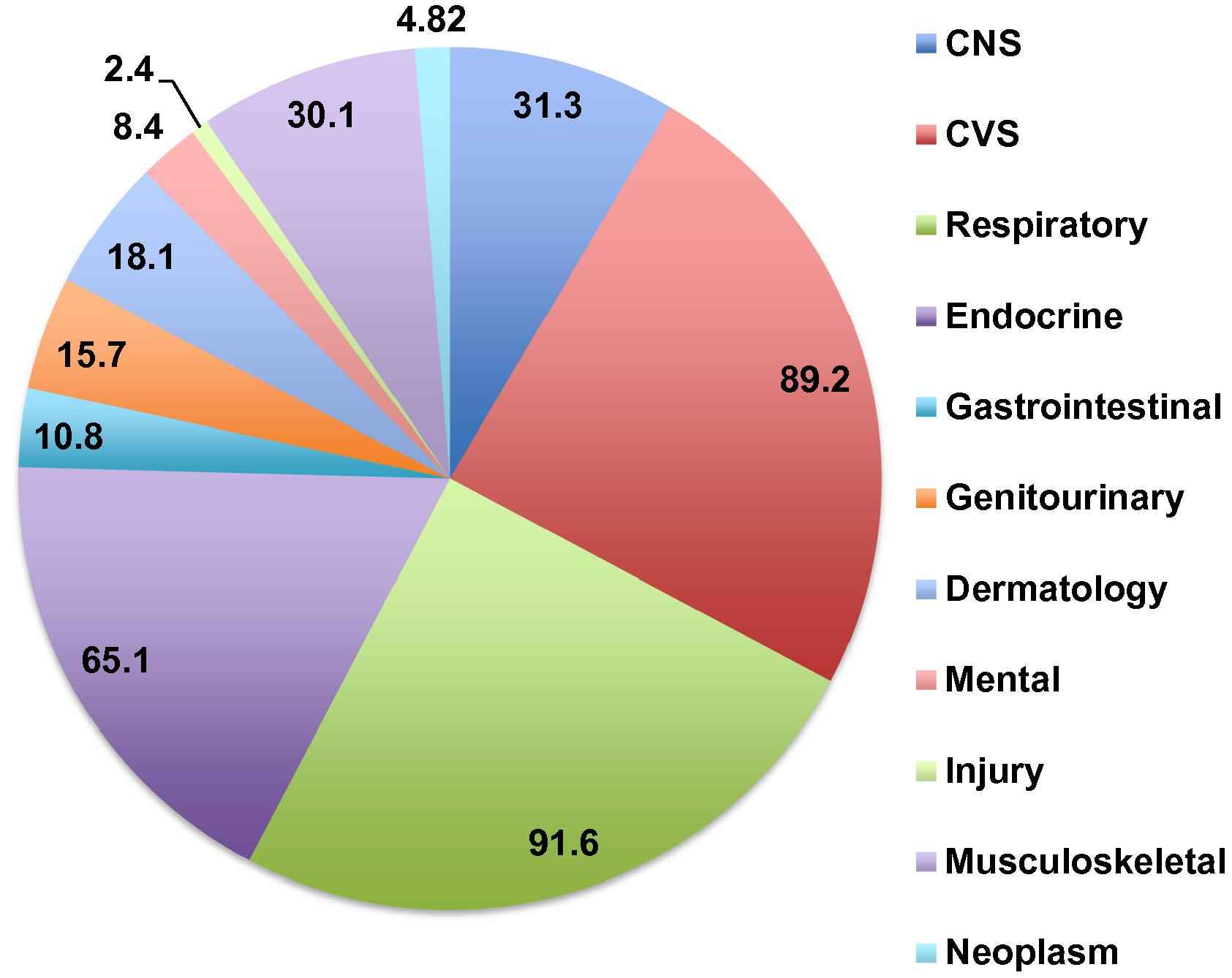
Diagnoses by organ system in patients enrolled through the Madinah Home Medical Program Center, Kingdom of Saudi Arabia, 2013. CNS = Central Nervous System; CVS = Cardiovascular System.
