
COVID-19 Epidemic and Public Health Measures in China
- DOI
- 10.2991/jegh.k.200421.001How to use a DOI?
- Keywords
- COVID-19; epidemic; public health measure; China
- Abstract
Objectives: The study aims to analyze the status quo of public health emergency measures taken in China in dealing with the spread of new coronavirus pneumonia (COVID-19), and to put forward policy suggestions for system construction and improvement.
Methods: According to the official data released by the National Health Commission, the epidemic data of infected people from 0:00 on January 24, 2020 to 24:00 on February 23, 2020 were quantitatively analyzed through statistical analysis. We used EXCEL software to draw the overall epidemic trend chart and Statistical Product and Service Solutions (SPSS) to carry out descriptive statistical analysis of mortality and cure rate. We made qualitative analysis on the emergency measures implemented by national administrative departments and provincial governments to work on controlling and monitoring COVID-19 nationwide spread.
Results: The number of patients diagnosed showed a linear increasing trend, with the slope increasing first and decreasing later. Suspected and new cases showed an inverted V pattern, with the peak occurring on February 8 and 12, respectively. There was a linear increase in the number of deaths and an exponential increase in the number of cures. Over the 31-day study period, the mortality rate fluctuated between 2.0% and 3.4%. The mean cure rate was 10.03%, the minimum value was 1.33%, and the maximum value was 32.05%. The quantitative and qualitative analysis shows that the public health emergency response system constructed in China plays a significant role in controlling the epidemic in a certain period of time.
Discussion: The four-tier emergency management system and the joint prevention mechanism established in China have provided various resources to control the epidemic, but there are still weakness in dealing with the spread of COVID-19. It is suggested to improve and strengthen the emergency management system, public health service system, health legal system, citizen health education, and international exchange and cooperation.
- Copyright
- © 2020 The Authors. Published by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
The ongoing COVID-19 pandemic was reported in China in late 2019 as unexplained cases of pneumonia [1]. On February, the World Health Organization declared this disease as a Public Health Emergency of International Concern, and on March 11, as a pandemic.
In an effort to contain the outbreak, the Chinese government on January 23 closed down the city of Wuhan and urged people from other regions to stay at homes for 14 days during the lunar New Year holiday. All provinces and government departments in China have taken emergency response measures. On February 14, the Chairman Xi Jinping pointed out that ensuring the safety of people’s lives and good health is a major task of the country’s governance. In view of the weaknesses and deficiencies exposed by COVID-19 outbreak, we should persist in doing so, improve the system and mechanism for the prevention and control of major outbreaks, and improve the national public health emergency management system [2]. Based on current spread situation and policy making decision, this research will collect and analyze the data on COVID-19 released by the National Health Commission of China from January 24 to February 23, 2020 to present the COVID-19 epidemiologic trend, and sort out the health measures promulgated from the State Council administrative departments and provincial governments, further to discuss the weakness existing in current public health emergency system, and to put forward countermeasures and suggestions.
2. METHODS
2.1. Data Source
The data are from the epidemic distribution of COVID-19 in China from 0:00 on January 24 to 24:00 on February 23, 2020 released by the National Health Commission, and the information of the official emergency response measures taken by the Chinese government website. The time period is 1 month, i.e. 31 days.
2.2. Analysis Method
The paper selects the indexes such as confirmed, suspected, deaths, and cured population and uses EXCEL to draw the national total change trend chart of COVID-19, and Statistical Product and Service Solutions (SPSS) to calculate the fluctuation range and mean of mortality and cure rate, and to analyze the spread of new coronavirus pneumonia. Through qualitative analysis of the emergency management response measures adopted by various administrative departments and provinces and regions in China, this paper explores China’s public health emergency management framework and capacity to cope with the development of COVID-19 epidemic, so as to further study the existing weakness and propose countermeasures and suggestions.
