
Building Capacity for Mortality Statistics Programs: Perspectives from the Indonesian Experience
- DOI
- 10.2991/jegh.k.190429.001How to use a DOI?
- Keywords
- Mortality; causes of death; death registration; CRVS systems; capacity building; statistics
- Abstract
Information on deaths by age, sex, and cause are primary inputs for health policy and epidemiological research. Currently, most developing countries lack efficient death registration systems that generate these data on a routine and timely basis. The global community is promoting initiatives to establish and strengthen national mortality statistics programs across the developing world. Building human, technical, and institutional capacity to operate these programs are essential elements for the program. In Indonesia, the government has established a national Sample Registration System (SRS) covering a population of 9 million and is looking toward further scaling up of operations of the mortality statistics program in conjunction with expansion of the national Civil Registration and Vital Statistics (CRVS) systems. This article reports the theoretical and practical perspectives gained from experiences in developing human capacity in the Indonesian context. These perspectives are described in terms of the institutional, personnel, and functional components of the program for collection, compilation, analysis, and utilisation of mortality and cause of death data. The article also describes the challenges and potential solutions for implementing capacity building activities at national and subnational level. In conclusion, the need for and availability of training resources are discussed, including the potential for involvement of public health academia and international collaborations within a research framework on program management, quality evaluation, and data utilisation. Adequate attention to capacity building is essential to ensure the success and sustainability of national mortality statistics programs.
- Copyright
- © 2019 Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Mortality statistics are essential for population health assessment, planning, evaluation, and research. The United Nations Sustainable Development Goals (UNSDGs) have listed 14 indicators that require reliable data regarding deaths by age, sex, and cause on a routine annual basis for monitoring progress toward these goals [1]. Yet, a considerable number of countries do not have functional mortality statistics programs to generate the required data to measure these indicators [2]. Therefore, in the absence of empirical data, there is an increasing reliance on modelled estimates of these indicators for most developing countries [3]. There is an urgent need for national empirical data to strengthen the measurement and political relevance of these indicators to guide health policy for UNSDGs.
Approximately 15 years ago, Indonesia embarked on its journey toward developing a national mortality statistics program. Starting with a pilot project covering three field sites on Java in 2005, the program expanded into a sentinel mortality surveillance activity covering sites on all major islands over the period up to 2011 [4,5]. Building on these experiences, Indonesia launched its national Sample Registration System (SRS) in 2014, covering 128 sub districts located in 30 provinces across the country, and a population of about 9 million [6]. More recently, the international community has emphasised the importance of national Civil Registration and Vital Statistics (CRVS) systems as the optimal source of mortality statistics for health development. Therefore, as part of the CRVS “Get everyone in the picture” decade 2015–2024 initiative led by the United Nations Economic and Social Commission for Asia Pacific [7], Indonesia is looking toward further expansion of the coverage of mortality statistics activities in alignment with scaling up of national CRVS operations. A critical challenge lies in building institutional and human capacity to enable program expansion. Here, we describe theoretical and practical perspectives gained from experiences in building human resources along the course of developing the mortality statistics program in Indonesia.
2. ORGANISATIONAL ASPECTS OF MORTALITY STATISTICS PROGRAMS
Figure 1 depicts the sequential stages involved in the organisation of mortality statistics programs in terms of the process by which information on deaths in a population and their causes is eventually utilised for health sector policy and research [8]. As observed, the process involves multiple institutions and personnel, ranging from community level registration offices through health facilities to regional and national health, statistical, and research agencies.
Each stage involves several administrative and technical functions that are required for compilation, evaluation, and analysis of mortality data. Hence, a robust organisational structure with intersectoral coordination mechanisms is necessary to provide a strong framework for mortality statistics operations [9]. Establishing such a framework requires high-level capacity in strategic planning and organisation, with an appropriate perspective of institutional mandates, roles, and resources in this area of work. The need for a broad and long-term vision for engaging in such developmental activities cannot be overemphasised.