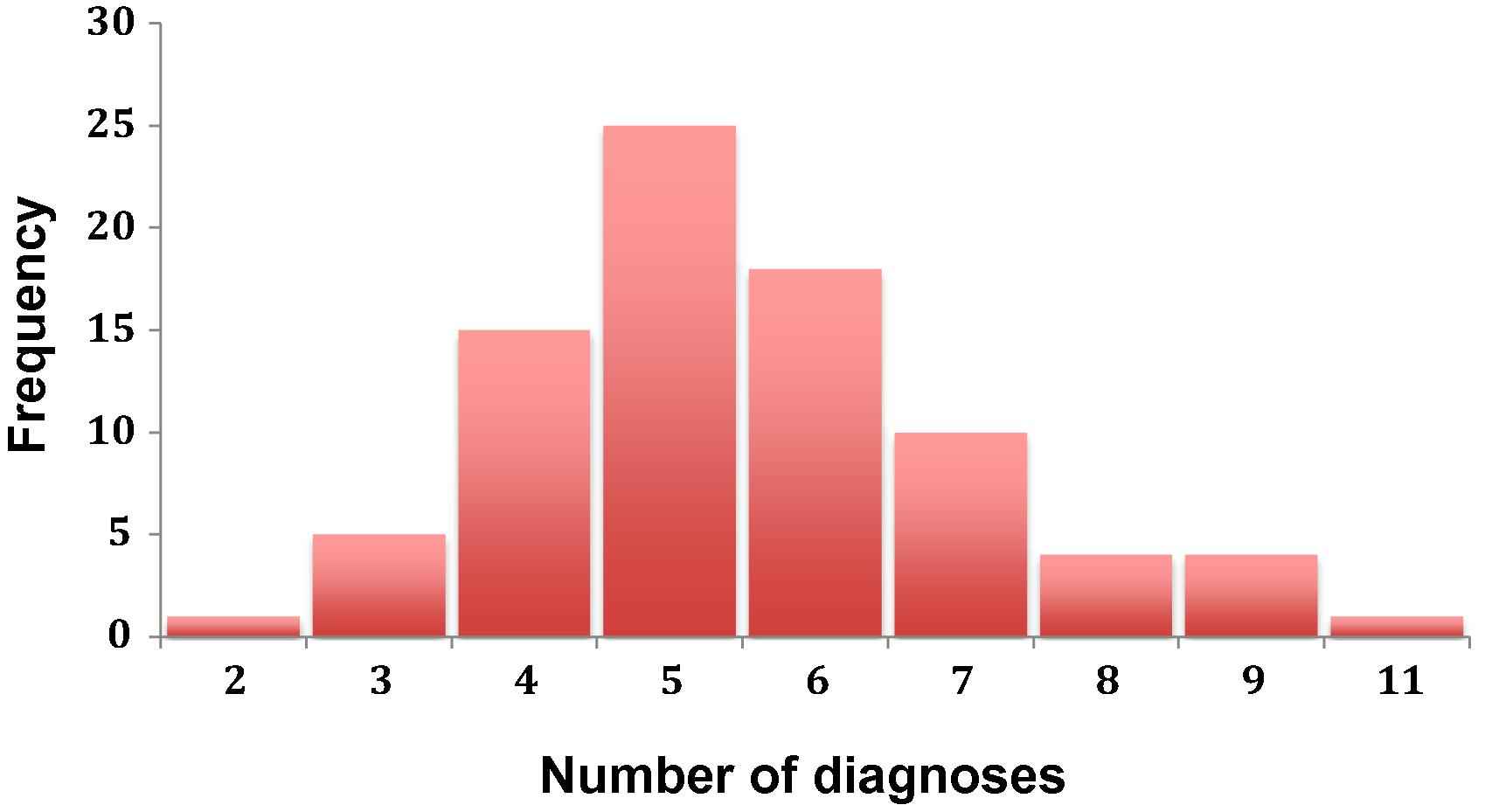
Frequency of diagnosis counts among 83 patients enrolled in the Madinah Home Medical Program Center, Kingdom of Saudi Arabia, 2013.
