
Operationalizing the One Health Approach in Uganda: Challenges and Opportunities
- DOI
- 10.2991/jegh.k.200825.001How to use a DOI?
- Keywords
- One Health implementation; zoonotic diseases; public health threats; Uganda; low-income settings; multi-sectoral collaboration
- Abstract
Uganda is considered as a ‘hot spot’ for emerging and re-emerging infectious disease epidemics. The country has experienced several epidemics including; Ebola, Marburg, plague, Rift Valley fever, yellow fever and Crimean Congo haemorrhagic fever. Epidemics overwhelm health systems, devastate economies and cause global health insecurity. These public health challenges arising from the interaction of humans-animals-environment link require a holistic approach referred to as One Health (OH). OH is the collaborative effort of multiple disciplines working locally, nationally, and globally, to attain optimal health for people, animals, and the environment. Given its situation, Uganda has embraced the OH approach in order to be able to predict, prepare and respond to these public health challenges effectively, though still in infancy stages. In this paper, we present major achievements and challenges of OH implementation, and make recommendations for systematic and sustainable OH implementation. Achievements include: formation of the National One Health (NOH) platform with a Memorandum of Understanding between sectors; a national priority list of zoonotic diseases, the NOH Strategic Plan and a One Health communication strategy to strengthen engagement across sectors and stakeholders. There have also been efforts to integrate OH in academia. The challenges are related to inadequate; coordination across sectors, government commitment, advocacy and awareness creation and research. For systematic and sustainable OH engagements, urgent efforts should be made through government support to address current and related future challenges.
- Copyright
- © 2020 The Authors. Published by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Globally about 75% of newly emerging infectious diseases and 60% of all human infections are of animal origin (zoonoses) [1]. According to the World Health Organization (WHO), one or more new infectious diseases have emerged each year since the 1970s [2]. This has resulted from closer proximity of animals and humans than ever before due to several factors such as: population growth, urbanization, advances in transport and animal industry, deforestation and climate change [3–5]. This close interaction has led to increased transmission and quick spread of diseases from animals to humans [6,7], resulting into epidemics that can potentially overwhelm health systems, and devastate economies [8,9], lead to morbidity and mortality of both animals and humans [10]. Diseases have negative social and economic consequences as well as global health security [10]. Recognizing ecosystem linkages and interdependencies of humans, animals and the environment necessitates a holistic approach to health issues, referred to as One Health (OH). The OH strategy is necessary as there is need for more systematic and diverse experts working together in identifying and responding to global health threats arising at the human–animal–ecosystem interface [11–13]. The OH approach holds promise in mitigating public health threats [14]. The approach has been embraced by WHO, Food and Agriculture Organization (FAO), World Organisation for Animal Health (OIE) and the Global Health Security Agenda (GHSA) as a strategy for promoting the collaborative effort of multiple disciplines working locally, nationally and globally, to attain optimal health for people, animals and the environment [14]. In this paper the authors describe the experience of Uganda including its achievements, opportunities, challenges and recommendations for implementing the OH approach. We start with a brief description of the rationale for and achievements in implementing a OH agenda in the country. This is followed by a description of the challenges that have been faced and continue to face in operationalizing the OH strategy, including what needs to be done to improve the implementation. This is based on available literature and drawn from the authors experience of working with the One Health Central and Eastern Africa Project [now Africa One Health University Network (AFROHUN)] in Uganda [15].
2. RATIONALE FOR OH APPROACH IN UGANDA
Uganda is considered a ‘hot spot’ for emerging and re-emerging zoonotic disease outbreaks because of its biological diversity and high population pressure, increasing the humans-animals interaction presenting high chances of zoonotic pathogens disease spill over [1]. In the recent past, the country has experienced several epidemics including Ebola, Marburg, plague, avian influenza, Rift Valley Fever (RVF), yellow fever and Crimean Congo Haemorrhagic Fever (CCHF) [16]. In addition, a number of zoonotic diseases such as brucellosis, rabies, trypanosomiasis and anthrax are endemic in Uganda [17]. Recently, the country experienced an increase in frequency and intensity of extreme weather variability and epidemics ranging from vector borne to other zoonotic disease outbreaks. For example, RVF which is usually triggered by sustained heavy rains was for the first time reported in Uganda in the South Western part of the country in March 2016 [17]. Uganda also has one of the fastest population growth globally [18] which has resulted in land degradation, wildlife poaching, loss of biodiversity, and increasingly variable climate patterns [19]. This promotes close human interactions with animals that carry new threats [20–22]. In addition, there is a mounting problem of antimicrobial resistance (AMR) with nearly 70% of Enterobacteriaceae isolated from blood cultures at a tertiary hospital in 2014–15 were found to be resistant to third generation cephalosporin and 20% resistant to carbapenem [23]. AMR is a very complex problem, much more multifaceted than any other infectious threat, posing a significant challenge to global health and animal production with significant economic consequences [24]. It is a direct consequence of the selection pressure from antibiotic use in humans, animals, and the environment, thus its control and containment requires a OH approach [24]. Epidemics overwhelm health systems, cause social disruptions and devastate economies. For example recurrent oubreaks of Ebola, Marburg, CCHF, RVF and the current COVID-19 in Uganda, have posed heavy impact on the country in terms economic burden-with interruption of international trade and tourism, in addition to social disruptions and straining health systems [16,25,26]. Therefore, efforts that integrate inputs from multidisciplinary and diverse sets of knowledge holders are needed to understand the risks and find solutions. Multidisciplinary collaborations will significantly advance the fundamental understanding of emerging health threats and spur the development of initiatives that decrease vulnerabilities of communities and ecosystems [11].
