
Predictors of Quality of Life in Transfusion-dependent Thalassemia Patients Based on the PRECEDE Model: A Structural Equation Modeling Approach
- DOI
- 10.2991/jegh.k.191001.001How to use a DOI?
- Keywords
- Quality of life; transfusion-dependent thalassemia; PRECEDE model
- Abstract
This study aimed to determine the predictors of Quality of Life (QoL) in Transfusion-Dependent Thalassemia (TDT) patients based on PRECEDE (Predisposing, Reinforcing and Enabling Constructs in Educational Diagnosis and Evaluation) model. This cross-sectional analytical study was performed on 389 TDT patients who were under treatment in four thalassemia centers in Tehran, Iran. Data gathering instrument consisted of three parts: socioeconomic and demographic information, the Persian version of the six standardized questionnaires for measuring some of the potential predictive factors of QoL in TDT patients based on the PRECEDE model constructs, and a researcher-made questionnaire to assess knowledge of patients about health- and QoL-promoting behaviors and enabling factors involved in health- and QoL-promoting behaviors. Using AMOS 23.0, the structural equation modeling with maximum likelihood estimation was conducted to test the proposed hypotheses. Associations of QoL with all of the PRECEDE model constructs, including anxiety–depression, self-efficacy, perceived barriers, knowledge, enabling factors, and reinforcing factors were significant (all p < 0.001). Anxiety–depression and perceived barriers were the significant negative predictors of QoL in TDT patients, whereas health-promoting lifestyle was the significant positive predictor of QoL in TDT patients. The final conceptual model of the study was adequately fit and can be applied as a framework for future educational-supportive programs aimed at improving the QoL in TDT patients.
- Copyright
- © 2019 Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Thalassemia is the most common hereditary chronic anemia disorders in the world [1], and it has become a major global concern because it affects life expectancy and Quality of Life (QoL) of 100s of 1000s of individuals across the globe [1]. Owing to the chronic condition of the disease, Transfusion-dependent Thalassemia (TDT) patients might deal with a variety of complications such as heart failure, arrhythmia, diabetes, hypogonadism, hypothyroidism, HIV infection, and thrombosis [2] that might affect their QoL. Significant advances in treatment modalities and improved clinical management have led to a substantially higher life expectancy of these patients [2–4]; thus, the need for improvement in QoL remains a major responsibility of the health care providers and policymakers. The effects of thalassemia disease on QoL are not well evaluated [5]. Considering the improved survival rates in TDT patients [2,6], and with regard to the importance of QoL improvement as a core target of healthcare provision, closer attention should be paid to the careful investigation of factors affecting QoL in these patients.
Identifying factors affecting QoL in TDT patients can help health educators and health care providers to develop and conduct better psychosocial support and counseling programs as well as clinical interventions to improve treatment outcomes in these patients [7]. The effectiveness of health education programs predominantly depends on the choice of appropriate health behavior theories and models because they give us a clear concept of strategies and intervention objectives [8]. Therefore, having a model as a conceptual framework to identify factors affecting QoL in TDT patients is an advantage.
1.1. Conceptual Framework
PRECEDE is an acronym for Predisposing, Reinforcing and Enabling Constructs in Educational Diagnosis and Evaluation. PRECEDE is a useful and cost–benefit model proposed by Lawrence Green that determines various factors, particularly behavioral factors that affect QoL. This model provides a framework for exploring factors influencing behaviors, including predisposing factors, reinforcing factors, and enabling factors [9]. Predisposing factors are defined as factors that exert their effects before a behavior occurs. Indeed, they influence an individual’s motivation to undertake that particular behavior [10]. The predisposing factors within the scope of this research were anxiety–depression, perceived self-efficacy, perceived barriers, and knowledge. Reinforcing factors refer to factors that reward or strengthen the desired behavior [10]. The reinforcing factors within the scope of this research were social supports from family members, friends, and significant others. Enabling factors are resources and skills that facilitate health behavior change [10]. The enabling factors within the scope of this research were the degree of availability and accessibility of resources and services for TDT patients.
Predisposing, reinforcing and enabling constructs in educational diagnosis and evaluation model is one of the widely used models for designing and evaluating health education programs [10]. The model is a suitable choice for clinical trials [11], behavior change interventions [12], and QoL interventions among patients with chronic diseases [13]. So far, no study has sought to examine the correlates and predictors of QoL in TDT patients using a valid and practical model. In this study, using the structural equation modeling approach, we aimed to identify the predictors of QoL in TDT patients based on the constructs of the PRECEDE model.