3. RESULTS
3.1. The Trend of the Total Amount of COVID-19 Diffusion
In Figure 1, the data shows the increase of the number of confirmed patients (increase), the cumulative number of confirmed patients (total), and the number of suspected infected patients (suspect) in this 1 month. The increased cases in this paper refer to the newly increased confirmed cases compared with the previous day. The data in Figure 2 show the cumulative number of deaths (death) and discharges (cured). On January 24, there were 1287 confirmed cases, and on February 23, the total number of confirmed cases was 77,150. The number of confirmed cases (red) showed a linear growth trend, which tended to increase first and then decrease. On February 12, the number of people increased dramatically, from 44,653 on February 11 to 59,804 (Figure 1). It broke through 70,000 for the first time on February 16 and has since slowed. The suspected curve (yellow) and the increase curve (blue) both showed an inverted V-shaped trend. The peak of the suspected curve appeared on February 8, and the maximum value was 28,942. At this time, it was exactly 15 days away from January 23, which was in line with the prediction of the incubation period of 14 days. Since then, the suspected values have fallen, indicating that the “stock” has been reduced. On February 12, the increase curve peaked with a maximum value of 15,152, mainly due to the revision of the criteria for confirmation on February 12, resulting in the number of new confirmed cases exceeding 10,000 on that day. Since then, the number of new cases has dropped significantly and emergency management interventions have gradually come into play. This shows that, due to the long incubation period of the virus, the strong infectivity, and relatively insidious, the emergency response will not appear immediately after the start of the effect, but after a certain response cycle.
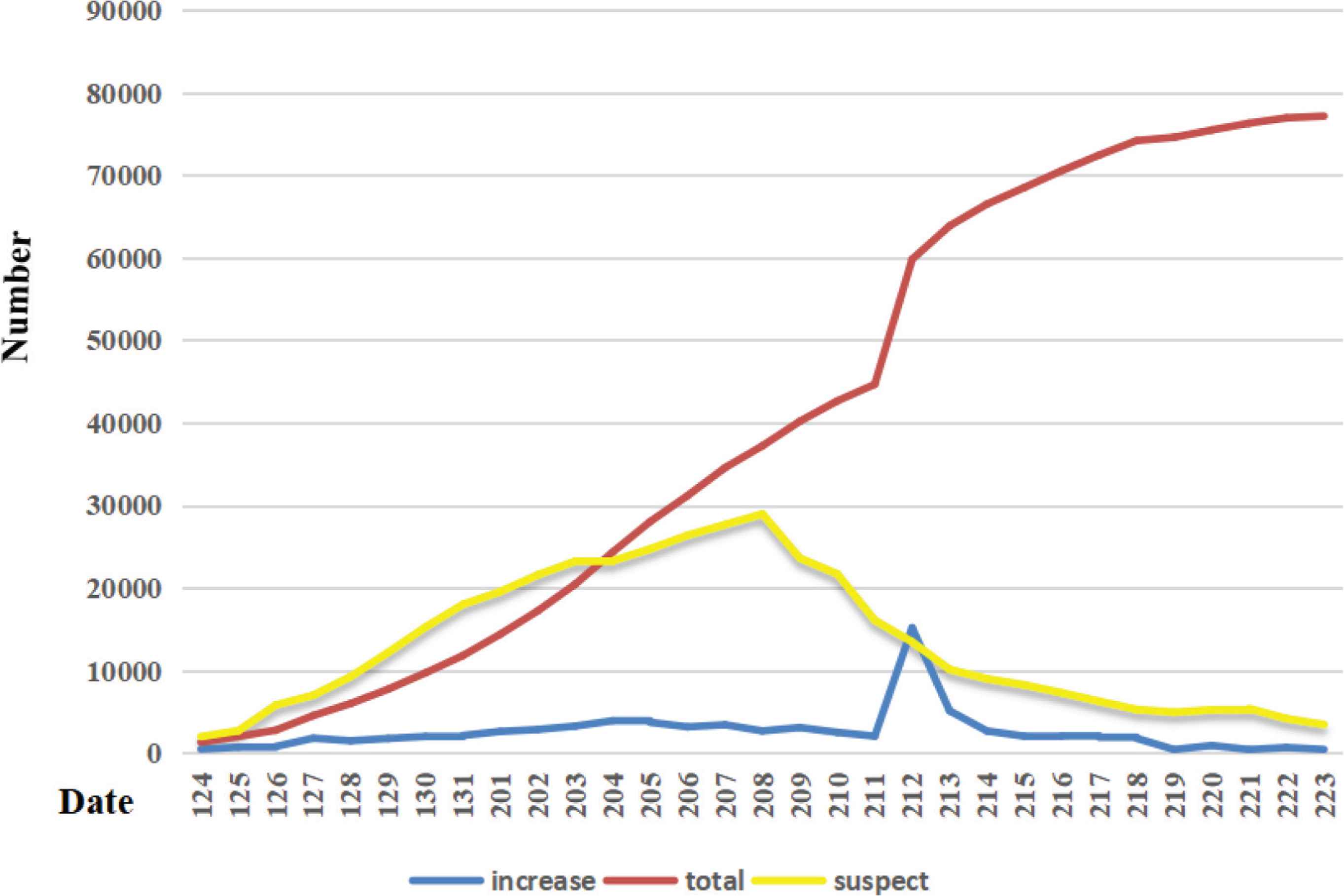
Trends in the spread of new coronavirus pneumonia between 24 January and 23 February 2020.