3. OH ACHIEVEMENTS IN UGANDA
3.1. Early on Attempts of OH Approach
While the OH approach was not yet institutionalized, Uganda has had some successful multi-sectoral disease response initiatives in the past. These initiatives include: (i) The Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome (HIV/AIDS) epidemic in the 1980s was put under control through strong political leadership (spearheaded by the President) and multi-sectoral collaboration including civil society, other sectors participation; (ii) Uganda established a Veterinary Public Health division within the Ministry of Health (MoH) in the early 1980s. Thus recognizing the importance of the two sectors; human and animal working together. (iii) The Uganda Trypanosomiasis Control Council was established in 1992. Its Coordinating Office-Control of Trypanosomiasis in Uganda as its secretariat was one of the earliest high-level multi-sectoral coordinating bodies for disease response [17]. It is a OH platform to human and animal Trypanosomiasis-working on the tsetse and trypanosomiasis research and control in Uganda. This work is done in collaboration with the Ministry of Agriculture, Animal Industry and Fisheries (MAAIF), Ministry of Health (MoH), Ministry of Finance, Planning and Economic Development, Ministry of Tourism, Trade and Industry, Ministry of Local Government and Ministry of Land, Water and Environment (MWE) [17].
3.2. Formation of the OH Platform and OH Strategic Plan
In addition to the historical attempts, Uganda has continued to embrace the OH approach, though still at a limited scale. The country, is a member of the GHSA and a signatory to the International Health Regulations [27]. In 2013, the Ugandan Veterinary and Medical Associations hosted a OH conference, which resulted in the signing of a OH Memorandum of Understanding (MOU) between the medical and veterinary professions. In 2016, four main government entities: health (MoH); agriculture (MAAIF); Uganda Wildlife Authority (UWA) – an agency under the Ministry of Tourism Wildlife and Antiquities; and Water and Environment (MWE), formed a collaboration (with financial and technical support from The U.S. Agency for International Development Emerging Pandemic Threats 2 Program (USAID/EPT-2) Preparedness and Response (P&R) Project). These sectors established the One Health Framework (OHFW), a document that legalizes their formal collaboration and guides their operations [28]. On 3rd November, 2016; the Uganda National One Health Platform (NOHP) was launched by formalising the OHFW and signing of an MOU between all partners, see Figure 1. The NOHP has two key structures: (i) the One Health Technical Working Group and the Zoonotic Diseases Coordination Office (ZDCO) each with clear terms of reference. The OH technical working group is responsible for advising government, partners and other agencies on OH issues including: technical guidance and oversight to the ZDCO, advocacy and resources mobilization, and reviewing and updating plans and budgets and those of its sub-committees. It is co-chaired by technical directors of the collaborating ministries on a 6 month rotational basis, and has representatives of core government OH sectors and partners organizations such as United Nations agencies, US Goverment agencies, professional bodies (Uganda Veterinary and Medical Associations), academia and research institutions, and other technical partners, see Figure 2. (ii) The ZDCO is the secretariat of the OH Platform and is responsible for coordinating the implementation of OH activities by the government under the supervision of the OH technical working group.