1.2. Study Hypotheses
Hypotheses 1–4: Predisposing factors (H1), reinforcing factors (H2), enabling factors (H3), and Health-Promoting Lifestyle (HPL) (H4) affect QoL in TDT patients.
Hypotheses 5–7: Predisposing factors (H5), reinforcing factors (H6), and enabling factors (H7) affect QoL in TDT patients through a mediating role of HPL.
1.3. Study Variables
Independent variables or exogenous latent variables: predisposing factors, enabling factors, and reinforcing factors.
Mediating variable: HPL.
Dependent variable or endogenous latent variable: QoL.
1.4. Definitions of the Study Variables
Exogenous variable: A variable that is not affected by the other variables in the model.
Endogenous variable: A variable that is changed or determined by its relationship with other variables in the model.
Manifest variable: A variable that can be directly measured or observed.
Latent variable: A variable that cannot be directly measured or observed.
Mediating variable: A mediating variable can be seen as both independent and dependent variables; however, it is considered as an endogenous latent variable in the Structural Equation Modeling (SEM).
2. MATERIALS AND METHODS
In this cross-sectional investigation, we studied 389 TDT patients who were under treatment in four major thalassemia centers in Tehran, Iran. The centers under study were affiliated with the Iran University of Medical Sciences, Tehran University of Medical Sciences, and Iranian Blood Transfusion Organization. The total number of TDT patients over 18 years who had medical records in the mentioned centers was 651 patients (according to the Iranian Ministry of Health data, 2015). The sampling method was stratified random sampling. Out of the nine thalassemia centers, we identified centers with more than 50 TDT patients as strata.
Four centers, including Zafar Adult Thalassemia Clinic with 288 patients, Baharloo Hospital with 54 patients, Ali Asghar Children’s Hospital with 70 patients, and Children’s Medical Center Hospital with 103 patients were included in the study. Then, proportional to the number of patients at each center, the required samples were selected using simple random sampling. Ethical approval for this study was obtained from the Tehran University of Medical Sciences (IR.TUMS.REC.1394.1153) and informed consent was received from all patients. Note that participating in the study was not an extra burden on patients, and they participated in the study during their routine medical visits or chelation therapy.
2.1. Measures
The survey instrument consisted of three parts: The first part contained information on socioeconomic and demographic characteristics, including age, gender, marital status, level of education, and employment status. The second part included the Persian version of the following standardized questionnaires:
12-Item Short-Form Health Survey (SF-12) [14]: This is a shorter alternative of the 36-item Short-Form Health Survey. The questionnaire measures the physical and mental condition of the respondent using 12 items. The raw score for each item ranges from 1 to 6. Scores on some items should be recoded and then will be transformed into a 0 to 100-point scale. The higher the score, the better the QoL [15].
Health-Promoting Lifestyle Profile [16]: The questionnaire measures six dimensions of HPL (nutrition, physical activity, health responsibility, stress management, interpersonal relations, and spiritual growth) through 52 items. Each item is given a response on a 4-point Likert Scale (from never to routinely). The overall possible score ranges from 52 to 208, with higher scores indicating better HPL [17].
Hospital Anxiety and Depression Scale [18]: The questionnaire contains 14 items and measures two subscales of anxiety and depression on a 4-point Likert Scale (0–3 points). The overall 21 scores can be awarded for each subscale. Scores 0–7 represent normal status, 8–10 mirror a borderline abnormality, and 11–21 represent severe anxiety and depression [19].
Multidimensional Scale of Perceived Social Support [20]: The scale contains 12 items to measure perceived social support from family members, friends, and significant others. Each item is rated on a 5-point Likert Scale (from quite agree to quite disagree), with higher scores indicating receipt of greater support from family members, friends, and significant others [21].
Perceived Health Competence Scale [22]: The questionnaire includes eight items to measure self-efficacy in the respondent. Items are rated on a 5-point Likert Scale (from I strongly agree to I strongly disagree), with higher scores indicating individual’s capability to effectively control and manage his or her health outcomes [23].
