
Impact of Advocacy, Communication, Social Mobilization and Active Case Finding on TB Notification in Jharkhand, India
- DOI
- 10.2991/jegh.k.190812.002How to use a DOI?
- Keywords
- Tuberculosis epidemiology; tuberculosis prevention and control; disease notification; multilevel analysis; program evaluation
- Abstract
Community-level benefits of screening for active tuberculosis (TB) disease remain uncertain. Project Axshya (meaning free of TB) conducted advocacy, communication, social mobilization, and active case finding among vulnerable/marginalized populations of India. Among 15 districts of Jharkhand state, the project was initiated in 36 subdistrict level administrative units – tuberculosis units (TUs) in a staggered manner between April 2013 and September 2014, and continued till the end of 2015. Seven TUs did not implement the project. We assessed the relative change in the quarterly TB case finding indicators (n = 4) after inclusion of a TU within the project. By fitting four multilevel models (mixed-effects maximum likelihood regression using random intercept), we adjusted for secular (over previous five quarters) and seasonal trends, baseline differences within Axshya and non-Axshya TUs, and population size and clustering within districts and within TUs. After inclusion of a TU within the project, we found a significant increase [95% confidence interval (CI)] in TU-level presumptive TB sputum examination rate, new sputum-positive TB Case Notification Rate (CNR), sputum-positive TB CNR, and all forms TB CNR by 12 (5.5, 18.5), 1.1 (0.5, 1.7), 1.3 (0.6, 2.0), and 1.2 (0.1, 2.2) per 100,000 population per quarter, respectively. Overall, the project resulted in an increase (95% CI) in sputum examination and detection of new sputum-positive TB, sputum-positive TB and all forms of TB patients by 22,410 (10,203, 34,077), 2066 (923, 3210), 2380 (1162, 3616), and 2122 (203, 4059), respectively. This provides evidence for implementing project Axshya over and above the existing passive case finding.
- Copyright
- © 2019 Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Globally, there were an estimated 10 million new patients with tuberculosis (TB) in 2017. Of these, 2.7 million (27%) were in India and 0.42 million people died due to TB [1,2]. Despite significant gains made by India’s Revised National TB Control Programme (RNTCP) in terms of lives saved, India still accounts for one-third of ‘missing’ 4.3 million patients with TB globally [3]. Advocacy, Communication, Social Mobilization (ACSM), and community-based Active Case Finding (ACF) have the potential to enhance the patient-initiated pathway to TB diagnosis and close the gaps within the TB cascade [4,5].
Even in high-burden countries, certain marginalized or vulnerable populations are more prone for the disease and therefore screening these populations has been recommended to detect all TB patients early and to ensure their treatment completion [5]. According to the 90–(90)–90 targets set by the ‘global plan to end TB (2016–2020),’ in 2015, the second 90 deals with reaching 90% of TB among vulnerable/marginalized populations [6].
In line with the strategic vision of RNTCP (2012–2017), project ‘Axshya’ (meaning free of TB) was implemented to enhance the reach and visibility of RNTCP services among vulnerable/marginalized populations and mitigate the impact of TB on the country through ACSM and ACF. The ACF was known as Axshya SAMVAD (meaning conversation). SAMVAD stood for Sensitization and Advocacy in Marginalized and Vulnerable Areas of the District. Although these activities were resulting in high and equitable coverage of TB awareness, detection of large numbers of TB patients, and reduction in delays and costs due to TB diagnosis [7–11], there was very limited information on whether they were increasing the TB case finding indicators [Case Notifications Rates (CNRs)] at population level when compared with areas where Axshya was not implemented.
Globally, the epidemiological impact of Passive Case Finding (PCF) has been inadequate, and individual and community-level benefits from community-based ACSM and screening for active TB disease remains uncertain [12–14]. One of the key indicators to determine the impact on patient detection (population-level benefits) is an initial increase in the TB CNRs, while long-term positive effect (impact on TB epidemiology) is a decline in CNR (up to 10 years from screening initiation, assuming continued case finding intensity and effectiveness) when compared with PCF alone [13]. Therefore, in settings where large-scale ACSM and screening activities (like project Axshya) have been implemented, it is recommended that a rigorous and consistent assessment of TB notification and mortality rates be carried out over prolonged periods of time [15].
This study therefore was planned to determine the relative changes in programmatic TB CNRs in geographic areas where project Axshya was implemented when compared with areas where Axshya was not implemented in the state of Jharkhand, India (2013–15). Our hypothesis was that the project resulted in significant change in CNRs after adjusting for baseline differences, and secular and seasonal trends.
2. MATERIALS AND METHODS
2.1. Study Setting
2.1.1. General setting
Jharkhand is a landlocked state in east India with a population of 33 million, 76% residing in rural areas, and a literacy rate of 67% [16]. Administratively the state is divided into 24 districts [16] (Figure 1). It is one of the five least developed states of India [17]. The annual CNRs were lower in Jharkhand during 2015 and 2016 than the average national rates per 100,000 population (97 and 96 per 100,000 population compared with 111 and 109 per 100,000 population, respectively) [18,19].