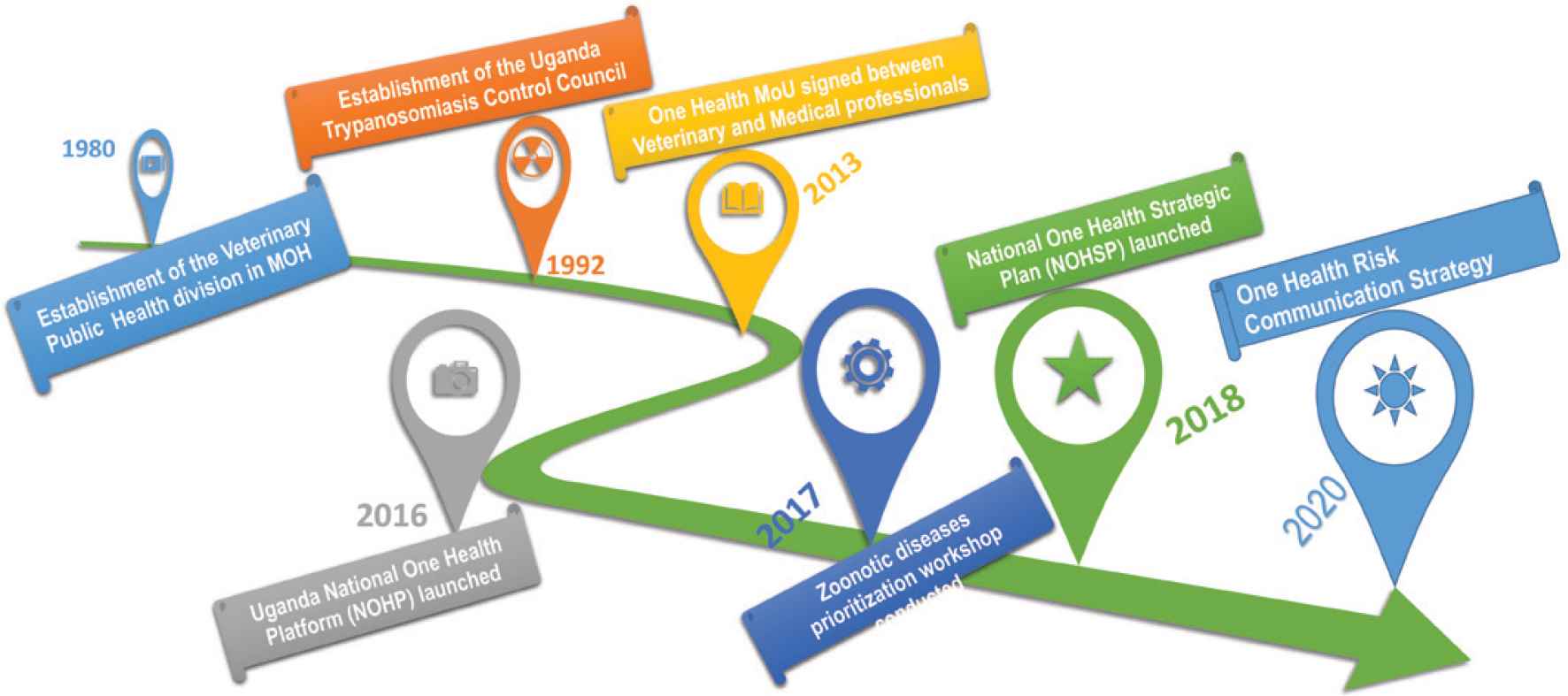
One Health achievements in Uganda.
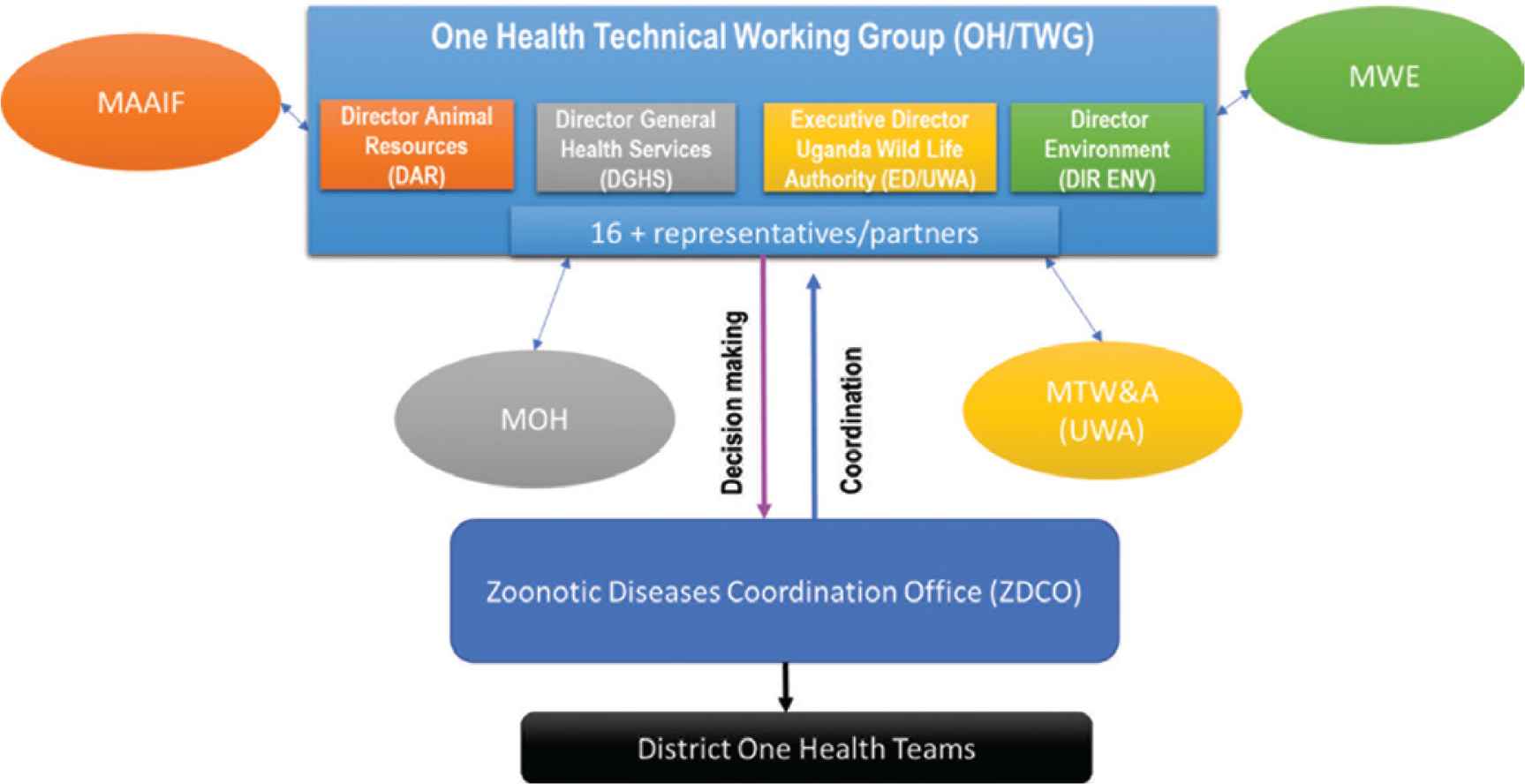
National One Health Platform Organogram.
On 15 February 2018, the National One Health Strategic Plan (NOHSP) was launched laying emphasis on the seven priority zoonotic diseases, AMR, public health threats and related bio-security issues in its initial 5-year period (2018–2022) [17]. Based on the five strategic objectives, the strategic plan covers commitment to OH among high-level government stakeholders. The commitment is focused on institutionalization and capacity building to ensure effective operation of the OH initiatives; outreach to enhance awareness of the value of the OH approach; strengthened preparedness and response to zoonotic diseases, AMR, biosecurity threats, and communication. In addition, Uganda has a National Action Plan on AMR [29]. Also a OH communication strategy to strengthen communication across the sectors (to enhance coordination, collaboration and networking of the sectors and stakeholders in promoting internal communication on preparedness and response to public health emergencies, AMR and other OH issues in the country) has been developed. The OH technical working group and ZDCO are charged with management, leadership, monitoring and evaluation, and coordination of implementation of the Uganda One Health Strategic Plan [17].
3.3. Zoonotic Diseases Prioritization