Asthma accounted for about a third of respiratory disease diagnoses (33.7%). Other diagnoses included chronic obstructive pulmonary disease (10.8%), respiratory failure (9.6%), and lung fibrosis (8.4%) (Table 2).
| Respiratory diagnosis | n (%) |
|---|---|
| Asthma | 28 (33.7) |
| COPD | 9 (10.8) |
| Respiratory failure | 8 (9.6) |
| Lung fibrosis | 7 (8.4) |
| Pulmonary edema | 3 (3.7) |
| TB | 2 (2.5) |
| Others | 19 (22.9) |
| Total | 76 (91.6) |
Based on 10th International Classification of Diseases (ICD-10) N – 83. COPD = Chronic obstructive pulmonary disease; TB = tuberculosis.
Respiratory diagnosesa of patients needing respiratory therapy enrolled in the Home Medical Program (HMP), Madinah HMP Center, Kingdom of Saudi Arabia, 2013.
3.2. Patient profiles needing HRT at the MHMP Center
All 83 patients needed nursing services and health education; in addition, most needed advanced respiratory services (69.9%). Regarding the respiratory modalities, the majority of patients required either two or three modalities, and 8% required four modalities. Almost all of the patients (94%) used treatment respiratory modalities like oxygen therapy, and 14% were on mechanical ventilation (invasive and noninvasive) (Table 3).
| Patient profile | n (%) |
|---|---|
| Services provided | |
| Nursing | 83 (100) |
| Health education | 82 (98.8) |
| Respiratory | 58 (69.9) |
| Physiotherapy | 33 (39.8) |
| Social | 20 (24.1) |
| Dietary | 18 (21.7) |
| Respiratory modalities/patient | |
| One | 17 (20.5) |
| Two | 28 (33.7) |
| Three | 31 (37.4) |
| Four | 7 (8.4) |
| Respiratory modalities administered | |
| Treatment | 78 (94) |
| Supportive | 58 (70) |
| Measurement | 46 (55) |
| Mechanical ventilation | 12 (14) |
Profiles of patients needing respiratory therapy in the Home Medical Program (HMP), Madinah HMP Center, Kingdom of Saudi Arabia, 2013.
3.3. Outcomes
3.3.1. Patient satisfaction toward overall care
Annual satisfaction surveys are distributed to all HMP patients served through the MHMP Center. Data from this survey were available only for 41 patients in this study. According to these survey results, overall patient (or caregiver) satisfaction toward the HMP Center’s services was high: 90.2% of patients were either satisfied or very satisfied, 4.9% were either dissatisfied or very dissatisfied, and 4.9% were uncertain about their response (Table 4).
| Outcomes | n (%) |
|---|---|
| Patient satisfaction | |
| Very satisfied/satisfied | 37 (90.2) |
| Very dissatisfied/dissatisfied | 2 (4.9) |
| Uncertain | 2 (4.9) |
| Total | 41 (100) |
| Patient progress | |
| Not improved/static | 40 (48.2) |
| Improved | 36 (43.4) |
| Deterioration or died | 7 (8.4) |
| Total | 83 (100) |
Outcomes of patients needing respiratory therapy in the Home Medical Program (HMP), Madinah HMP Center, Kingdom of Saudi Arabia, 2013.
3.3.2. Patients’ progress through the HMP
Regarding patient progress through the HMP Center, 43.4% were improved, 48.2% remained static without any improvement or deterioration, and 8.4% deteriorated or died (Table 4).