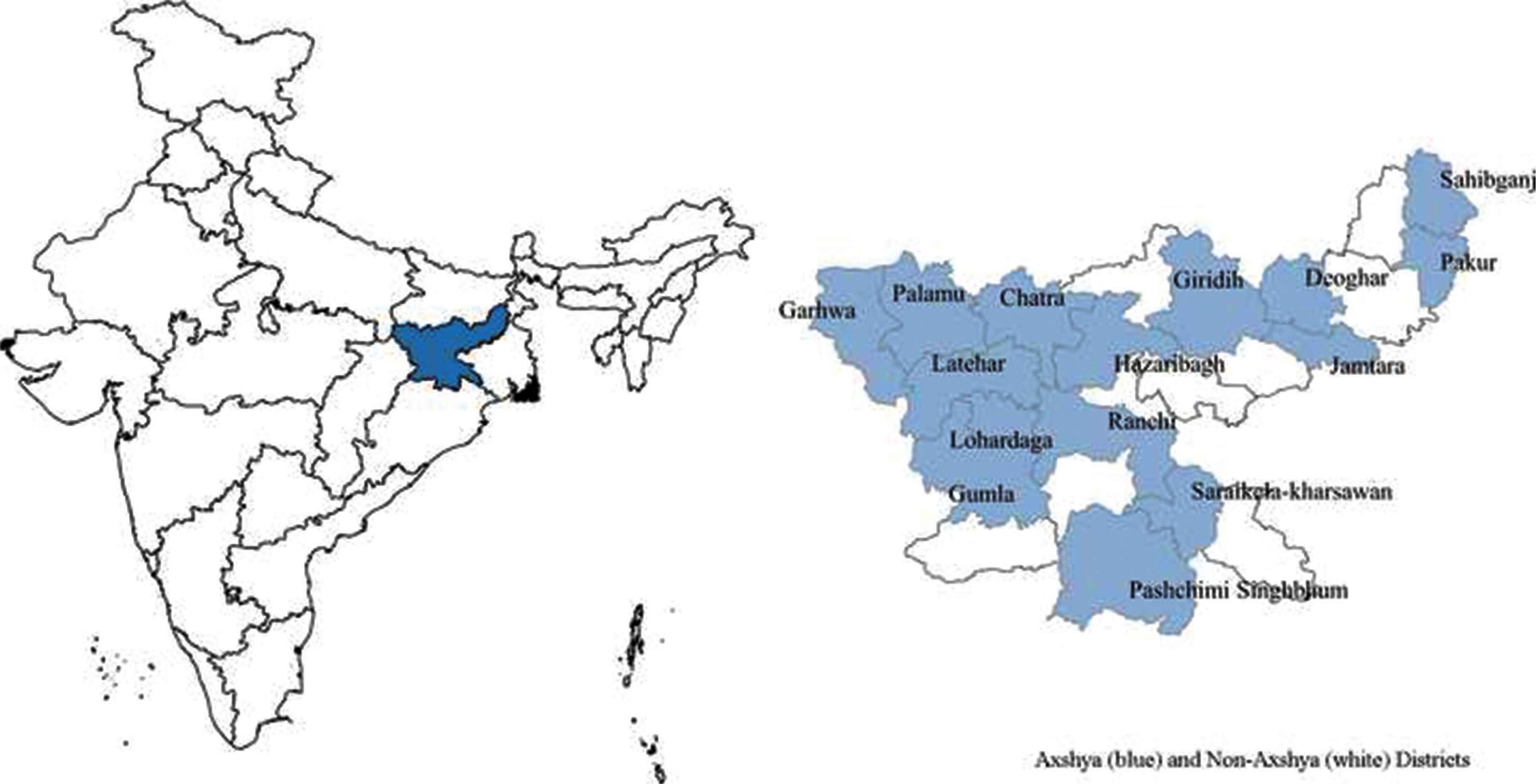
Location of Jharkhand state in India along with the Axshya (n = 15) and non-Axshya districts (n = 9), 2013–15.
This study included 15 Axshya districts. Of the 15 districts under phase II of project Axshya in the state, there were 43 TUs. Seven TUs were not covered under the project throughout (non-Axshya TUs). Among Axshya TUs, inclusion of TUs under the project began in Apr–Jun 2013 and eventually all 36 TUs were included by Jul–Sep 2014.