In addition, Uganda supported by the U.S. Center for Disease Control (CDC)/GHSA conducted a OH zoonotic disease prioritization workshop that identified and prioritized zoonotic diseases of greatest national concern in order to enable focused and guided use of limited resources optimally [30]. This risk mapping and prioritization is recommended by World Bank as an entry point to OH approach [24]. Seven zoonotic diseases; rabies, viral hemorrhagic fevers, anthrax, brucellosis, plague, zoonotic influenza viruses and African trypanosomiasis were prioritized [30].
3.4. Integration of OH Approach in Academia
Last but not least, there have been efforts to integrate OH in academia through the One Health Central and Eastern Africa (OHCEA)/One Health Workforce (OHWF) Project- rebranded to AFROHUN. This is a network of universities in eight countries (including Uganda), consisting of 23 institutions of public health, veterinary medicine and environmental sciences [15]. OHCEA has played a key role in building capacity in infectious disease detection, prevention and response. With support from USAID, OHCEA focused on strengthening training and educational programs in universities to create a multidisciplinary workforce with skills and competencies needed to effectively respond to emerging pandemic threats in the Eastern, Central and Western African region [31] which is considered a “hot spot” for emerging and re-emerging infectious diseases.
4. CHALLENGES AND OPPORTUNITIES IN IMPLEMENTING OH IN UGANDA
While significant progress has been made, Uganda still has challenges in the implementation of OH as well as opportunities described below including mechanisms for sustainable OH engagements.
