
Serosurvey for Health-Care Workers Provides Supportive Evidence for the Effectiveness of Hydroxychloroquine Prophylaxis against SARS-CoV-2 Infection
 , Archana Pate3, Aruna Shankarkumar2, , Shreyasi Athalye2, , Shweta Shinde1, Umair Ahmed Bargir1, , Mangesh Pate3, Makarand Ganpule3, Meena Pruthi3, Hemant Patil3, Manisha Rajan Madkaikar1, *,
, Archana Pate3, Aruna Shankarkumar2, , Shreyasi Athalye2, , Shweta Shinde1, Umair Ahmed Bargir1, , Mangesh Pate3, Makarand Ganpule3, Meena Pruthi3, Hemant Patil3, Manisha Rajan Madkaikar1, *, - DOI
- 10.2991/jegh.k.210518.001How to use a DOI?
- Keywords
- Sero-surveillance; SARS-CoV-2; healthcare workers; hydroxychloroquine; prophylaxis
- Abstract
Background: The Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) pandemic has resulted in occupational exposure among Healthcare Workers (HCWs) and a high risk of nosocomial transmission. Asymptomatic infection and transmission of infection before the development of symptoms are well-recognized factors contributing to the spread of infection. We conducted a cross-sectional observational study to understand the seroprevalence of SARS-CoV-2 infection among HCWs and to verify the appropriateness of infection control measures, particularly Hydroxychloroquine (HCQ) prophylaxis.
Methods: A cross-sectional sero-surveillance study was conducted among 500 HCWs in Dombivli and surrounding Mumbai Metropolitan area (Maharashtra, India) between 21st July and 3rd August 2020. The vulnerability of the study participants to SARS-CoV-2 infection was ascertained through a history of (i) involvement in direct care, (ii) exposure to aerosol-generating procedures, (iii) co-morbidities, (iv) Personal Protective Equipment (PPE) use, and (v) HCQ prophylaxis. SARS-CoV-2 IgG antibodies were tested using COVID KAVACH anti-SARS-CoV-2 IgG antibody detection enzyme-linked immunosorbent assay (ELISA) from Zydus Cadila. A systematic analysis of the correlation between the development of antibodies and factors affecting vulnerability to infection was performed.
Results: The overall SARS-CoV-2 seroprevalence in the study population was 11%. Providing direct care to COVID-19 patients (Adjusted OR 16.4, 95% CI 3.3–126.9, p = 0.002) for long hours and irregular use of PPE (Adjusted OR 3.78, 95% CI 1.1–11.9, p = 0.02) were associated with an increased incidence of seropositivity. Prophylaxis with HCQ may have a role in reducing the vulnerability to infection as depicted by univariate and multivariate analysis (Adjusted OR 0.55, 95% CI 0.3–0.9, p = 0.047). It was also noted that those not on HCQ prophylaxis were threefold more prone to infection and developed severe disease as compared to those on HCQ prophylaxis.
Conclusion: Prophylaxis with HCQ may have a role in mitigating the incidence and severity of SARS-CoV-2 infection. Although vaccination is the most robust strategy to safeguard against COVID-19, it will be months before vaccination percolates to the masses. In the face of the second wave of COVID-19, the use of HCQ prophylaxis in combination with use of face-masks regularly may be considered as a cost-effective measure for population dense areas like urban slums where social distancing is not possible.
- Copyright
- © 2021 The Authors. Published by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
The Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) pandemic has resulted in occupational exposure among Healthcare Workers (HCWs) and a high risk of nosocomial transmission [1]. The WHO Weekly Epidemiological Update (2nd February 2021), reported over 1.29 million infections with SARS-CoV-2 among HCWs across 183 countries by 31st January 2021 accounting for approximately 8% of cases [2]. Early reports from China and Italy had mentioned that 29% and 9% respectively of the total cases were HCWs [3,4]. SARS-COV-2 testing for symptomatic HCWs in UK, Netherland, and India revealed SARS-CoV-2 infection in 18%, 11% and 5% of the tested HCWs respectively [5–7].
Healthcare workers had not been well prepared for the outbreak especially in departments other than infectious diseases, and the general lack of awareness among the staff to take precautions and inadequate training on the use of Personal Protective Equipment (PPE) added to the situation [8]. Also, asymptomatic infection and transmission of infection before the development of symptoms are well-recognized factors contributing to the spread of infection [9]. Laboratory testing based on reverse transcription polymerase chain reaction (RT-PCR) does not necessarily reflect on the infectivity among HCWs [10]. The availability of serological tests for anti-SARS-CoV-2 antibody determination has made it possible to study the seroprevalence and seroconversion in this high-risk population [11]. Some studies on seroprevalence among HCWs in Wuhan, Germany, and Italy have reported it to be 3.8%, 1.6% and 3.4% respectively [12–14]. The importance of understanding the dynamics of transmission in HCWs lies in planning strategies for the reduction of nosocomial spread.