2.1.2. RNTCP in Jharkhand (2013–15)
Tuberculosis patients were being detected predominantly through PCF. The RNTCP infrastructure included a district TB center for each district, subdistrict level program management units called TB units (TUs – one for 500,000 population) and Designated Microscopic Centers (DMCs – one for 100,000 population) for sputum microscopy. These worked under the administrative control of the State TB officer. Patients with presumptive TB visited the DMCs for sputum examination and once diagnosed with TB, were registered at TU level for anti-TB treatment [20]. Laboratory registers maintained in each DMC contained details of each person who underwent sputum smear microscopy and TB registers maintained at each TU indicated the number of TB patients treated under RNTCP. RNTCP had its own quarterly reporting system that was first generated at TU level, then collated at district level followed by at state level [21].
2.2. Project Axshya (2013–15) – The Intervention
It was implemented in India by The Union South-East Asia (New Delhi). Funded by The Global Fund against AIDS, TB and Malaria, phase II was implemented between quarter 2 (Apr–Jun) of 2013 and quarter 3 (Jul–Sept) of 2015 in 300 districts spread across 21 states in collaboration with more than 1000 civil society organizations [22–25].
In Jharkhand, 15 districts and 36 TUs (of the 43 TUs in these 15 districts) were identified at the beginning of 2013 in consultation with the program of the state as Axshya districts and Axshya TUs, respectively (Figure 1). Even within an Axshya TU, activities were preferentially targeted toward marginalized and vulnerable populations (Table 1). Project activities were initiated in the Axshya TUs in a phased/staggered manner. Once initiated, the project activities continued throughout the project period (Table 2 and Figure 2). Each Axshya district had a district coordinator who was supervised by the assistant program manager, the state technical consultant, and program management unit at The Union office in New Delhi, India.
|
Schedule caste/tribe are terms used in Indian Constitution
Marginalized or vulnerable population where advocacy, communication, social mobilization, and active case-finding activities were targeted under phase II, Project Axshya (2013–15).
| Implementation details | Value |
|---|---|
| Number of districts | 24 |
| Number of Axshya districts | 15 |
| Number of TUs in Axshya districts | 43 |
| Number of TUs in Axshya districts that remained non-Axshya TUs throughout 2013–15 | 7 |
| Number of TUs eventually included as Axshya TUs | 36 |
| Quarter when inclusion of TUs under phase II of project Axshya started | Apr–Jun 2013 |
| Axshya TUs during Apr–Jun 2013 | 27 |
| Axshya TUs during Jul–Sep 2013 | 29 |
| Axshya TUs during Oct–Dec 2013 | 31 |
| Axshya TUs during Jan–Mar 2014 | 33 |
| Axshya TUs during Apr–Jun 2014 | 33 |
| Axshya TUs during Jul–Sep 2014 | 36 |
Tuberculosis units are subdistrict level administrative units under Revised National Tuberculosis Control Programme.
TU, Tuberculosis units.
Implementation of phase II of project Axshya in Jharkhand, India, 2013–15

Grid diagram indicating the number of TUs implementing and not implementing project Axshya at various time periods in 15 Axshya districts in Jharkhand, India, between 2012 and 2015.
Grids shaded in gray indicate that the TU was implementing project Axshya for the corresponding time period. Each time period indicates one quarter of a year beginning from quarter 1 (Jan–Mar) 2012 and ending with quarter 4 (Oct–Dec 2015). Of the 15 districts under phase II of project Axshya in the state, there were 43 TUs. Seven TUs were not covered under the project throughout (non-Axshya TUs). Among Axshya TUs, inclusion of TUs under the project began in Apr–Jun 2013 and eventually all 36 TUs were included by Jul–Sep 2014. TU1–TU36, Axshya TUs; TU37–TU43, non-Axshya TUs.
The activities under phase II were: creation of Axshya villages, Sputum Collection and Transport (SCT), rural healthcare provider engagement, non-governmental organization engagement with RNTCP schemes, strengthening district TB forums, and Axshya SAMVAD. The activities were conducted with the support of trained community volunteers (Axshya Mitras, friends of Axshya) from local grassroots level non-governmental organizations in coordination with district- and TU-level RNTCP staff. Activity-based honorarium was provided with inbuilt quality control mechanisms [23]. The district coordinator provided a 1-day training to Axshya Mitras about collecting quality sputum specimen and identifying presumptive TB using the symptomatic verbal screening criteria – more than 2 weeks of cough, and/or evening rise in temperature, loss of appetite, and loss of weight (any one).
Following the mapping of vulnerable/marginalized areas, a series of mid-media activities were conducted (announcement through microphones, wall painting, and canopy at market days). Under Axshya SAMVAD, Axshya Mitras conducted house-to-house visits to create awareness about TB, identify presumptive TB, and refer them to the nearest public DMCs for sputum examination. Axshya Mitras also provided an option for SCT services for patients who had difficulty in reaching the DMCs. Axshya Mitras also visited and sensitized the rural healthcare providers who also supported in referral or SCT. SCT services were also provided at a few facilities where patients were identified during outpatient visits at non-DMC public facilities.