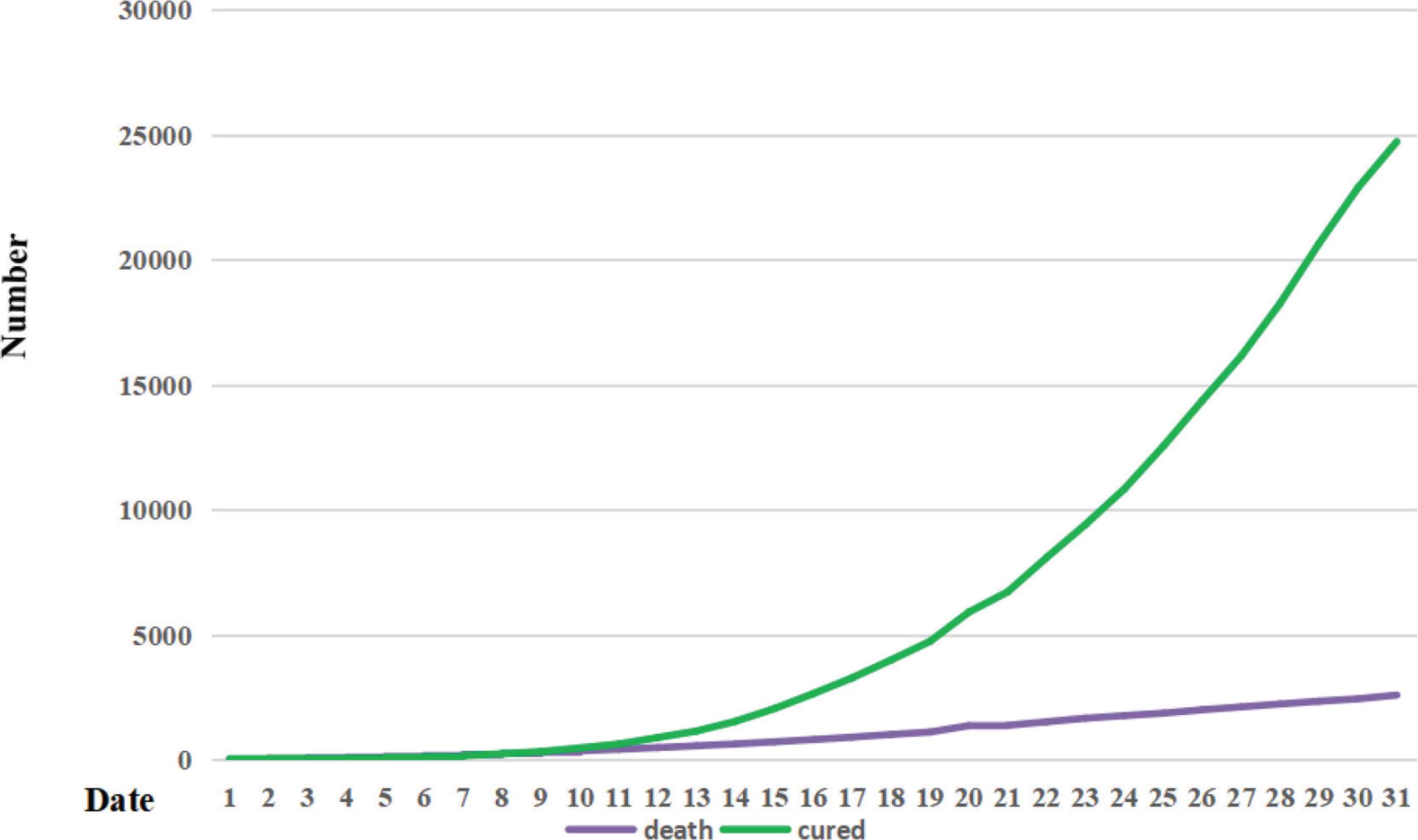
Trends in the mortality and cured cases between 24 January and 23 February 2020.