Barriers to Health Promoting Activities for Disabled Persons Scale [22]: The questionnaire contains 18 items that measure perceived barriers to health-promoting behaviors. Items are rated on a 4-point Likert Scale (from never to routinely), with higher scores reflecting greater perceived barriers in individual [24].
The third part of the survey instrument was a researcher-made questionnaire to assess knowledge of patients about health- and QoL-promoting behaviors and enabling factors involved in health- and QoL-promoting behaviors.
Patients’ knowledge about different aspects of a healthy lifestyle, the importance of a healthy lifestyle, and factors influencing QoL improvement in TDT patients was measured using 12 items. Each correct answer received one point, whereas each wrong or I do not know answer received zero points. The enabling factors (access to resources, skills, and tension-reduction factor) were measured using eight items with three categories (yes, somewhat, no). The range of possible scores was from 0 to 16, with higher scores indicating a patient’s higher access to enabling factors. The content validity of the researcher-made questionnaire was checked by five faculty members who were health education and promotion specialists, and five physicians with at least 2 years of work experience in thalassemia centers. The reliability of the questionnaire was measured through internal consistency reliability and test–retest method. Thirty patients were asked to fill out the questionnaires twice with a 2-week interval.
The Cronbach’s alpha values of the overall knowledge scale and enabling factor scale were 0.79 and 0.74, respectively. The intraclass correlation coefficients of the overall knowledge scale and enabling factor scale were 0.89 (95% confidence interval, range 0.65–0.93) and 0.82 (95% confidence interval, range 0.60–0.92), respectively.
2.2. Data Analyses
Data were entered into SPSS version 23 (IBM Corp., Armonk, NY, USA), and descriptive statistics (mean, standard deviation, frequency, and percentage) were used to describe the socioeconomic and demographic characteristics of the participants. The Pearson correlation coefficient was used to determine the correlation between the independent and dependent variables. Using AMOS 23.0 (IBM Corp., Armonk, NY, USA), the SEM with maximum likelihood estimation was conducted to test the proposed hypotheses.
Structural equation modeling includes a series of statistical methods and mathematical models that specify the causal relationship between one or more independent variables and one or more dependent variables by combining the measurement model and structural model [25]. Whereas the measurement model explains the relationship between latent variables and manifest variables, the structural model illustrates the direct and indirect effects of the latent variables (exogenous and endogenous latent variables) on each other [25]. In the current study, the relationship between some of the potential factors affecting QoL was analyzed in two steps. In the first step, the relationship between the latent variables and manifest variables was analyzed using the factor loadings. Factor loading is a correlation coefficient between latent variables and their related manifest variables. Consistent with experts’ recommendations, we excluded the manifest variables with factor loadings of <0.5 from the model [26,27]. There is no consensus among experts concerning which of the goodness-of-fit indices better represent the goodness-of-fit of the model. However, they recommend reporting three to four indices [28,29]. In this study, the Comparative Fit Index (CFI), Root Mean Square Error of Approximation (RMSEA), Goodness-of-Fit Index (GFI), and Adjusted Goodness-of-Fit Index (AGFI) were used. The model was considered to have an acceptable fit if CFI > 0.9, RMSEA < 0.08, GFI > 0.8, and AGFI > 0.8 [30,31]. The structural model was evaluated by testing the significance of all direct and indirect effects specified in the model to determine whether the independent variables (exogenous latent variables) and mediating variable have direct and indirect effects on the dependent variable (endogenous latent variable). The R2 value was used to estimate the percentage of variance in the dependent variable explained by independent variables and the mediating variable. A p-value of <0.05 was considered to indicate statistical significance.
3. RESULTS
3.1. Description of the Study Variables
The mean age of the patients was 30.2 ± 8.3 years. Almost half of the patients (46.0%) were male, and the majority (67.1%) were single. The demographic characteristics of the patients are indicated in Table 1. The mean and standard deviation of the scores of QoL, HPL, anxiety–depression, self-efficacy, perceived barriers, knowledge, enabling factors, and reinforcing factors are listed in Table 2.