Irrespective of the size of the population or the volume of the vulnerable/marginalized populations, the upper limit of activities that could be conducted in a district in a quarter remained more or less fixed (3000 households visited under Axshya SAMVAD, 300 SCTs, 60 community meetings, and 10 mid-media activities). At any given quarter, >90% of the planned activities were implemented. These activities have been summarized in Table 3. Project Axshya also provided technical support to RNTCP at state level through its state technical consultant. One of the expected benefits of these activities was an increase in the TB CNRs at TU level.
| Activities | Value |
|---|---|
| Number of Axshya Mitras trained | 1090 |
| Number of community meetings done | 7667 |
| Number of mid-media activities done | 716 |
| Number of households covered under Axshya SAMVAD | 409,091 |
| Number of patients with TB sensitized on patient charter | 4556 |
| Number of non-governmental organizations trained in program schemes | 211 |
| Number of health staff trained in soft skills | 685 |
| Number of Axshya villages formed | 444 |
| Number of rural healthcare providers (informal sector) trained | 1353 |
| Number of patients examined at designated microscopy centers through patient referrals | 7010 |
| Number of patients examined at designated microscopy centers through sputum collection and transport | 34,158 |
Axshya Mitras, used colloquially for village-level community volunteers working for project Axshya (Mitras in Hindi means friends);
Axshya SAMVAD, used colloquially for active case-finding strategy under the project (SAMVAD in Hindi means communication);
Axshya village, a village where the community is aware of tuberculosis care and control.
Summary of activities under phase II of project Axshya in Jharkhand, India, 2013–15
Project Axshya maintained its own reporting system through the project management unit at New Delhi, and starting point of the same was the monthly report submitted by the district coordinator. It only contained information on the number of activities and number of patients detected directly during the activities. The project activities could have also resulted in the patients reaching the health facilities on their own and therefore it was imperative to measure the project effects at the TU level. The annual reports of the project activities are available online [24].
2.3. Study Design, Period, and Population
In this study involving an ecological design (with TU as the study unit), we assessed the relative change in TB CNRs within the Axshya TUs (n = 36) when compared with the non-Axshya TUs (n = 7). We analyzed quarterly TU-level aggregate data in all the 43 TUs under the 15 Axshya districts in the state of Jharkhand (Figure 1) over 16 time periods from quarter 1 (Jan–Mar) 2012 to quarter 4 (Oct–Dec) 2015. The baseline period was from quarter 1 (Jan–Mar) 2012 to quarter 1 (Jan–Mar) 2013 in both Axshya and non-Axshya TUs.
2.4. Variables, Source of Data, and Data Collection
Source of data was the published RNTCP quarterly performance reports. The following variables were collected quarter-wise in long form in an Excel (Microsoft, Redmond, WA, USA) sheet: district name; name of TU; unique identifier of TU (serial number 1–43); Axshya implementation status of TU; quarter of the year (first, second, third, or fourth); time period (1–16); number of patients with presumptive TB examined for sputum microscopy; number of new sputum-positive TB; number of sputum-positive TB; number of all forms of TB; and population of the TU. The number of new sputum-positive TB, sputum-positive TB, and all forms of TB included patients who were registered under the program (at TU) for treatment. Sputum-positive TB included ‘new’ as well as ‘previously treated’ TB. All forms of TB included sputum-positive pulmonary, sputum-negative pulmonary, and extrapulmonary TB (new and ‘previously treated’) [26].
Axshya implementation status at the level of TU was collected in the form of two variables: group and groupFin. The group variable indicated implementation status of the project in the TU for the specific time period/quarter. It was entered as ‘no implementation’ (variable value equal to zero) through all the time periods in the seven non-Axshya TUs and through the first five time periods (starting Jan–Mar 2012) in all the 43 TUs. In the 36 Axshya TUs, group was recorded as ‘implementation’ (variable value equal to one) based on the time period from when they were included under phase II. Although phase II of the project Axshya completed in quarter 3 (Jul–Sep) of 2015, we categorized quarter 4 (Oct–Dec) of 2015 in 36 Axshya TUs as ‘implementation’ because project Axshya continued into the next phase starting October 2015 with a largely similar set of activities (Figure 2).
Under groupFin variable, the 7 non-Axshya TUs and 36 Axshya TUs were entered as ‘no implementation’ (variable value equal to zero) and ‘implementation’ (variable value equal to one), respectively, throughout the 16 time periods.
2.5. Data Analysis
Data were imported into and analyzed using Stata (StataCorp. 2011. Stata Statistical Software: Release 12, College Station, TX: StataCorp LP). Four TB indicators were derived for each time period in each TU as presumptive TB sputum examination rate, new sputum-positive TB CNR, sputum-positive TB CNR, and all forms TB CNR (quarterly, non-annualized, per 100,000 population). These are the standard indicators reported by the program. Year-wise (2012–2015) population-weighted mean quarterly indicators (non-annualized) for Axshya (n = 36) and non-Axshya TUs (n = 7) (based on the variable groupFin) were calculated (S1 Annex).