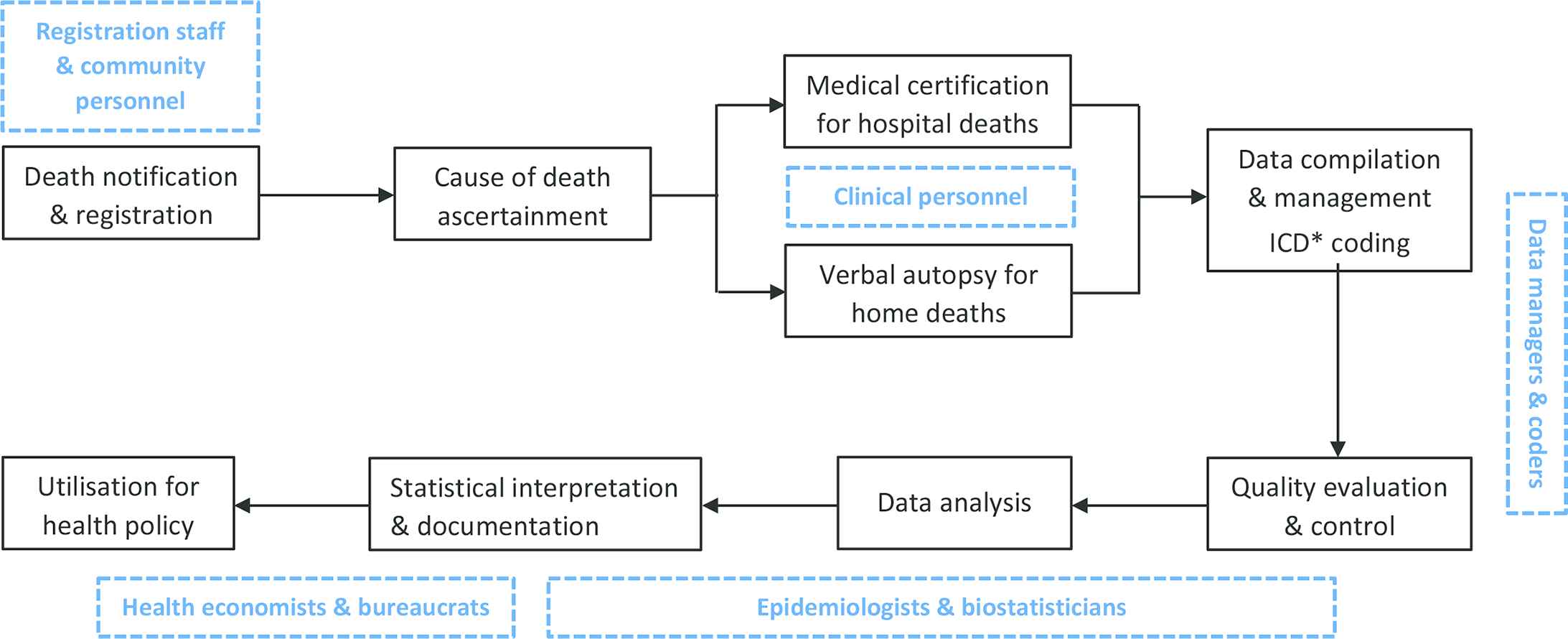
Information processes in mortality statistics programs highlighting key functions that require targeted capacity building activities. *ICD; International Classification of Diseases and Health Related Problems, Tenth Revision (ICD-10).
3. FUNCTIONAL AND TECHNICAL PERSPECTIVES OF CAPACITY BUILDING
From a functional perspective, the mortality statistics program would require adequate human capacity for several broad purposes, each of which will require personnel equipped with a range of technical competencies and skills. These are summarised across institutions, personnel, and their functions in Table 1. First, there is a need for trained personnel to provide quality assurance at the point of data capture in terms of complete identification and reporting of all deaths. Therefore at the primary level, careful attention should be paid to train local civil registrars and notifiers of vital events about the rules, forms, and procedures for death notification and registration while also emphasising the imperative for them to ensure high quality of data. Accurate data capture is also required for information on causes of death, for which skills are required at both community health centres and hospitals, encompassing a range of separate but closely related functions involved in assigning and coding causes of death from available clinical information.
| Node | Personnel | Functions | Capacity building elements |
|---|---|---|---|
| Community |
|
|
|
| Civil registration office |
|
|
|
| Community health centres |
|
|
|
| Hospitals |
|
|
|
| District/city health offices |
|
|
|
| Province/state health departments |
|
|
|
| National health planning/statistics office |
|
|
|
Local notifier network usually includes village health workers, religious leaders, police, and local social service agencies.