| Variables | Sub-variables | Number (%) |
|---|---|---|
| Thalassemia center | Children’s Medical Center Hospital | 78 (20.1) |
| Ali Asghar Children’s Hospital | 53 (13.6) | |
| Zafar Adult Thalassemia Clinic | 218 (56.0) | |
| Baharloo Hospital | 40 (10.3) | |
| Gender | Male | 179 (46.0) |
| Female | 210 (54.0) | |
| Marital status | Single | 261 (67.1) |
| Married | 128 (32.9) | |
| Level of education | Illiterate | 5 (1.3) |
| No high school diploma | 51 (13.1) | |
| High school diploma | 171 (44.0) | |
| University degree | 162 (41.6) | |
| Occupational status | Housewife | 60 (15.4) |
| High school student | 11 (2.8) | |
| University student | 44 (11.3) | |
| Civil servant | 33 (8.5) | |
| Self-employed | 167 (42.9) | |
| Unemployed | 74 (19.0) | |
| Total | 389 |
Demographic characteristics of the patients (N = 389)
| Variables | Mean ± SD | Scale rangea | Min–Maxb |
|---|---|---|---|
| QoL | 61.44 ± 23.38 | 0–100 | 2.08–100 |
| HPL | 2.44 ± 0.41 | 1–4 | 1.35–3.94 |
| Anxiety–depression | 1.06 ± 0.47 | 0–3 | 0.07–2.71 |
| Self-efficacy | 3.5 ± 0.61 | 1–5 | 1.75–5 |
| Perceived barriers | 2.08 ± 0.53 | 1–4 | 1–4 |
| Knowledge | 0.73 ± 0.18 | 0–1 | 0–1 |
| Enabling factors | 0.80 ± 0.36 | 0–2 | 0–2 |
| Reinforcing factors | 3.48 ± 0.72 | 1–5 | 1–5 |
The lowest and highest values that can be obtained from the original scale.
The lowest and highest values that were obtained in this study.
QoL, quality of life; HPL, health-promoting lifestyle; SD, standard deviation; Min: minimum; Max: maximum.
The mean and standard deviation of independent and dependent variables (N = 389)
3.2. Correlations
Associations of QoL with all of the PRECEDE model constructs, including anxiety–depression, self-efficacy, perceived barriers, knowledge, enabling factors, and reinforcing factors were significant (all p < 0.001) (Table 3).
| Independent variables | R | p-value |
|---|---|---|
| HPL | 0.521 | <0.001 |
| Anxiety–depression | −0.636 | <0.001 |
| Self-efficacy | 0.569 | <0.001 |
| Perceived barriers | −0.605 | <0.001 |
| Knowledge | 0.166 | <0.001 |
| Enabling factors | 0.336 | <0.001 |
| Reinforcing factors | 0.462 | <0.001 |
QoL, quality of life; HPL, health-promoting lifestyle.
Pearson correlation between QoL and independent variables
3.3. Testing the Hypotheses and Final Conceptual Model
Before testing the hypotheses and final conceptual model of the study, the second-order confirmatory factor analysis in SEM was used to test the appropriateness of the measurement model of the independent, mediating, and dependent variables. The final measurement model and the structural model were also examined (Tables 4 and 5). The first-order confirmatory factor analysis was used to examine the validity of the measurement model of the final conceptual model. Table 5 presents the goodness-of-fit values of the overall measurement model. Goodness-of-fit values indicated an adequate fit of the model (Tables 4 and 5). Therefore, the appropriateness of the overall measurement model was confirmed. After ensuring the appropriateness of the overall measurement model, the main hypotheses of the study (the relationship between the latent variables) were tested in the structural model. Table 6 shows the results of the hypothesis testing and direct and indirect effects of the independent variables and mediating variable on the dependent variable.
| Variables | RMSE | CFI | GFI | AGFI |
|---|---|---|---|---|
| Anxiety–depression | ||||
| Initial model | 0.108 | 0.800 | 0.866 | 0.815 |
| Final model | 0.077 | 0.929 | 0.941 | 0.907 |
| Perceived barriers | ||||
| Initial model | 0.085 | 0.881 | 0.876 | 0.838 |
| Final model | 0.070 | 0.926 | 0.910 | 0.872 |
| Knowledge | ||||
| Initial model | 0.083 | 0.706 | 0.833 | 0.794 |
| Final model | 0.066 | 0.927 | 0.944 | 0.907 |
| Enabling factors | ||||
| Initial model | 0.070 | 0.977 | 0.970 | 0.936 |
| Final model | 0.070 | 0.977 | 0.970 | 0.936 |
| Reinforcing factors | ||||
| Initial model | 0.095 | 0.930 | 0.909 | 0.861 |
| Final model | 0.079 | 0.956 | 0.939 | 0.899 |
| HPL | ||||
| Initial model | 0.069 | 0.696 | 0.707 | 0.682 |
| Final model | 0.062 | 0.959 | 0.830 | 0.810 |
| QoL | ||||
| Initial model | 0.113 | 0.862 | 0.871 | 0.811 |
| Final model | 0.073 | 0.949 | 0.940 | 0.900 |
QoL, quality of life; HPL, health-promoting lifestyle; RMSE, root mean square error; CFI, comparative fit index, GFI, goodness-of-fit index; AGFI, adjusted goodness-of-fit index.