We fitted a multilevel model for each TB indicator (mixed-effects maximum likelihood regression using random intercept model) for assessing the relative change in TB indicator after the implementation of project activities (S1 Annex) [27].
β2 coefficient [95% confidence interval (CI)] was our key parameter of interest and it indicated the within-TU effect of phase II of project Axshya after adjusting for (a) secular trends; (b) seasonal trends; (c) the baseline differences between the TUs where Axshya was implemented/not implemented (variable groupFin); (d) the differences in the population size of the TUs; and (e) clustering at district level and at TU level (repeat measurements) [27]. The multilevel model parameters did not significantly improve (assessed using likelihood ratio (LR) test) when we added an interaction term between the variables group and ‘TU population in 100,000’ to the above model (group#TU population in 100,000).
We performed a Hausman endogeneity test and retained the random intercept model because the Hausman test was non-significant (p > 0.05) for all the models except the one involving presumptive TB examination rate [27]. Despite this, we eventually decided to retain the random intercept model (instead of fixed effects) involving presumptive TB sputum examination rate as we were dealing with a large number of TUs (n = 43) (belonging to 15 districts) measured over 16 time periods.
2.6. Ethics
Ethics approval was obtained from the Ethics Advisory Group (EAG) of International Union Against Tuberculosis and Lung Disease (The Union), Paris, France (EAG number 15/15, dated 28 September 2015).
3. RESULTS
Between 2012 and 2015, there were 688 (43 TUs*16 time periods) TU-time periods. Of the 396 (36 TUs*11 time periods) TU-time periods between quarter 2 of 2013 and quarter 4 of 2015 in Axshya TUs, there were 369 TU-time periods when phase II of project was implemented (Figure 2).
3.1. Trends in TB Indicators from 2012 to 2015
The gross trends of various TB indicators are depicted in Figure 3.

Trends of mean quarterly TB indicators at the TB unit (TU) level, stratified by phase II Axshya implementation (eventual implementation status), Jharkhand, India, 2012–15*.
*Population-weighted mean rates. *Of the 15 districts under phase II project Axshya in the state, there were 43 TUs. Seven TUs were not covered under the project throughout (non-Axshya TUs). Among Axshya TUs, inclusion of TUs under the project began in Apr–Jun 2013 and eventually all 36 TUs were included by Jul–Sep 2014.
3.1.1. Presumptive TB sputum examination rate
Overall, the mean quarterly rate was lower in Axshya TUs than non-Axshya TUs (variable groupFin) at baseline (115 vs 123 per 100,000 population). During 2013–14, as the Axshya TUs were getting included under the project, the rate increased in both and was higher in Axshya TUs compared with non-Axshya TUs (131 vs 128 per 100,000 population). In 2015, the rate in Axshya TUs was again lower than the non-Axshya TUs.
3.1.2. New sputum-positive TB CNR and sputum-positive TB CNR
There was a difference in mean quarterly rate at baseline (2012) that continued into 2015 and was consistently higher in Axshya TUs. However, the decline seen in non-Axshya TUs was higher than that seen in Axshya TUs (variable groupFin) during 2013–15.
3.1.3. All forms TB CNR
At baseline (2012), the mean quarterly rate was higher in non-Axshya TUs, they crossed over in 2013 and the rate was higher in Axshya TUs than in non-Axshya TUs in 2014 and 2015.
3.2. Impact of Project
Multilevel modelling indicated that there was a significant change in the presumptive TB sputum examination rate, new sputum-positive TB CNR, sputum-positive TB CNR, and all forms TB CNR by 12 (95% CI: 5.5, 18.5), 1.1 (95% CI: 0.5, 1.7), 1.3 (95% CI: 0.6, 2.0), and 1.2 (95% CI: 0.1, 2.2) per 100,000 population per quarter, respectively, before and after implementing Axshya activities (β2 coefficient). There was a decrease in indicators with time as well as with increasing population of the TU (Table 4).