3.2. Trends in Mortality and Cure Rates
The number of deaths increases slowly, in a nearly linear trend. The number of cured people increases day-by-day, which is similar to the exponential growth trend (Figure 2). The growth rate of the number of people cured was significantly higher than that of the number of died people. In this paper, the specific mortality and cure rate were obtained by dividing the number of deaths and cured cases by the cumulative number of confirmed cases, and descriptive statistical analysis of the mortality and cure rate was conducted by SPSS software (SPSS Inc., Chicago, IL). The results showed that during the 31-day study period, the mortality rate fluctuated between 2.0% and 3.4%, with a minimum of 2.01% on February 4 and 5 and a maximum of 3.36% on February 23. The average cure rate was 10.03%, and the minimum value 1.33% appeared on January 27, and the maximum value 32.05% appeared on February 23. Since February 13, the cure rate has been greater than 10%, and since February 19, the cure rate has been greater than 20%. The significant increase of cure rate and small fluctuation of death rate indicate that the government’s emergency intervention measures are effective and that the emergency management system plays an important role.
3.3. Public Health Emergency Management Framework and Epidemic Response Measures
China’s public health emergency management system is divided into horizontal and vertical system dimensions. In terms of horizontal emergency management, the state council is the highest administrative leading department, and led by the National Health Commission, the joint prevention and control mechanism of public health emergencies was firstly composed of 32 ministries and commissions of the state council (Figure 3). The 32 units included National Health Commission, National Development and Perform Commission, Ministry of Finance, Ministry of Science and Technology, Ministry of Culture and Tourism, Ministry of Civil Affairs, Ministry of Public Security, Ministry of Justice, Ministry of Transport, Ministry of Industry and Information Technology, Ministry of Education, Ministry of Agriculture and Rural Affairs, Ministry of Ecology and Environment, National Audit Office, Human Resources Security Department, Ministry of Foreign Affairs, Ministry of Commerce, Ministry of State Security, Ministry of Natural Resources, People’s Bank of China, Ministry of National Defense, Ministry of Housing and Urban-Rural Development, Ministry of Water Resources, Ministry of Emergency Management, Ministry of Veterans Affairs, The General Administration of Customs, National Radio and Television Administration, General Administration of Sport, Healthcare Security Administration, Ethnic Affairs Commission, State Taxation Administration, and General Administration of Market Regulation. Multi-sectoral and trans-regional cooperation mechanism is adopted to make clear division of labor and form joint forces, and to establish a joint defense and control mechanism of “vertically to the end and horizontally to the edge” [3]. On January 24, solstice on February 22, 32 national ministries and commissions successively issued more than 70 response measures and standard requirements on the prevention and control of the new coronavirus pneumonia. In particular, during the period from January 24 to January 31, 25 ministries and commissions issued more than 30 epidemic prevention and control notices. It covered many emergency response measures including epidemic monitoring, emergency resources supply, daily supplies supply, traffic control regulations, financial subsidies allocation, social order stability, human resource relationship guarantee, medical insurance reimbursement, and drug payment preferential treatment.