The goodness-of-fit values of the measurement model of the independent, mediating and dependent variables
| Variable | RMSE | CFI | GFI | AGFI |
|---|---|---|---|---|
| Perceived barriers | ||||
| Initial model | 0.082 | 0.886 | 0.771 | 0.723 |
| Final model | 0.071 | 0.928 | 0.842 | 0.801 |
RMSE, root mean square error; CFI, comparative fit index, GFI, goodness-of-fit index; AGFI, adjusted goodness-of-fit index.
The goodness-of-fit values of the overall measurement model
| Hypotheses | Direct effect | p-value | Indirect effect | Overall effect | R2 |
|---|---|---|---|---|---|
| Anxiety–depression → QoL | −0.461 | 0.002 | −0.053 | −0.514 | 0.569 |
| Self-efficacy → QoL | 0.036 | 0.641 | 0.082 | 0.119 | |
| Perceived barriers → QoL | −0.181 | 0.035 | −0.001 | −0.182 | |
| Knowledge → QoL | −0.072 | 0.139 | −0.015 | −0.087 | |
| Enabling factors → QoL | 0.029 | 0.368 | 0.023 | 0.052 | |
| Reinforcing factors → QoL | −0.041 | 0.591 | 0.036 | −0.005 | |
| HPL → QoL | 0.212 | 0.010 | 0 | 0.212 |
HPL, health-promoting lifestyle; QoL, quality of life.
Reported values of the predictive factors in the final structural model
Anxiety–depression (β = −0.461, p < 0.002) and perceived barriers (β = −0.181, p < 0.035) had a significant direct negative effect on QoL, whereas HPL (β = 0.212, p < 0.01) had a significant direct positive effect on QoL. Self-efficacy (indirect effect = 0.082), enabling factors (indirect effect = 0.023), and reinforcing factors (indirect effect = 0.036) had a significant indirect positive effect on QoL through HPL (Figure 1). Anxiety–depression had the strongest effect on QoL (total effect = −0.514). Predisposing factors, enabling factors, reinforcing factors, and HPL together explained 57% of the overall variance in QoL (Table 6). R2 values of the model reached an acceptable value (R2 = 0.569) [32].
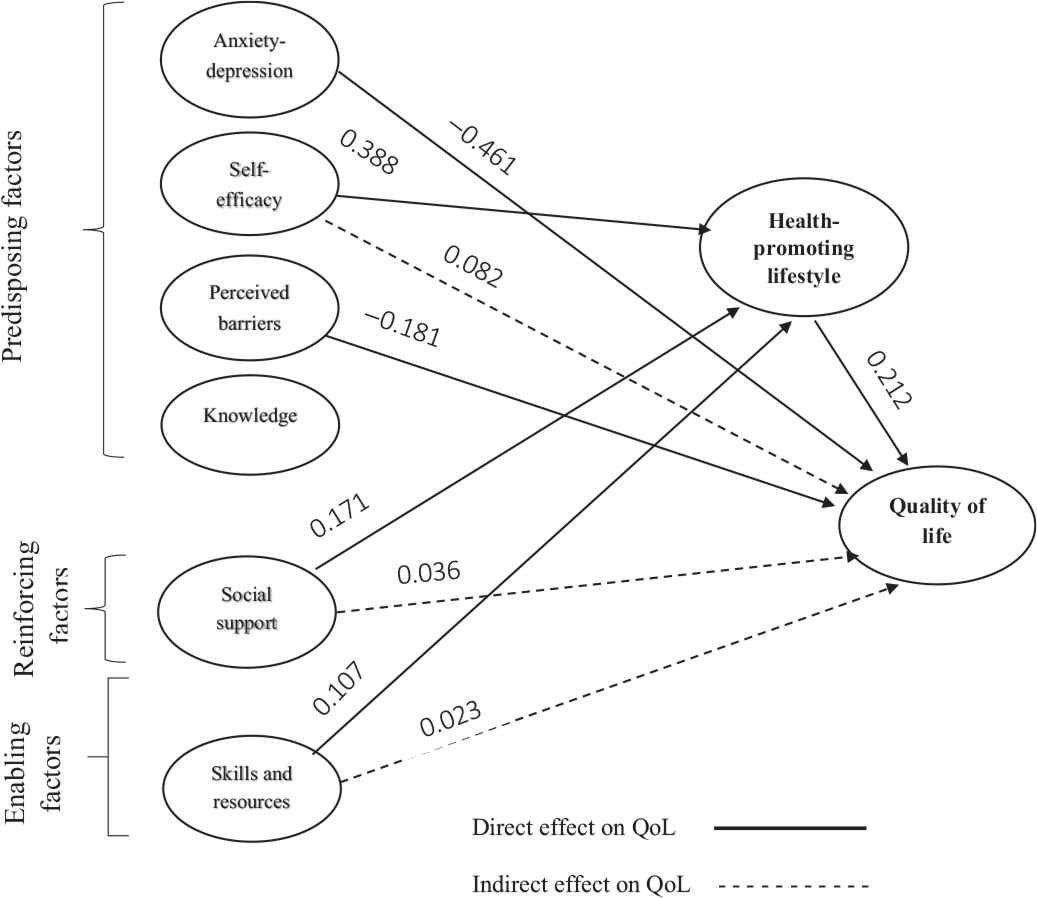
The final conceptual framework of the predictors of QOL in TDT patients based on the constructs of the PRECEDE mode.
4. DISCUSSION