| TB indicator | β coefficient (95% CI) | p-value |
|---|---|---|
| Presumptive TB sputum examination rate | ||
| Axshya – between TUs (groupFin) | −13.51 (−39.31, 12.30) | 0.31 |
| Axshya within TUs (group) | 12.00 (5.53, 18.47) | <0.01*** |
| Time** | 0.42 (−0.20, 1.04) | 0.18 |
| Quarter (Ref: Jan–Mar) | ||
| • Apr–Jun | 3.78 (−1.43, 9.00) | 0.16 |
| • Jul–Sep | 4.70 (−0.55, 9.94) | 0.08 |
| • Oct–Dec | −10.37 (−15.70, −5.05) | <0.01*** |
| TU population in 100,000 | −4.14 (−7.17, −1.10) | <0.01*** |
| Constant | 146.80 (116.35, 177.25) | <0.01 |
| New sputum-positive TB case notification rate | ||
| Axshya – between TUs (groupFin) | 0.83 (−1.33, 2.99) | 0.45 |
| Axshya within TUs (group) | 1.12 (0.50, 1.74) | <0.01*** |
| Time** | −0.14 (10.20, −0.08) | <0.01*** |
| Quarter (Ref: Jan–Mar) | ||
| • Apr–Jun | 2.17 (1.67, 2.67) | <0.01*** |
| • Jul–Sep | 1.24 (0.74, 1.75) | <0.01*** |
| • Oct–Dec | −0.84 (−1.35, −0.33) | <0.01*** |
| TU population in 100,000 | −0.65 (−0.94, −0.36) | <0.01*** |
| Constant | 16.23 (13.41, 19.05) | <0.01 |
| Sputum-positive TB case notification rate | ||
| Axshya – between TUs (groupFin) | 0.61 (−1.87, 3.10) | 0.63 |
| Axshya within TUs (group) | 1.29 (0.63, 1.96) | <0.01*** |
| Time** | −0.16 (−0.23, −0.10) | <0.01*** |
| Quarter (Ref: Jan–Mar) | ||
| • Apr–Jun | 2.43 (1.89, 2.96) | <0.01*** |
| • Jul–Sep | 1.54 (1.00, 2.08) | <0.01*** |
| • Oct–Dec | −0.96 (−1.50, −0.41) | <0.01*** |
| TU population in 100,000 | −0.79 (−1.10, −0.48) | <0.01*** |
| Constant | 19.02 (15.93, 22.13) | <0.01 |
| All forms TB case notification rate | ||
| Axshya – between TUs (groupFin) | −4.71 (−9.95, 0.53) | 0.08 |
| Axshya within TUs (group) | 1.15 (0.11, 2.20) | 0.03*** |
| Time** | −0.20 (−0.30, −0.10) | <0.01*** |
| Quarter (Ref: Jan–Mar) | ||
| • Apr–Jun | 4.21 (3.37, 5.05) | <0.01*** |
| • Jul–Sep | 3.15 (2.31, 4.00) | <0.01*** |
| • Oct–Dec | −1.31 (−2.17, −0.45) | <0.01*** |
| TU population in 100,000 | −1.32 (−1.84, −0.80) | <0.01*** |
| Constant | 37.12 (30.62, 43.63) | <0.01 |
Mixed-effects ML regression using random intercept model (random intercept for district and TU); *Indicators were non-annualized per 100, 000 population per quarter at TU level; *Of the 15 districts under phase II project Axshya in the state, there were 43 TUs. Seven TUs were not covered under the project throughout (non-Axshya TUs). Among Axshya TUs, inclusion of TUs under the project began in Apr–Jun 2013 and eventually all 36 TUs were included by Jul–Sep 2014; *TB indicators in the 43 TUs during 2012 (all TUs were non-Axshya) were also included in the analysis.
TB indicators and Axshya implementation status were measured across 16 time points between 2012 and 2015 (each quarter was one time point).
Statistically significant.
Impact of phase II of project Axshya on TB indicators at TB unit (TU) level after adjusting for baseline differences, time and clustering effect of district and TU (repeated measures within TU), Jharkhand, India (2013–15)*
By multiplying the β2 coefficients with 369 TU-time periods for which the project was implemented (average TU size of 500,000), the estimated number (95% CI) of sputum examinations, new sputum-positive TB, sputum-positive TB, and all forms of TB attributable to phase II of the project were 22,410 (10,203, 34,077), 2066 (923, 3210), 2380 (1162, 3616), and 2122 (203, 4059), respectively.
4. DISCUSSION
This is the first state-wide study from India to document the impact of a large-scale ACSM and ACF TB project on TB case finding indicators in program setting. The relatively robust methodology was as per international recommendations [13,27]. In a setting with an overall decreasing trend of case finding indicators, project Axshya resulted in an increase in presumptive TB sputum examination rate and TB CNRs in Axshya TUs when compared with PCF after adjusting for the secular and seasonal trends and baseline differences in indicators between Axshya and non-Axshya TUs.
During 2013–14 when the Axshya TUs were being included in the project (Table 2), either the gap between Axshya and non-Axshya TUs increased (with Axshya TUs trend line being consistently higher) or the gap reduced with the trend lines crossing over (with Axshya TUs having a lower baseline indicator in 2012) (Figure 3). In other words, when compared with TUs where the project was not implemented (PCF), project Axshya appeared to result in a relative increase in all the TB indicators. This was confirmed in the multilevel modelling where when compared with PCF, project Axshya resulted in a significant increase (significant ‘within’ effect) in all four TB indicators. The findings are consistent with a Cochrane review (2017) involving controlled trials (randomized/non-randomized), which suggests that active/enhanced case-finding approaches may result in increase in TB patient detection in the short term [28].