The search for a medication that would reduce the risk of infection has led to the repurposing of existing medications [15]. One such drug is Hydroxychloroquine (HCQ) which has attracted the attention of the scientific community globally, and Randomized Controlled Trials (RCTs) are underway to assess the efficacy of HCQ in providing effective prophylaxis to those at high risk of contracting the disease [16]. HCQ prophylaxis is recommended by the Indian Council of Medical Research (ICMR) National Taskforce for COVID-19 for asymptomatic HCWs [17].
Some studies on postexposure therapy with HCQ conclude that it did not prevent SARS-CoV-2 infection or symptomatic COVID-19 in healthy persons exposed to a PCR-positive case patient [18,19]. The question of preventing COVID-19 with HCQ prophylaxis remained unanswered by initial results of RCT conducted by Grau-Pujol et al. [20] and Rajasingham et al. [21] as the studies were underpowered.
We report a cross-sectional sero-surveillance study conducted among HCWs in Dombivli and the surrounding area which is a part of the Mumbai Metropolitan Area (MMR) in India. Our study aimed to understand the seroprevalence of SARS-CoV-2 infection among HCWs and to verify the appropriateness of infection control measures, particularly pre-exposure prophylaxis with HCQ.
2. MATERIALS AND METHODS
2.1. Design
A cross-sectional sero-surveillance study was conducted among HCWs in Dombivli and the surrounding areas (MMR, Maharashtra, India) between 21st July and 3rd August 2020 as a collaborative study by the Indian Medical Association Dombivli and ICMR-National Institute of Immunohaematology and the data was analysed in August 2020.
2.2. Participant Details and Study Procedure
Healthcare workers involved in the care of suspected and confirmed COVID-19 patients at dedicated COVID hospitals in Dombivli area were invited to participate in the study. They were requested to fill a survey questionnaire adopted from the WHO risk assessment tool for exposed HCWs (WHO/2019-nCoV/HCW_risk_assessment/2020.2) after informed consent. The vulnerability of the study participants to SARS-CoV-2 infection was ascertained through a history of (i) place of duty and involvement in the direct care of COVID-19 patients, (ii) performing or exposure to aerosol-generating procedures, (iii) presence of co-morbidities, (iv) use of PPE, and (v) use of immune-modulators which was collected through a structured questionnaire. A history of the development of symptoms of a viral illness in the preceding 3 months and RT-PCR testing were also recorded. Only those who completed the survey questionnaire were included in the study. About 3 ml blood was collected per participant and tested for SARS CoV-2 IgG antibodies using COVID KAVACH anti-SARS-CoV-2 IgG antibody detection ELISA from Zydus Cadila.
2.3. HCQ Prophylaxis
Hydroxychloroquine prophylaxis was defined as an intake of HCQ by asymptomatic HCWs as recommended by the ICMR National Taskforce for COVID-19, with a loading dose of 400 mg twice a day on day 1 followed by 400 mg weekly. The HCWs who consumed HCQ were divided into four groups – No HCQ, and intake of HCQ for <6 weeks, 6–10 weeks and >10 weeks. Participants who did not indicate the number of weeks of intake of HCQ prophylaxis were not considered for purpose of regression analysis.
2.4. Ethical Approval
The study is approved by the Institutional Ethics Committee of ICMR-National Institute of Immunohaematology.
2.5. Analysis
The data were collated using Microsoft Excel, and statistical analysis was done using Graph pad prism8 (Chicago, IL, USA) for Microsoft Windows. Primary univariate analysis was performed using the Chi-square and Fisher’s exact tests to correlate the development of antibodies and the factors affecting vulnerability. A secondary analysis was performed using multivariate logical regression for factors that significantly affected vulnerability to infection according to the primary analysis.
3. RESULTS
Of the 560 HCWs who were provided with the survey questionnaire, 500 who completed the survey were included in the study. The characteristics of the participant group and history of a viral illness are summarised in Table 1.