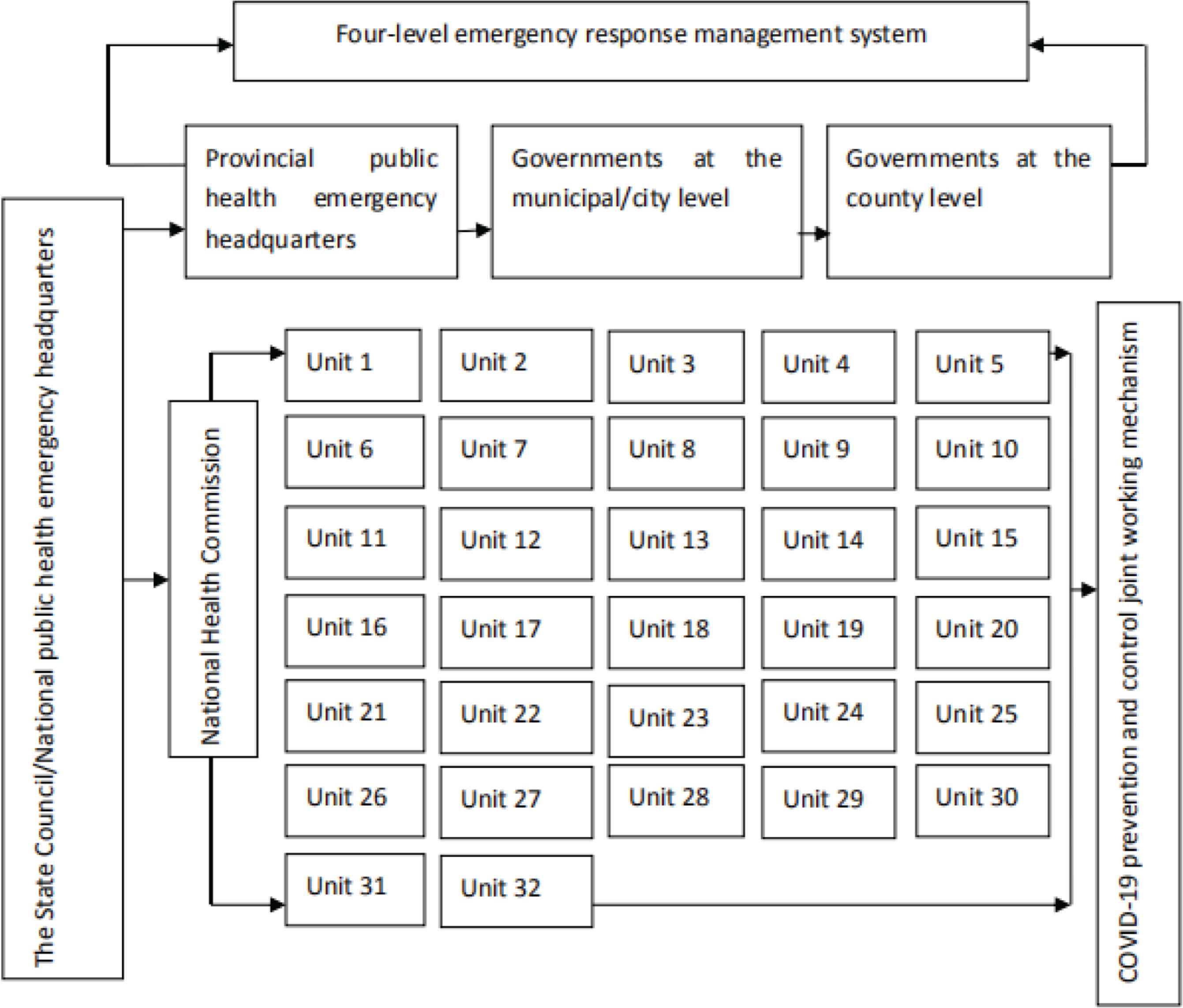
Public health emergency management framework for COVID-19.
Vertical emergency response system refers to the four-level vertical management system of “state–province–city–county”, specifically speaking, the national public health emergency command composed of the state council, which successively directs the emergency management mode of the provincial public health emergency command, prefecture-level government, and county-level government (Figure 3) [4]. General Emergency Plan for National Public Emergencies of China and Contingency Plan for National Work Safety Accidents and Disasters of China classify accident response into four levels, namely, Grade I accident (level I response), Grade II accident (level II response), Grade III accident (level III response), and Grade IV accident (level IV response). The grade I accident indicates that the cumulative number of confirmed cases is very large, and the epidemic situation is very serious. By analogy, level IV indicates a cumulative number of confirmed fewer people [5]. According to the unified decision, deployment and command of the state council, 31 provinces, municipalities directly under the central government and autonomous regions in China successively launched a first-level (level I) response to the new coronavirus pneumonia epidemic from January 23 to January 29, and organized and coordinated the emergency response work within their respective administrative regions. For example, Beijing municipality issued a specific notice and proposal on strengthening the prevention and control of pneumonia caused by new coronavirus. Heilongjiang province set up aid medical team to Wuhan. Hebei province put on the drugs and medical services used by confirmed patients to the regional essential medicine list and local health insurance system. Over 15 provinces including Shandong, Anhui, Guangxi, Hainan, and Tianjin ensure the supply of daily necessities and stabilize the prices of food and epidemic prevention supplies. Zhejiang, Jiangsu and other provinces carry out online government office services. Tianjin and Jiangsu provinces promptly allocate funds for epidemic prevention subsidies.
In addition, under the overall deployment and command of the state council, all provinces carry out trans-regional cooperation. On February 10, the National Health Commission pooled high-quality resources to establish a working mechanism for interprovincial counterpart to support the medical treatment of COVID-19 pneumonia in cities other than Wuhan in Hubei province. In addition to Wuhan, 19 provinces provided support to 16 cities with severe epidemic conditions in Hubei province, and gave full support to Hubei province to ensure patients’ treatment and safeguard, so as to maintain people’s safety and health.