The activities under the project were limited to the marginalized and vulnerable populations of Axshya TUs. Therefore, not all DMCs under the Axshya TUs were covered. Within a DMC as well, it was not mandatory that the whole population would have been covered. In addition, the project also provided technical support at the state level that may have its effect on non-Axshya TUs. Implementation of any activity at the field level was sufficient for the variable group to be entered as ‘implementation’. In addition, activities conducted in one TU may spillover to the adjacent TU and, therefore, the results could get biased toward the null. For these reasons, the estimates provided in our study are conservative and the true impact could be higher.
We believe that the project Axshya activities resulted in changes in the case finding indicators as a result of its effect on presumptive TB sputum examination rate that could be attributed largely to two activities under the project: Axshya SAMVAD and SCT (Table 3). This in turn could have resulted in higher diagnosis of sputum-positive TB (new and previously treated) and sputum-negative TB leading to a relative increase in all forms of TB CNR as well.
There were many studies that were without a control arm, unlike our study [29–31]. Hence, they were not in a position to conclusively determine the effect of the TB screening strategy [15]. Two studies had control arms. First, in a study from Cambodia (2016), a retrospective household and neighborhood contact investigation along with cartridge-based nucleic acid amplification test resulted in increased patient detection during the intervention (2-year period), which was followed by decrease after the intervention. Sustained impact on TB epidemiology was not studied, similar to our study [32]. Second, the Zambia South Africa TB and HIV reduction (ZAMSTAR) study was a community-randomized trial done in Zambia and the Western Cape province of South Africa. There were two interventions: community-level enhanced TB case finding and household level TB–HIV care, which was followed by a prevalence survey for impact on TB epidemiology. Neither intervention led to a statistically significant reduction in TB [33].
4.1. Implications for India’s National TB Program
There are three major implications of our study. First, on the basis of our study and two studies conducted elsewhere in other countries [32,33], it appears that whether the activities under project Axshya will have an effect on the case finding indicators in other states/districts of the country will depend upon the size of the high-risk populations in relation to the overall population of the TU/district, the TB burden in the high-risk population, their previous health-seeking behavior (particularly what proportion of TB patients were being diagnosed and treated under the program prior to implementing ACSM activities), coverage of the high-risk populations by the ACSM activities, effectiveness of ACSM activities implemented, the short- and long-term changes introduced by the ASCM activities in changing this behavior, the diagnostic tools used, changes in the health system-related factors, and so on. We have not measured and do not have an estimate on many of these factors and, therefore, the true effect of the impact of the project activities in any given context elsewhere will depend on the magnitude and distribution of these factors.
Second, detection of large numbers of patients was attributed to the project. These patients would have either been managed in the private sector (and not been notified to RNTCP) or remained undiagnosed and died, or diagnosed with delay within RNTCP after 2015 with associated morbidity and mortality. Whether these numbers are worth the investment, this requires further cost-effective analysis.
Third, India’s technical and operational guidelines (2016) have also recommended systematic ACF over and above the existing PCF strategies under RNTCP [21]. The program has decided to scale-up ACF to all the districts as per the national strategic plan to eliminate TB (2017–25). Our study findings support these national level decisions [34]. This is essential as India gears up to attain the target of ending TB by 2025, 5 years before the global target of 2030 as per the sustainable development goals [34,35].
4.2. Future Research
Future research should focus on continued documentation of TU-level indicators over a longer period (say till 2023) to document the impact on TB epidemiology [13,15]. This analysis should adjust for other TU-level factors. The next phase of project Axshya (after 2015) will provide that opportunity. A detailed cost-effectiveness analysis of the project in the state is also recommended.
4.3. Strengths
There were many strengths in our study. First, availability of non-Axshya TUs during the intervention (2013–15) in Axshya districts and information on exact time period when an Axshya TU was included in the project allowed for a comparison. We chose TUs within Axshya districts only as control TUs and did not include TUs in non-Axshya district. Therefore, district-level factors (if any) were likely to affect both types of TU within the district equally. Second, availability of indicators in the TUs for five pre-intervention time periods [quarter 1 (Jan–Mar) 2012 to quarter 1 (Jan–Mar) 2013] allowed for adjustment for secular trends and baseline differences between TUs. These baseline differences were because the TUs were not randomly selected. Third, we also provided estimates for the effect of the project that were adjusted for clustering and population size of a TU. Fourth, data on TB indicators for each and every quarter across all TUs were included in analysis. Therefore, the analysis was more rigorous and robust than a before and during analysis with a comparison arm. Since all TUs in the Axshya districts were included, there was no sampling bias. To the best of our knowledge, they were not any other extraneous factors that were differentially introduced in Axshya TUs.
4.4. Limitations
However, there are some limitations. First, we have studied the impact of the intervention within program settings and could have missed patients who were receiving treatment in the private sector. Second, we did not have sufficiently long follow-up periods, say 10 years, to document the impact of the project, or the lack of impact, on TB epidemiology in long run (reduction in CNRs) [13,15]. Third, there were other factors at TU level that may affect the indicators but these were not collected. Data on the level of implementation of the project at TU level was not available and this would have established the dose–response relationship. This information was available for each activity under the project at the level of district and not at the level of TU in the quarterly progress reports of the project. Finally, as this is an ecological design, ecological fallacy cannot be ruled out.