3.3.3. Hospital utilization during HMP enrollment
Regarding the hospital utilization, around half of the patients had no visits or readmissions to the OPD and ER after enrollment to the HMP. Around one third of the patients had either one visit or two visits (Table 5).
| Hospital utilization after enrollment to the HMP | |
|---|---|
| Readmission | |
| 0 | 47 (56.6) |
| 1 | 27 (32.5) |
| 2 | 8 (9.6) |
| 4 | 1 (1.2) |
| Total | 83 (100) |
| Outpatient department | |
| 0 | 37 (44.6) |
| 1 | 18 (21.7) |
| 2 | 21 (25.3) |
| 3 | 5 (6.02) |
| 4 | 1 (1.2) |
| 5 | 1 (1.2) |
| Total | 83 (100) |
| Emergency room | |
| 0 | 42 (50.6) |
| 1 | 27 (32.5) |
| 2 | 12 (14.5) |
| 3 | 2 (2.4) |
| Total | 83 (100) |
| Sum of all hospital visits/1 y | |
| 0–2 visits | 50 (60.2) |
| >2 visits | 33 (39.8) |
| Total | 83 (100) |
Hospital utilization of patients needing respiratory therapy in the Home Medical Program (HMP), Madinah HMP Center, Kingdom of Saudi Arabia, 2013.
For the hospital utilization (the sum of ER, OPD, and readmissions), half of the patients had between zero and two visits, and 33% had more than two visits (Table 5).
3.4. Cost saving assessment
3.4.1. Pilot study
The second part of this study examined 30/83 patients to evaluate the effectiveness of home respiratory care by comparing the clinical changes in hospital utilization and GCS before and after enrollment through the HMP Center and the estimated cost savings.
3.4.2. Demographic characteristics of this population
Out of the 30 patients in the pilot group, 79.5% were female, 86.7% were Saudi citizens, and 46.7% were married. The demographic of this random subgroup is similar to the demographic of the entire study population and very representative of the 83 patients.
3.4.3. Comparative analysis of hospital utilization
3.4.3.1. ER visits
Patients had a total of 30 ER visits before enrollment in the HMP, which decreased to 13 visits after HMP enrollment (Table 6), with the average reduction of 1.3 visits (SD ± 0.5, p < 0.0001).
| Medical care | n |
|---|---|
| Hospital utilization | |
| Before enrollment | |
| Number of ER visits | 30 |
| Cost of ER visits | $2400 |
| Number of OPD visits | 29 |
| Cost of OPD visits | $1933 |
| Total | $4333 |
| After enrollment | |
| Number of ER visits | 13 |
| Cost of ER visits | $1040 |
| Number of OPD visits | 17 |
| Cost of OPD visits | $1133 |
| Total | $2173 |
| Clinical care | |
| Glasgow Coma Scale | Mean (SD) |
| Before enrollment | 13.0 (1.1) |
| After enrollment | 13.6 (2.4) |
| Mean difference | 0.6 (1.9)* |
ER = emergency room; OPD = outpatient department; SD = standard deviation.
p < 0.08.
Comparative analysis of 30 random patients needing respiratory therapy in the Home Medical Program (HMP) prior to and after enrollment in Madinah HMP Center, Kingdom of Saudi Arabia, 2013.
3.4.3.2. OPD visits
Patients had a total of 29 OPD visits before enrollment in the HMP, which decreased to 17 visits after HMP enrollment (Table 6), with the average reduction of 1.5 (SD ± 1.1, p < 0.0001).
3.4.4. Clinical assessment by GCS
The mean GCS at the hospital prior to HMP enrollment was 13 (SD ± 1.1), with a range between 5 and 15; the mean of the last GCS done at the HMP was 13.6 (SD ± 2.4), with a range between 9 and 15 (Table 6). The mean increase in GCS after enrollment to the HMP was 0.6 (SD ± 1.9), with the paired t test; the difference in the GCS at hospital discharge and the last one done at the HMP was not statistically significant (p < 0.08).
3.4.5. Patient satisfaction
Patient satisfaction improved after enrollment in the HMP, but there was no statistical test applicable to satisfaction ratings.
3.4.6. Cost savings through the HMP
The estimated cost for each ER visit was 300 SAR ($80), so enrollment in the HMP resulted in savings of $1440. HMP enrollment resulted in $800 in savings for OPD visits for this study population (Table 6).
4. Discussion
This study assessed respiratory therapy delivered through the HMP Center in Madinah. Among our many positive findings, HMP care resulted in a high level of overall patient satisfaction, better or stable patient progress than standard care, less frequent hospital utilization, and shorter hospital stays, which led to cost savings. The study provided clinical and financial evidence supporting the provision of HMP respiratory services when comparing the patients themselves at hospital and after enrollment to the HMP.