This study sought to identify the predictors of QoL in TDT patients based on the constructs of the PRECEDE model. Results revealed that anxiety–depression, perceived barriers, and HPL were the predictors of QoL in TDT patients. Perceived barriers and anxiety–depression had a significant negative effect on QoL, whereas HPL had a significant positive effect on QoL. Another study has also reported that anxiety–depression negatively affected the physical and mental components of QoL in TDT patients. The higher the anxiety–depression, the lower the QoL [33]. Naturally, anxiety is a temporary condition; however, it is considered a disease when it is extended in the absence of mental pressure or threats [34]. Owing to the chronic nature of thalassemia disease, the prevalence of mental disorders such as anxiety and depression in TDT patients is much higher than that of healthy individuals [35,36]. The high levels of depression and anxiety hurt the social life, and occupational and recreational activities, increase the risk of hospitalization and mortality, and finally affect QoL in TDT patients [33]. Therefore, timely diagnosis and treatment of mental disorders in TDT patients are necessary. Note that the ideas and insights of psychologists and psychiatrists regarding effective interventions would be helpful.
According to the results from this study, perceived barriers were the significant predictive factor for QoL in TDT patients. This finding is in line with that of Han et al. [37]. Perceived barriers include assumptions about an action that is inaccessible, irrelevant, expensive, problematic, and time-consuming. Perceived barriers usually impede health-promoting behaviors and are considered as hurdles, which are one’s belief about actual costs and psychological burden of performing a behavior [38]. Lack of interest, fatigue, lack of money, and transportation problems are common barriers that hinder an individual from undertaking healthy behaviors [24]. Thalassemia patients may attribute daily barriers to the particular condition of the disease. Lack of access to health care services and adherence to the health-promoting behaviors adversely affect QoL in these patients [39,40]. Consequently, health policymakers should pay more attention to reducing barriers that interfere or prohibit access to health facilities. Furthermore, applied educational–behavioral interventions should be implemented to assist thalassemia patients to overcome barriers, particularly personal barriers such as lack of information about health care behaviors, lack of motivation to adhere health-promoting behaviors, and psychosocial distress.