4.1. Coordination Across Sectors
Traditionally, the medical and veterinary professionals and sectors have focused on the improvement of human health and livestock production, respectively as their primary objective [32]. In Uganda, response to disease outbreak has been traditionally through the main responsible government ministries such as health (MoH), agriculture (MAAIF), wildlife (UWA) and environment (MWE), working as individual sectors (silo system) which has caused wastage and inefficiency with less impact [3,17]. This compartmentalization has been criticized less desirable in low income countries, where the zoonotic disease burden is high. A joint approach on diagnosis, data sharing, monitoring and surveillance systems, training and interventions has been recommended [5,23] because it improves opportunities to prevent pathogens from ‘spilling over’ from one species to another [33]. Collaboration and cooperation have been recommended to be critical because they are fundamental to linking these independent pillars of OH i.e. human and animal health systems and environmental health and management, to ensure that maximum sustainable health and economic benefits are achieved in the most efficient manner [24].
Recently, efforts have been put in place to make OH gain a firm institutional foothold such as development of the Framework (OHFW), formation of the Platform (NOHP) and the Strategic Plan (NOHSP) as described above. However, apart from having meetings of NTF, the ZDCO, OH technical working and partners, there is little attempt to operationalize OH beyond meetings hence actual collaboration in implementation has largely not been achieved. This is similar to what Lee and Brumme [34] reported in their paper on operationalizing of OH at a global level. In a marburg outbreak of 2017, late and lack of involvement of some of key stakeholders and weak leadership and coordination structures at the centre and the districts was highlighted as a major challenge [26]. From a stake holder mapping of OH, several barriers to operationalizing OH in Uganda were noted including: (i) Unstreamlined collaboration and communication among sectors including poor personal relations among staff within the sectors which affects communication; (ii) Lack of effective coordination and commitment to OH preparedness and response efforts; (iii) Lack of an agreed mechanism for sharing information across sectors and partners; and (iv) Building consensus among sectors usually takes a long time. Consequently, national response to outbreaks still happens in silos, as the interventions are not well coordinated, despite having the same goal and joint meetings. One reason attributed to these fragmented initiatives is the lack of funding for OH activities in the country. For instance, the coordinating body (ZDCO) has no physical office, uses volunteer staff, and has no budget. OH activities such as response to outbreaks depend on availability of money in individual sectors and this results in disjointed participation, contrary to the OH approach resulting in wastage of resources and limited impact on disease prevention and control. In addition, although chairing the OH platform is on the rotational basis by technical directors of the key ministries (health, agriculture, wildlife and environment), the period of the term is just 6 months [17]. This is really not enough time for any impactful work to be done. It seems to be just a ceremonial activity with no serious expectations from the seating chair and ministry.
Although the MoH has a modest surveillance system, the disease detection, reporting and responding mechanisms are slower in the animal sector [9]. There is also no joint surveillance of zoonotic diseases which would lead to early detection, prevention and response to outbreaks [9]. In the workforce assessment report of 2016, several concerns regarding principles and roles of partnership were raised including different perspectives regarding which sector or institution should assume a lead role on OH, and lack of a clear collaboration processes [11,34]. This is related to the established technical roles of individual sectors, and a reflection of the desire to protect institutional mandates and any future resources accruing to them [34]. Successful approaches that have been suggested include interdisciplinary surveillance, reporting and laboratory collaboration, coordinated data sharing and interpretation, and strong communication channels for disease reporting and rapid action [24]. There is need to invest in strong laboratory capacity and build coordination between laboratories of human and animal sectors, because this critical to equip countries to rapidly detect pathogens of public health concern and for the other disease pathogens. Rapid diagnosis is necessary in the containment of a disease-both known and novel, leading to less lengthy societal disruptions in the numerous sectors that can be affected during an epidemic (e.g., education systems, vaccination campaigns, tourism, supply chains, agricultural trade, etc) [24].
The effective and desired collaboration will require a move away from only meetings to actual joint planning, budgeting, and programs as well as collaborative projects [11]. In addition, there is need for improvement in communication and information sharing between sectors as well as ensuring projects foster transparent inter-sector/agency collaboration. It is critical to forge co-equal, inclusive collaborations across multiple sectors/agencies in the country, and to promote resiliency of Ugandans through an enhanced understanding of climatic change impacts on health risks to people, animals and the environment [11]. One idea that has been put forward by Kayunze et al. [35] in Tanzania is the need for guidelines for collaboration. Applying the principles of collaboration, learning and adaptability [36] could help improve and sustain collaboration and coordination in OH over time.