Capacity building requirements for establishing national mortality statistics programs
Next, although data compilation and management may appear to be largely administrative functions, there is a need for adequate human capacity to maintain strict oversight of efficiency in reporting compliance across the large scale of territorial and institutional coverage of death registration systems. Therefore, at intermediate organisational levels, the administrative functions of data compilation and management get combined with technical functions of data quality evaluation and analysis, requiring personnel with adequate skills from both perspectives. An additional layer of competencies involves the ability to provide leadership and technical guidance to peripheral units, along with logistics and other forms of program support.
Third, given the complexity of information on causes of death, specialised skills are required for accurate data analysis, interpretation, and documentation of results. In general, expanding mortality statistics programs tend to record higher numbers of deaths, but with limitations in cause attribution owing to the additional complexities of this function. Therefore, available data from the statistics program would first need to be closely evaluated for potential biases in regard to completeness and validity of causes of death [10]. There is a need for skills in demographic and epidemiological analysis, accompanied by experience in data interpretation and utilisation for health policy and research. This could require engagement with research organisations and academia where human capacity for these tasks is available.
Finally, statistical outputs need to be translated by experienced policy analysts into appropriate evidence for health policy evaluation as well as formulation by informed health decision makers and bureaucrats. Health program managers at regional levels also require skill development to utilise mortality indicators for evaluating program performance and guide interventions. Policy analysts also need to monitor national mortality trends and differentials, and report statistics for international comparisons and over time.
4. CHALLENGES AND SOLUTIONS FOR CAPACITY DEVELOPMENT
Challenges in implementing capacity building in Indonesia were realised from the detailed evaluation of SRS [5], which identified important limitations in data completeness and accuracy. To solve these limitations, a large-scale capacity building initiative is currently underway involving collaboration between Indonesian and Australian academic institutions funded by a bilateral government partnership program. The collaboration first analysed the reasons for poor data quality and identified the lack of adequate capacity at the point of data capture, an inefficient centralised program for data management, and limited skills in data quality evaluation and analysis at all levels.
In addressing these limitations, the collaboration identified two general challenges in capacity development for mortality statistics programs. First, in large populations, a considerable, widely dispersed work force is involved in these operations, which will require a range of targeted skill development activities. This was the case in the Indonesian SRS, which involves operations in 252 health centres serving 1575 villages and urban wards in the sample sites. This necessitates commitment of considerable financial resources along with the availability of a critical mass of trained resources for capacity building. A second challenge is that almost all personnel involved in SRS field operations are already in regular government employment, as would be the case in other countries as well. These staff personnel require in-service training, which carries the hazards of managing change in existing work environments. Careful planning is necessary to negotiate these two challenges, and where necessary, an incremental approach to capacity building may be required in large populations and/or where training resources are limited.
An important consideration in the design of capacity building activities lies in delivery through several different modes. For instance, the Indonesian experience has shown that in addition to in-class briefings, careful attention is required for practical elements of skill development such as exercises in completing registration forms, complying with rules and procedures, conducting household interviews, and completing medical certificates of cause of death. Field supervision, “on-the-job” training, and feedback on work performance and data quality are also essential strategies to follow-up knowledge conveyed at workshops. In the absence of formal educational qualifications to directly support this area of work, capacity building through postgraduate research projects as well as doctoral research studies are alternative potential mechanisms for developing technical and leadership skills in mortality statistics activities, as per the research framework outlined in Table 2. Elements of this framework are currently being implemented in Indonesia.