4. DISCUSSION
As early as the end of the SARS in 2003, China established national emergency management system at the macro level, composed of the emergency plan and the emergency management system, mechanism, and legal system [6]. On the basis of summing up the prevention and treatment work of SARS and other emergent acute infectious diseases, a public health emergency management system with graded responsibility and territory-based responsibility was established. The law of the People’s Republic of China on the prevention and treatment of infectious diseases has been amended, and a series of laws, regulations and plans have been formulated, including the regulations on responding to public health emergencies, the national emergency plan for public health emergencies and the national emergency plan for influenza pandemic. A multi-sectoral and joint prevention and control mechanism for the outbreak of acute infectious diseases led by the National Health Commission was established. To promote the joint prevention and control of various departments, the national emergency plan for public health emergencies establishes the principle of “relying on science and strengthening cooperation”, requiring all relevant departments and units to work together and share resources to effectively respond to public health emergencies. In this outbreak of new coronavirus pneumonia, China’s existing emergency management system embodies the principle of “classified management, hierarchical responsibility, block combination and territorial management” mechanism. Especially in terms of resource security, the central government is able to give priority to local governments and give overall command and coordination to multi-party coordination across regions and departments to ensure the delivery of adequate medical relief supplies and life support supplies to the affected areas.
Despite the rapid launch of the public health emergency management mechanism in response to the epidemic, there are still have weakness in the emergency management system, emergency plan system, emergency support capacity, and social publicity and health education in the process of dealing with public health emergencies. The war of the new coronavirus pneumonia reminds us to earnestly study and improve the public health emergency management system, and to gradually establish a public health emergency management system that combines prevention, control, and treatment. For example:
4.1. Improve the Public Health Emergency Management System
China needs to continue to carry out top-level design for building institutions and mechanisms, improve the monitoring system for public health emergencies, and achieve networked and accurate management. China should improve the emergency response mechanism for major outbreaks, establish a centralized, unified and efficient leadership and command system, and improve our ability to respond to major public health emergencies [7]. China should strengthen cross-provincial, cross-regional and -departmental communication, and collaboration mechanisms.
4.2. Optimize the Public Health Service System
China should strengthen the development of a contingency plan system for public health emergencies, formulate contingency plans by category, and specify and standardize the specific contents of such plans. China should focus on improving the ability of medical institutions and public health administrative departments at all levels to respond to and manage public health emergencies. China should increase investment in medical and health resources, strengthen the public health workforce and personnel training, and improve the personnel structure. China should establish an evaluation and incentive system for medical personnel and improve their remuneration.
4.3. Strengthen the Rule of Law in Public Health
China should repair the wildlife protection act. The wild animals carrying the virus are included in the fasting list, the areas of endangered wild animals are strictly protected, and the punishments for those who eat and sell wild animals are clearly defined [8]. China should strengthen publicity of the laws on the prevention and treatment of infectious diseases enacted in China and comprehensively improves our ability to prevent and control infectious diseases in accordance with the law.
4.4. Raise Public Health Awareness
China should intensify efforts to publicize the prevention and treatment of infectious diseases, and conduct popular science education to the general public through the preparation of publicity manuals, popular science books, new online media and other forms. In the community, experts and doctors of infectious diseases will be invited to give training lectures on popular science, so that the public can learn basic knowledge and ideas of epidemic prevention and have basic skills to deal with sudden infectious diseases.
4.5. Facilitate International Exchanges and Cooperation
China should learn from the advanced public health emergency management system across the world, such as World Health Organization, including emergency management organization system, operation mode, early warning and monitoring, scientific research and experiment, and civic education. China should actively participate in international academic exchanges on epidemic prevention and control, work closely with counterparts around the world to share research results, and fight against infectious disease.
5. CONCLUSION
Through analyzing and studying the COVID-19 control in China, especially the public health emergency responses China has taken, this research provides and shares China’s experiences to the world, aimed at helping everyone to fight against this infectious disease in global village.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
All authors contributed in study conceptualization, data curation, formal analysis and writing (original draft, review & editing) the manuscript. TX contributed in funding acquisition, project administration and also supervised the project.
ETHICAL STATEMENT
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Footnotes
Data availability statement: The data that support the findings of this study are openly available in the website of China National Health Commission at http://www.nhc.gov.cn/, Reference number [5].
REFERENCES
Cite this article
TY - JOUR AU - Tingting Xu AU - Ruoyu Yang PY - 2020 DA - 2020/04/28 TI - COVID-19 Epidemic and Public Health Measures in China JO - Journal of Epidemiology and Global Health SP - 118 EP - 123 VL - 10 IS - 2 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.200421.001 DO - 10.2991/jegh.k.200421.001 ID - Xu2020 ER -