| S. No. | Characteristics | Sero-positive (n = 55) | Sero-negative (n = 445) | p |
|---|---|---|---|---|
| 1 | Median age (in years) | 40 | 44 | |
| 2 | Sex | |||
| Male | 67.3% | 58.4% | 0.2 | |
| Female | 32.7% | 41.6% | ||
| 3 | Primary place of work | |||
| Out-Patient department/Pharmacy/X-ray department/ECG | 12.4% | 87.6% | 0.9 | |
| Medical unit/ICU/Emergency/OT/Either or all | 10.2% | 89.8% | ||
| Laboratory | 13.5% | 86.5% | ||
| Administration | 8.7% | 91.3% | ||
| Others including teleconsultation and support services like an attendant, ambulance services, security, etc. | 9.8% | 90.1% | ||
| 4 | Co-morbidities | |||
| Diabetes | 10.9% | 14.3% | 0.6 | |
| Hypertension/Heart disease | 16.3% | 16.6% | ||
| Asthma/Lung disease | 3.6% | 1.6% | ||
| Others | 5.4% | 6.7% | ||
| 5 | Type of exposure to COVID-19 patients | |||
| Direct | 81.8% | 78.4% | 0.8 | |
| 6 | Presence of symptoms consistent with a viral illness in the preceding three months | 33 | 152 | 0.0003 |
| 7 | Tested with RT-PCR | 69.7% | 41.4% | NA |
| 8 | SARS-CoV-2 RT-PCR | |||
| Test positive | 60.9% | 17.5% | ||
| Test negative | 39.1% | 82·5% | ||
| 9 | HCWs reporting affected family members (n = 200) | 2.5% | 3% | NA |
Participant characteristics and history of symptoms
Overall, 11% (55/500) participants were detected with IgG antibodies to SARS-CoV-2. About two-fifth (33/55) of those with IgG antibodies had experienced symptoms of a viral infection in the preceding 3 months. Among the symptomatic participants, 23/33 underwent RT-PCR testing, 14 (60.9%) were confirmed with COVID-19 disease and treated as per standard treatment guidelines.
A comparison of the seroprevalence between HCWs positioned in dedicated COVID-19 care and those working in non-COVID-19 areas revealed a higher seroprevalence of 17.2% among those working in non-COVID-19 areas as compared to 9.6% among those providing direct care to COVID-19 patients. In univariate analysis, the variables which affected vulnerability to infection, in a statistically significant manner include the number of hours of exposure, rational use of PPE, and HCQ prophylaxis as depicted in Table 2. The development of IgG antibodies correlated well with the number of hours of exposure (p = 0.002) as shown in Figure 1. Running Table 2 HCQ prophylaxis numbers through logistic regression, for each increasing category of HCQ use we noted a dose–response OR = 0.70 (95% CI 0.50–0.99, p = 0.032). This trend is much stronger among the ever-exposed categories (i.e., excluding the never-used HCQ people), per-category OR = 0.27 (95% CI 0.11–0.65, p = 0.0036). None of the participants who took HCQ prophylaxis reported serious side effects (specifically arrhythmias).
| Variables | SARS-CoV-2 antibody positive (n = 55) | SARS-CoV-2 antibody negative (n = 445) | p |
|---|---|---|---|
| Rational use of PPE as per WHO recommendations | 85.4% | 71.5% | 0.04* |
| No. of hours of exposurea | |||
| >8 | 24.4% | 19.5% | 0.002** |
| 4–8 | 44.4% | 22.3% | |
| <4 | 31.1% | 58.2% | |
| Exposure to aerosol-generating procedures | 22.7% | 18.8% | 0.55 |
| HCQ prophylaxisb | |||
| HCQ < 6 weeks | 25% | 11.8% | 0.01* |
| 6–10 weeks | 11.4% | 22.8% | |
| >10 weeks | 2.3% | 10.7% | |
| No HCQ | 61.4% | 54.5% | |
| Presence of co-morbidity | 12 | 97 | >0.99 |
Only those providing direct care were included in analysis (n = 45 for the sero-positive group and n = 349 for the sero-negative group).
Data regarding the number of weeks of intake of HCQ was missing for 101 HCWs, hence excluded from the analysis.
Boldface p-value indicates statistical significance (*p < 0.05, **p < 0.01).