4.5. Conclusion
Project Axshya activities in marginalized/vulnerable populations had an impact on increasing the presumptive TB sputum examination rate, new sputum-positive TB CNR, sputum-positive TB CNR, and all forms TB CNR at the subdistrict level TUs over a period of 3 years (2013–15) when compared with PCF in Jharkhand, India. This was despite the project being limited to the marginalized and vulnerable populations of Axshya TUs. This calls for sustaining and scaling up the project activities in other similar districts in the state and elsewhere in the country.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHOR CONTRIBUTIONS
H.D.S., V.G., S.M., R.R., B.M.P., A.M.V.K. and S.S.C. were involved in conception and design of the study; H.D.S., V.H.G., S.N., M.B., S.S., K.K.R., G.M., O.P.B., P.P., S.M. and S.P. were involved in data collection; H.D.S., V.G., S.S., A.M.V.K., S.S.C., R.D. and R.R. were involved in data analysis/interpretation; H.D.S. prepared the first draft; all authors revised it critically for important intellectual content and approved the final version to be published. V.G., V.H.G. and S.N. contributed equally as second authors; A.M.V.K. and S.S.C. contributed equally as senior authors.
FUNDING
Project Axshya is being implemented by The Union South-East Asia and is supported by The Global Fund. This study did not require separate budget as it was conducted under the project conditions using project staff.
ACKNOWLEDGMENTS
The authors sincerely acknowledge the contribution of subrecipients of Project Axshya for the implementation of project Axshya in Jharkhand, India: Population Services International (PSI), India; The Catholic Health Association of India (CHAI); and Emanuel Hospital Association (EHA) and the staff from project management unit, The Union South-East Asia Office for the supervision of the implementation (Anand Das, currently MDR-TB and HIV specialist, Ministry of Health, Timor Leste and ER Babu, currently working as Senior Manager, Plan International: India Chapter). We thank all the District Coordinators and Interpersonal Communication Coordinator of Project Axshya that were involved in implementation of the project in 15 Axshya districts during 2013–15. We also acknowledge the support received from Liji Mohandas, The Union South-East Asia Office, in coordinating the meeting of project staff for data extraction. We thank the Department for International Development (DFID), UK, for funding the Global Operational Research Fellowship Programme at the International Union Against Tuberculosis and Lung Disease (The Union), Paris, France in which Hemant Deepak Shewade works as a senior operational research fellow.
ABBREVIATIONS
- TB,
tuberculosis;
- RNTCP,
Revised National Tuberculosis Control Programme;
- ACF,
active case finding;
- ACSM,
advocacy, communication and social mobilization;
- PCF,
passive case finding;
- The Union,
International Union Against Tuberculosis and Lung Disease;
- SAMVAD,
sensitization and advocacy in marginalised and vulnerable areas of the district;
- CNR,
case notification rate;
- TU,
tuberculosis unit;
- DMC,
designated microscopy center;
- SCT,
sputum collection and transport;
- CI,
confidence interval.
DISCLAIMER
The contents of this paper do not necessarily reflect the views of the Government or non-governmental organizations or The Union.
RESEARCH DATA
Dataset (Stata and MS Excel format) and program file (Stata DO file) used for analysis (S1 Annex) have been provided as supplementary material and can be accessed using this link https://doi.org/10.6084/m9.figshare.c.4465757. These are available under the terms of the Creative Commons Zero “No rights reserved” data waiver (CC0 1.0 Public domain dedication). The program file contains the commands for calculation of population-weighted mean TB indicators and commands related to multilevel model development.
REFERENCES
Cite this article
TY - JOUR AU - Hemant Deepak Shewade AU - Vivek Gupta AU - Vaibhav Haribhau Ghule AU - Sashikanta Nayak AU - Srinath Satyanarayana AU - Rakesh Dayal AU - Subrat Mohanty AU - Sukhwinder Singh AU - Moumita Biswas AU - Kiran Kumar Reddy AU - Gayadhar Mallick AU - Om Prakash Bera AU - Prabhat Pandey AU - Sripriya Pandurangan AU - Raghuram Rao AU - Banuru Muralidhara Prasad AU - Ajay Madhugiri Venkatachalaiah Kumar AU - Sarabjit Singh Chadha PY - 2019 DA - 2019/09/06 TI - Impact of Advocacy, Communication, Social Mobilization and Active Case Finding on TB Notification in Jharkhand, India JO - Journal of Epidemiology and Global Health SP - 233 EP - 242 VL - 9 IS - 4 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.190812.002 DO - 10.2991/jegh.k.190812.002 ID - Shewade2019 ER -