4.2. Government Commitment and Political Will
Besides providing oversight and management of OH activities, the government’s responsibility involves political commitment including availing financial resources for OH. It will be important for Uganda to mirror the strong multi-sectoral response that was put in the fight against the HIV/AIDS epidemic in the early 1980s, characterised by strong political leadership and civil society participation where it registered successful disease response and control [37]. However, health initiatives in Uganda heavily depend on donor funding which is not sustainable and tends to focus on selected diseases, interventions and populations [34]. The current achievements in Uganda (OH framework), the Platform (NOHP), priorization of the zoonotic diseases, OH Strategic Plan (NOHSP), described above have been solely driven by external funding such as USAID and CDC through P&R. The P&R Project ended in 2018, leaving a number of initiatives including implementation of the NOHSP and drafting of the OH policy incomplete. Apparently, there seems to be no commitment from government to take over OH activities which has a great bearing on the operationalization of the OH Strategic Plan (NOHSP) and implementation of OH in general.
One of the major challenges affecting response to the number of outbreaks that has happened in Uganda, is late release of funds or no funds to implement response plans. This was reported in both the after-action review reports for Marburg and highly pathogenic avian influenza. The lack of emergency funds at the affected district/s results in slow response and demotivation of the players [25,26].
World Bank recommends that individual countries are fundamental to a coordinated global program; neither donors, nor international agencies, can lead such a program on their own. While recognizing that some of these threats are global, programs that will be effective in reducing these increasingly threats must be initiated, owned and led by countries. The international community can provide critical advice and support, implementation and sustaining of the programs remains countries’ responsibility [24]. For example, Uganda recently had outbreaks of avian influenza and anthrax where infected birds and cattle should have been destroyed/buried in order to contain the situation. However, lack of compensation from the government affected the farmers’ compliance with these measures, as they rather sold the meat of the infected carcasses cheaply, than lose completely [25].
Going forward, there is an urgent need for the government to take up responsibility and commit funds to OH, including interdisciplinary research that will inform appropriate policy and practice. To strengthen resource mobilisation, the Strategic Plan (NOHSP) suggested two ways on how OH funding can be availed: (i) That key sectors such as health (MoH), agriculture (MAAIF), environment (MWE), wildlife (UWA) and others should commit and mainstream OH plans and activities in their policies, budgets and workplans [17]; (ii) Funding should be put in a central place such as the Prime Minister’s Office which already has the National Policy for Disaster Preparedness and Management [38] where epidemics are already taken care of and money can be accessed whenever required. It is important for the Platform (NOHP) and other stakeholders to conduct targed advocacy especially the Parliament in order to push for approval of the national OH budget which should be sustained. Parliamentary approval of a OH budget should take into consideration the overall national socio-economic development where OH is central to the country’s target of being a middle income country by 2040 [39]. This is also recommeded by the World Bank [24]. There is also need to design and conduct advocacy engagements with political leaders at national, district and community levels regarding the benefit of OH. In addition, increased mobilization of external assistance, and engagement of the private sector, Non-governmental Organizations and Civil Society Organizations through greater public-private partnerships is required to support national and lower level OH activities, given that these epidemics/pandemics do not spare any sector. World Bank recommends that there is a need to provide for a balance between short and long-term actions. Immediate action is required in case of outbreaks, while for the longer term, the need to build capacity that performs core public health functions to the international standards established by OIE and WHO is critical. In addition, capacity for environmental health must be more fully established and integrated in public health systems along the prevent, detect, respond, and recover cascade to fully operationalize OH in the context of infectious disease but also more widely, such as protection of natural resources and systems [24].
4.3. OH Policy and Other Relevant Laws
Although, the country currently lacks policies, laws and institutional mandates that foster OH, policy frameworks, institutional structures and a programme implementation plan remain important for successful zoonoses control [32]. There is need for a National OH policy which is a critical tool for planning, budgeting and implementation of OH activities. Laws preventing environmental degradation and other public health threats that are OH related are needed. The wetlands coverage has significantly diminished, currently at 8.9% intact, 4.1% degraded and 2.6% completely lost. Deforestation has been a major challenge in Uganda leading to decline of forest cover from 24% in 1990 to 9% in 2017 and only 12% is under strict nature reserve [19] and continues to be lost at a fast rate with the recent give away of Budongo Central Forest Reserve for sugar growing. On a good note some of relevant bills are in the pipeline and these include the Climate Change and the National Environment Bills which were drafted and submitted to Parliament to review [19]. These need to be expidited and implemented. Relatedly, socio-economic drivers of OH challenges such as population explosion, poverty and their effects on land use should be addressed. Although, Uganda prioritized seven zoonotic diseases [30], the policy on zoonoses mainly focuses on livestock production by: improving public health standards for animal products, and reducing economic losses in order to promote export of livestock and livestock products [15]. Based on this policy, the control of zoonotic diseases such as rabies from dogs which may not directly benefit the livestock economy may not be prioritised [32]. This example makes a good case for the technical value of OH, human rabies eradication efforts will not succeed if not addressed in animal populations [24].