Findings from this study revealed that HPL was a significant predictive factor for QoL in TDT patients. Several studies have reported similar results, indicating the significant positive effect of health-promoting behaviors and HPL on QoL [37,40,41]. Health-promoting behaviors such as health responsibility, physical activity, healthy diet, spiritual growth, good interpersonal relationships, and stress management are known to improve QoL [42]. Lifestyle is a set of routine daily activities that are commonly accepted by individuals and vary from one person to another. Different rates of mortality and morbidity, and the risk of getting diseases are highly associated with lifestyle differences [43]. Lifestyle not only affects the general health status but also the overall QoL of people. The healthier the lifestyle, the better the QoL [42]. Planning different health education and promotion interventions toward the improvement of HPL that promotes health in the patients may lead to a decrease in the development of new disease and death rate in these patients. Through this and along with the increase in life expectancy, the patients can enjoy a better QoL.
The results of this study revealed that self-efficacy, knowledge, enabling factors, and perceived social support were not the predictors of QoL and had no direct effect on QoL in TDT patients. Contrary to our observation, results from a study on chronically ill patients in Korea indicated that social support and self-efficacy were the significant predictive variables of QoL [37]. In addition, Platania et al. [44] also found that self-efficacy had a direct effect on satisfaction with life in TDT patients. A reason behind this inconsistency is not clear; however, the use of different scales and statistical tests, as well as differences in the study population, maybe an explanation for the differences reported. Our findings revealed that knowledge was not a predictor of QoL in TDT patients. As with other patients, thalassemia patients need to have a correct understanding of behaviors that maintain and promote their health. However, knowledge alone may not guarantee QoL-promoting behaviors and along with an increase in knowledge, TDT patients should be provided with the necessary skills and training to tackle psychosocial distress and physical limitations.
Results indicated that enabling factors were not direct predictive factors of QoL in TDT patients; however, they had an indirect effect on QoL through a mediating role of HPL. Therefore, when planning the intervention programs aimed at improving QoL, it is necessary to pay enough attention to enabling factors in the context of HPL to empower patients and assist them in adopting health-promoting behaviors. For instance, health education specialists can improve the QoL of TDT patients by implementing educational classes to teach patients the tension reduction and stress reduction techniques, communication skills, and skills required for adopting a healthier lifestyle. In addition, enabling factors such as easy access to blood transfusion facilities and iron chelation therapies are highly effective factors in improving QoL in TDT patients [45].
According to the findings, reinforcing factors were not direct predictive factors of QoL in TDT patients. Contrary to what we found, a study on 488 cervical cancer patients found that social support was the significant predictor of QoL [40]. Application of different theoretical framework and measurement methods, and scoring system may explain this inconsistency. It is to be noted that in our study, social support had an indirect effect on QoL through a mediating role of HPL. Therefore, it can be concluded that social support alone may not improve the QoL of TDT patients, but it can improve the QoL through HPL. Accordingly, when planning intervention programs, health education experts should pay close attention to the supportive role of the family members and significant others as a primary source of support because they can have a pivotal role in motivating patients to sustain health-promoting behaviors.
5. CONCLUSION
Investigating the factors affecting QoL in TDT patients is a prerequisite of interventions targeted at improving QoL in these patients. We found that anxiety–depression, perceived barriers, and HPL were the significant predictors of QoL in TDT patients. Among them, anxiety–depression had the strongest effect on QoL in participants. As the health care resources (budget, time, and personnel) are limited, health policymakers are advised to allocate resources more efficiently. Therefore, factors having a stronger effect on QoL should be given higher priority in future QoL interventions. In this study, the PRECEDE model could well identify factors affecting QoL in TDT patients. Thus, we suggest that PRECEDE is a valid and practical model for application in future health promotion and QoL interventions among TDT patients. Finally, more studies are needed to identify other predictive factors of QoL in TDT patients.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
MM and RS contributed to the conceptualization and writing of the first draft of the manuscript. MM and AR Contributed to literature research, data analysis, writing and revision of the manuscript. HJ supervised investigation and methodology. RS was responsible for funding acquisition. MM supervised the research project.
FUNDING
This research is a part of a Ph.D. thesis of Dr. Mina Maheri. Financial support was provided by
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Mina Maheri AU - Alireza Rohban AU - Roya Sadeghi AU - Hamid Joveini PY - 2019 DA - 2019/10/16 TI - Predictors of Quality of Life in Transfusion-dependent Thalassemia Patients Based on the PRECEDE Model: A Structural Equation Modeling Approach JO - Journal of Epidemiology and Global Health SP - 157 EP - 163 VL - 10 IS - 2 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.191001.001 DO - 10.2991/jegh.k.191001.001 ID - Maheri2019 ER -