The findings were similar to what we found in most of the literature. For clinical improvement, our study showed lower hospital utilization, ER, OPD, and readmissions for all kinds of patients, especially those requiring HRT [14–16]. In this study, in addition to hospital utilization, we used the GCS as one of the objective clinical measures to assess patient health improvement; these figures reflected improvement in the score, but were not statistically significant (p > 0.05). For clinical assessment, other studies used many indicators and measures, such as using a scale for assessing the patients’ functional status, especially among the elderly at home [14], or assessing the wound care or bed sores among the elderly.
In terms of quality of life and patient satisfaction, this study revealed a high level of overall satisfaction, which was also seen in other studies nationally and internationally [11,17,18].
The cost benefit of the HHC was not firmly established in the literature; many studies showed it to be one of the most effective cost-saving approaches, but some research revealed there to be inconsistent results [19]. This study found cost benefits among the pilot group. The pilot group’s results, a comparison of variables before and after HMP enrollment, indicated improvement clinically (ER, OPD, GCS), in quality of life (satisfaction), and also economically, through savings achieved through reduced hospital utilization. This shows the value of respiratory services delivered through the HMP. This pilot group sample was different from the other 53 patients only in their severity scores; otherwise, they were similar (e.g., in amount of prior hospital utilization). In essence, the findings related to this pilot group could be applicable to the rest of the patients.
Although small, the 83 patient sample was a good representation of the population, as seen by the normal distribution of the number of diagnosis counts, and this strengthened the study. The patients were equally distributed (Fig. 2).
As mentioned earlier, even though there is ample evidence of the various benefits of incorporating HHC in the health system, this evidence has not come from the KSA until now. The services provided through the HMP are different from those offered in other countries, and this pilot was the first study that assessed the effectiveness of HHC in the KSA as well as the first that has provided evidence of its cost-effectiveness.
This study had several limitations. The lack of sufficient objective clinical measures was a limitation. The use of additional objective clinical indicators is recommended for future studies. Another limitation of this study was the small sample size, although it was the total number of patients enrolled in the HMP who had a respiratory diagnosis or needed respiratory care. Having a larger sample size would increase the power of the study, and the association and variance between variables could be estimated more accurately. Another limitation was that it was a secondary data analysis from medical records, and this could have meant information bias. A prospective study that regularly monitors patient changes would produce more valid data and reduce instances of data being unavailable. Assessing elderly persons with comorbidities is challenging, and in such cases, it is difficult to control the confounders that could have affected the patients’ health, due to the complexity of the interventions for the elderly [20].
We now have a better view of the HMP’s achievements and its contribution to reducing hospital utilization and healthcare costs. At the same time, the HMP maintained the same or a better level of care compared to hospitals, with more satisfaction and better health outcomes. Evidence provided here and in previous studies supports the effectiveness of the HMP and justifies the need for more funding from the MoH, especially for patients who have a respiratory illness or need respiratory care. A study encompassing more HMP patients using prospective performance and the impact evaluation measures is the next step.
5. Conclusions
This study revealed that respiratory therapy delivered through the MHMP Center was a valuable approach both clinically and economically. There were decreases in hospital utilization, improvements in overall patient satisfaction, and cost savings when patients with respiratory illness or patients needing respiratory care were treated at home.
6. Recommendations
We recommend broadening this study to include more patients in the future. We also recommend conducting a prospective study to ensure the accuracy of collected data and to better evaluate the patient outcomes. Since insufficient data were an obstacle, keeping better records or using an electronic filing system would be advisable. There were limitations in the clinical outcome indicators. Objective, measurable indicators should be included in subsequent studies. In evaluating the cost-effectiveness of any health intervention, we should have data such as disability-adjusted life year (DALY) that help us estimate the cost in the equation of health cost-effectiveness. Additional prospective studies or randomized trials are advisable for better evaluation and cost analysis comparison outcomes.
Conflicts of interest
None.