| Research theme | Topic | Utility |
|---|---|---|
| Program management | Reporting timeliness from registration and health sector institutions | Monitoring reporting compliance |
| Annual audit of registration staff/resources | Resource allocation | |
| Program feasibility and sustainability | Program strengthening interventions | |
| Data quality evaluation | Periodic field supervision and quality control | Evidence for targeted capacity building |
| Demographic analysis of data completeness | Adjustment factors for mortality estimates | |
| Validation of reported causes of death | ||
| Mortality outcomes research | Descriptive research on mortality levels, causes, trends, and differentials | Evidence for population health assessment |
| Analysis of aetiology and pathophysiology | ||
| Biological, behavioural and environmental risk factors for mortality | Outcome measures for clinical and epidemiological research | |
| Health policy analysis | Health program evaluation | Policy impact analysis |
| Econometric analysis | Cost effectiveness analysis | |
| Population health forecasting | Future implications |
Research framework for strengthening quality and utility of data from national mortality statistics programs
In the current environment, electronic platforms for data management have vastly improved program efficiency in terms of data compilation and processing, as well as quality evaluation and analysis. In the Indonesian context, the collaboration has developed an electronic data management system and is facilitating its implementation at district health offices and health centres as part of a comprehensive decentralisation strategy to improve system performance. However, as mentioned earlier, such decentralisation also poses challenges in developing adequate capacity for careful assessment of data quality and adjustment for potential data biases. As reporting performance improves, data managers will also be trained to effectively trace problems with data quality to the source, resulting in record verification as well as feedback to improve staff performance.
5. TRAINING RESOURCES
In Indonesia, the National Institute of Health Research and Development (NIHRD) in the Ministry of Health is nominated as the central technical agency to lead the national mortality statistics program. Capacity for all the above mentioned functions has been developed in the NIHRD through international research collaborations. However, rolling out capacity building across a vast country requires additional training resources, which are currently being developed through a network of public health academic institutions. These institutions play a role in the development and delivery of preservice and in-service training for staff across the institutional network of the program. Further, capacity building activities also need to be incorporated into regular monitoring and evaluation functions of personnel from district and provincial offices through field supervision and feedback on data quality. Arrangements are also underway to make available training resources to support tertiary data analyses and policy exercises through international academic and research collaborations.
6. CONCLUSION
There is an urgent need to improve the empirical basis for mortality measurement in developing countries. Capacity building for mortality statistics programs is an essential element that requires a strategic vision along with careful attention to technical detail. Establishing a critical mass of human resources at national level within an institution with a clear mandate and role in the national mortality statistics program is a primary step. As described earlier, there are a range of personnel and functions for which capacity is required, all of which require adequate attention for the overall success of the program. Close engagement within the network of involved institutions, public health academia, and international research collaborations will improve the availability of training resources to undertake capacity building responsibilities. Political will and funding support are necessary to ensure appropriate attention to capacity building as the cornerstone of sustainable initiatives to develop national mortality statistics programs.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
AUTHOR CONTRIBUTIONS
CR prepared the initial draft of the manuscript. YU contributed to the design and content of the tables. All authors critically reviewed the initial draft and approved the final version of the submitted manuscript.
ACKNOWLEDGEMENTS
All authors affiliated with the NIHRD, Indonesia, are employees of the Indonesian government. CR and MK are partially supported by a development partnership grant from the Department of Foreign Affairs and Trade, Australia, which also supports part of the capacity building activities described in this manuscript.
References
Cite this article
TY - JOUR AU - Chalapati Rao AU - Yuslely Usman AU - Matthew Kelly AU - Trijuni Angkasawati AU - Soewarta Kosen PY - 2019 DA - 2019/05/09 TI - Building Capacity for Mortality Statistics Programs: Perspectives from the Indonesian Experience JO - Journal of Epidemiology and Global Health SP - 98 EP - 102 VL - 9 IS - 2 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.190429.001 DO - 10.2991/jegh.k.190429.001 ID - Rao2019 ER -