4.4. Lack of Awareness and Documented Mechanisms for Operationalization of OH
Lack of awareness about OH, as well as why and how to implement it, is lacking in Uganda. The sensitization efforts have been on a limited scale, and there is need to create a critical mass of people who appreciate the need for OH. Even the few people that understand OH have inadequate understanding of actual processes of operationalization of the approach. As was pointed by Lee and Brumme [34] in their paper, there are no comparative case studies of successful or unsuccessful OH implementation. The publicatione in particular success stories of OH in action would offer valuable lessons on how to implement and sustain the OH approach. There is a need for studies focusing on the establishment and maintenance of institutional arrangements for OH to provide answers to important questions (what, why, and how) to guide operationalization of OH [34], see Table 1. The other challenge is that support for OH is expressed at high levels-national level, but its implementation on the ground remains limited due to a wide range of competing priorities [3]. This is how the prioritization of the OH issues at the national level becomes critical [24].
| 1. | What processes are needed to engage relevant institutional players? |
| 2. | How can collaboration and cooperation across the sectors be fostered? |
| 3. | What forms of governance are adopted to structure institutional contributions? |
| 4. | What implications do these arrangements have for resource distribution and re-distribution? |
| 5. | What impact have these arrangements had on human–animal–environmental health? |
Key questions that need answers to guide operationalization of OH
For the approach to be embraced, wide advocacy to all stakeholders including communities is very critical. Moving forward, there is need to invest in intensive advocacy and training to garner national support for OH as this will foster collaboration on OH programs. Sharing best practices in building partnerships and tackling complex health threats locally and nationally is recommended through conferences, joint meetings and public dialogues. Such engagements can be organized and coordinated through the existing Platform-NOHP, OH Communication Strategy, but there is need to set a budget to implement it.
4.5. Engaging Community Stakeholders in OH
The need for community engagement as important change agents should be emphasized, given the vast public health challenges affecting individuals, households and communities [40]. Outbreaks including zoonotic diseases start and end in communities, thus communities have a significant role in prevention, surveillance, early detection, rapid, and effective response to outbreaks. Communities are therefore crucial in the design of appropriate, context-specific and acceptable interventions. The OH approach promotes participatory community-based approaches which take into account traditional and local knowledge [11]. This is consistent with the goals of the global health effort which stresses the value and necessity of seeking participation from local communities and building interventions that draw on their capacities and resources, rather than top-down approaches. For example in an outbreak of Marburg in Kween and Kapchorw districts in Uganda in 2017, the locals exposed themselves by visiting bat caves to get droppings to fertilize their soils [26]. In the same outbreak, there was community resistance during the response, hampering contact tracing and follow-up. This was mainly due to misconceptions about the disease with a believe that it was witchcraft [26].
Therefore, it is important to work with such communities in order to understand the potential risks of disease transmission – taking into account the complexity and specificity of local conditions [40]. Engaging communities is also key in developing and implementing interventions that can be owned by the community and have sustainable impact. There is no doubt, the local people have immense understanding of their environments and ecosystems [11] and this knowledge should be tapped into, and sometimes improved by technical innovations for wider and sustainable benefit.
4.6. OH Workforce Development
Hotez advocated for training of a new generation of global health scientists with capacity to collaborate and think out of the box in all global health aspects [40]. Operation of universities in Uganda need to go beyond the traditional silos and foster an enviroment that will stimulate innovative problem solving [40]. Currently, there is hardly any systematic support for OH training and career opportunities in the country. The existing efforts including capacity building for pre-and in-service workforce at selected institutions and districts in the country are implemented by OHCEA/OHWF which is not adequate and sustainable just like many other donor funded intiatives. The Government needs to channel resources toward buiding capacity and integrating institutional players, across the human health, animal health, and the environment sectors.
The other challenge is that to date, the OH initiative has been majorly championed by a few disciplines, with limited involvement of social sciences, environmental health and others [41,42]. Strengthening efforts to bring the less involved disciplines on board, and in-service training, will be paramount [43]. To effectively train in OH across all levels (pre-service, in-service and communities), the Ministry of Education, universities and other training instituitions need to innovate on how to incorporate OH teaching including research and innovations, through inter-disciplinary delivery models. Incorporation of OH in teaching would ensure disciplines appreciate the contribution of other professions which will create a workforce and communities that embrace the OH approach. The training/delivery models could include joint lectures and practical/field work as has been demonstrated by OHCEA [15]. In addition to training, it is important to create career opportunities for OH trainees; especially the government should make deliberate effort to develop and implement a responsive recruitment mechanism capable of absorbing the OH workforce into employment. Furthermore, it will be important that the Government supports development of training infrastructure including ‘OH Hubs’ or ‘Centers of Excellence’ which will be central in providing a framework for capacity building and coordination of country-wide activities.