Acknowledgments
I would like to thank the Home Medicine General Department in the MoH and the Madinah Home Medical Program Center staff for helping me carry out this study. Special thanks to Dr. Aeshah Al-Saghier, Dr. Nevien Awad, Dr. Salem Aldahi and Mr. Ahmed Maseheli for their support and guidance when I started working on and formulating this work. Also, I would like to express my thanks to each person who was involved directly or indirectly in this research – the public health professionals at the MoH, my colleagues and instructors at the Rollins School of Public Health and in the King Abdullah Fellowship Program – their support and cooperation were integral to the completion of this paper.
Appendix 1
| Dependent variable | Description |
| Outcome measures | |
| Clinical progress | Evaluated the following variables depending on clinical judgment as nominal categories |
| 0) Improved | |
| 1) Static (not improved) | |
| 2) Deterioration or death | |
| Glasgow Coma Scale | Glasgow Coma Scale is a discrete numerical variable from 3 to 15 |
| ER visits | Discrete number of ER visits |
| OPD visits | Discrete number of OPD visits |
| Patient satisfaction | Evaluated the following as a categorical variable for this question from Home Care Client Satisfaction Instrument-Revised (HCCSI-R) “How satisfied you were with your overall care?” [12,13] |
| 0) Very dissatisfied/dissatisfied | |
| 1) Very satisfied/satisfied | |
| 2) Uncertain | |
| 3) Not available | |
| Independent variable | Description |
| Demographics | |
| Age | Evaluated as a categorical variable |
| 0) 18–60 y of age | |
| 1) 61–80 y of age | |
| 2) > 80 y of age | |
| Sex | Evaluated as a binary variable |
| 0) Male | |
| 1) Female | |
| Marital status | Evaluated as a binary variable |
| 0) Married | |
| 1) Non-married | |
| Nationality | Evaluated as a binary variable |
| 0) Saudi | |
| 1) Non Saudi | |
| Clinical diagnosis | |
| Patients diagnoses | Evaluated the diagnosis according to ICD-10 as categorical variables |
| Diagnosis counts | Evaluated the number of diagnoses per patients as |
| 1) No. of the patients who have one diagnosis | |
| 2) No. of the patients who have two diagnoses | |
| 3) No. of the patients who have three diagnoses | |
| 4) No. of the patients who have four diagnoses | |
| 5) No. of the patients who have five diagnoses | |
| Specific system diagnosis | Evaluated each specific organ system diagnosis as categorical variables |
| Clinical care at the HMP | |
| HMP services utilized | Evaluated the services utilized in the HMP as |
| 0) Nursing services | |
| 1) Advanced respiratory services | |
| 2) Social services | |
| 3) Physiotherapy services | |
| 4) Nutritional services | |
| 5) Health education | |
| Respiratory modalities | Evaluated the respiratory modalities utilized in HMP as |
| 0) Measurement modalities (pulse oximetry, spirometer) | |
| 1) Treatment modalities (tracheostomy, MDI, nebulizers, oxygen cylinder) | |
| 2) Mechanical ventilation (invasive and noninvasive as CPAP & BiPAP) | |
| 3) Supportive modalities (oxygen concentrator, suction machine, bag valve mask and chest physiotherapy) | |
ER = emergency room; OPD = outpatient department; HMP = Home Medical Program; ICD-10 = 10th International Classification of Diseases; MDI = Metered Dose Inhaler; BiPAP = Biphasic Positive Airway Pressure; CPAP = continuous positive airway pressure.
Description of dependent and independent variables used in this study.
References
Cite this article
TY - JOUR AU - Rana A. Alhelali AU - Scott J.N. McNabb AU - Ziad A. Memish PY - 2015 DA - 2015/08/21 TI - Evaluation of home respiratory therapy delivered to patients in the Ministry of Health’s Home Medical Program (HMP) and administered through the Madinah HMP Center, Kingdom of Saudi Arabia, 2013 JO - Journal of Epidemiology and Global Health SP - 19 EP - 27 VL - 6 IS - 1 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2015.07.006 DO - 10.1016/j.jegh.2015.07.006 ID - Alhelali2015 ER -