4.7. OH Implementation and Research
For decades, OH has been majorly focused on zoonotic diseases. However, given the current public health threats in Uganda and many other countries are facing including pollution, toxic waste, and climate change, it is critical to develop a broader implementation of OH beyond zoonotic trans-boundary threats such as Ebola and avian influenza. OH is inclusive and useful in addressing a broad range of public health challenges facing human, animal and environmental health [24]. In addition to zoonotic diseases and AMR that are a result of human, animal and environment interaction and need urgent action include; pollution, biodiversity loss, food insecurity, climate change, chemical toxicology [24]. Moving forward, the NOHSP should be developed beyond the priority zoonotic diseases and AMR, to comprehensively address other issue like land use, environmental toxicology, climate change, and food safety which should be reflected in the policy.
Interdisciplinary research and innovation [34], through integrating input from all disciplines is needed to inform appropriate policies and practices that decrease vulnerabilities of communities and ecosystems [11]. Demonstration through a retrospective and prospective evidence that OH interventions lead to better cross-species health outcomes is necessary. Benefits of collaboration at a pragramitc level may include resource efficiencies in conducting routine work such as; transport sharing between the sectors for example transporting human and animal vaccines when conducting immunization outreaches, sample collection to enable surveillance for multiple priority diseases, etc. In addition, through expanded information access and coordinated implementation of projects such as sampling methodologies, time of data collection, multi-sectoral projects may also generate value through earlier or more complete and accurate understanding of disease ecology and epidemiology that leads to more efficient and effective risk management, with possible time savings in disease investigations and avoiding consequences of delays [24]. As pointed out in Conrad’s paper [40], documenting the added value of collaboration across disciplines in preventing and controlling neglected zoonotic diseases, and also other health challenges that are of OH concern is important. However, there is currenly little support for OH research training and career opportunities in Uganda that would help to enable OH strengthen collective action across sectors [24].
5. CONCLUSION
Uganda is vulnerable to zoonotic diseases and other OH challenges due to its increasing animal, human and environmental interactions. The country has recently experienced multiple outbreaks of highly pathogenic zoonotic diseases including Ebola, Marburg, and Rift Valley fever and the ongoing COVID-19 epidemic. Recognizing that ecosystem linkages and interdependencies necessitate a holistic approach to health issues positions the OH approach as a well-matched tool for advanced understanding of public health threats in Uganda and globally. However, effective and sustainable implementation of OH initiatives in Uganda require: government’s support including funding; improved coordination and collaboration across sectors-inlcuding private sector; pre-service and in-service capacity building and a national OH policy including a comprehensive strategy for advocacy.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
EB conceived the idea and wrote the first draft of the manuscript. All the authors revised and approved the manuscript.
FUNDING
This work was supported by
ABBREVIATIONS
- CDC,
Center for Disease Control;
- EPT-2,
Emerging Pandemic Threats 2 Program;
- GHSA,
Global Health Security Agenda;
- HIV/AIDS,
the human immunodeficiency virus/acquired immunodeficiency syndrome;
- MAAIF,
Ministry of Agriculture, Animal Industry and Fisheries;
- MoH,
Ministry of Health;
- MWE,
Ministry of Water and Environment;
- MOU,
Memorandum of Understanding;
- NOHP,
Uganda National One Health Platform;
- OH,
One Health;
- OHCEA,
One Health Central and Eastern Africa;
- OHFW,
One Health Framework;
- OHWF,
One Health Workforce;
- OHTWG,
One Health Technical Working Group;
- OIE,
World Organisation for Animal Health;
- P&R,
USAID Funded Preparedness and Response Project;
- USAID,
The U.S. Agency for International Development;
- UWA,
Uganda Wildlife Authority;
- ZDCO,
Zoonotic Diseases Coordination Office.
REFERENCES
Cite this article
TY - JOUR AU - Esther Buregyeya AU - Edwinah Atusingwize AU - Peninah Nsamba AU - David Musoke AU - Irene Naigaga AU - John David Kabasa AU - Hellen Amuguni AU - William Bazeyo PY - 2020 DA - 2020/08/28 TI - Operationalizing the One Health Approach in Uganda: Challenges and Opportunities JO - Journal of Epidemiology and Global Health SP - 250 EP - 257 VL - 10 IS - 4 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.200825.001 DO - 10.2991/jegh.k.200825.001 ID - Buregyeya2020 ER -