Analysis of factors affecting vulnerability and statistical significance for their differences (p) in univariate analysis
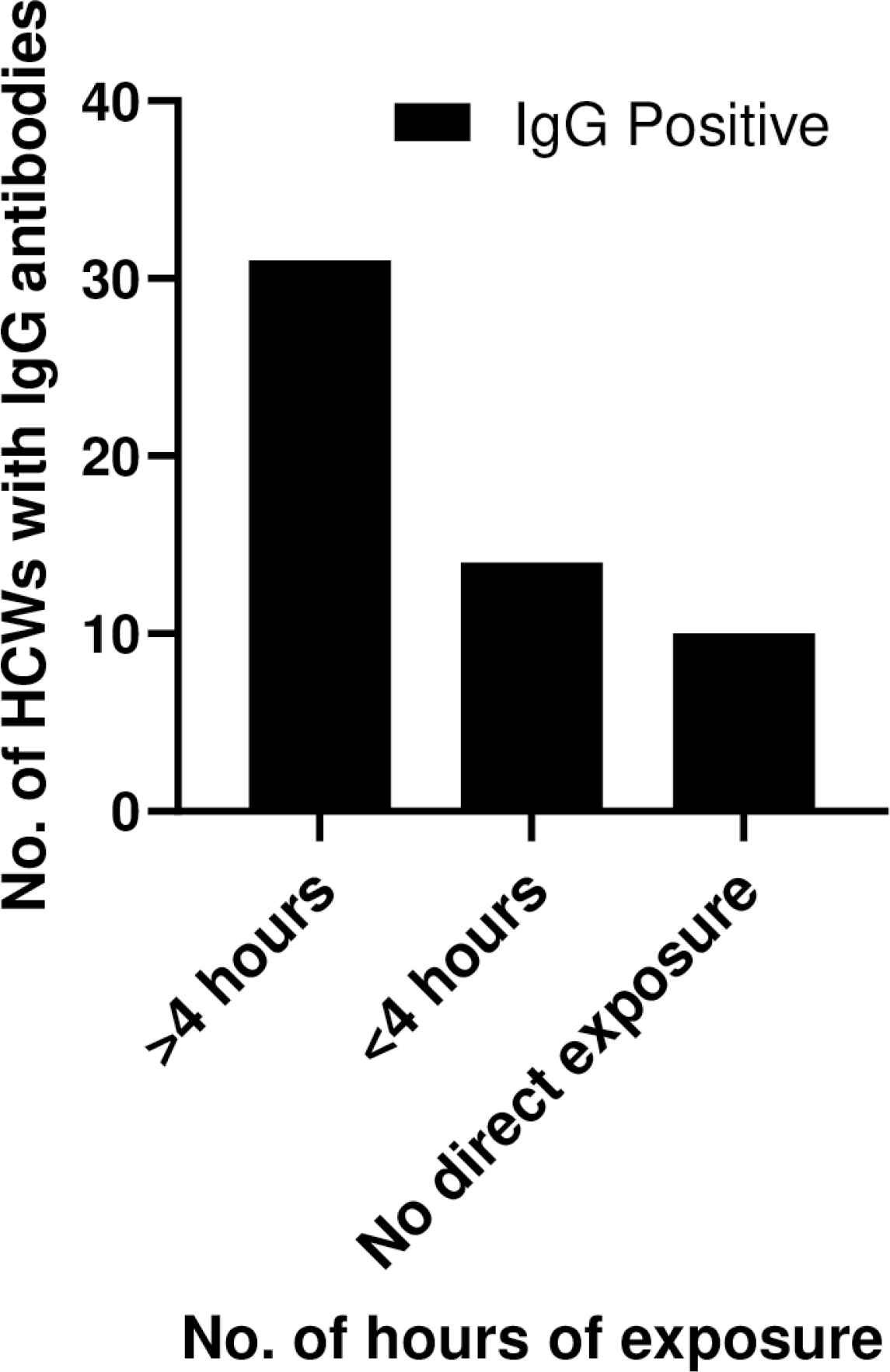
Correlation of the number of hours of exposure with the development of IgG antibodies.
Multivariate analysis for factors that might affect the development of antibodies, namely direct contact with COVID-19 patients, use of PPE, and HCQ prophylaxis was performed using multivariate logical regression. Those who had provided direct care to COVID-19 patients had sixteen times the odds of developing antibodies (95% CI 3.3–126.9, p = 0.002) than those working in non-COVID areas, and non-usage of PPE increased the odds of infection by almost four times (95% CI 1.1–11.9, p = 0.02). HCQ prophylaxis was associated with reduced odds of developing antibodies to almost half (95% CI 0.3–0.9, p = 0.047) as depicted in Table 3.
| Factor affecting vulnerability to infection | Adjusted odds ratio | 95% CI | p |
|---|---|---|---|
| Direct care | 16.40 | 3.3–126.9 | 0.002** |
| Never used PPE | 3.78 | 1.1–11.9 | 0.020* |
| HCQ prophylaxis | 0.55 | 0.3–0.9 | 0.047* |
Boldface p-value indicates statistical significance (*p < 0.05, **p < 0.01).
Odds ratios of the presence of anti-SARS-CoV-2 antibody for study variables in multivariate logistic regression analysis Dependent variable: Positive SARS-CoV-2 antibody test Analysis of independent variables:
Amongst participants who were on HCQ prophylaxis (n = 279), 111 reported symptoms suggestive of a viral illness in the preceding 3 months, SARS-CoV-2 infection was confirmed by RT-PCR testing in seven (2.5%), and 2/7 required hospitalization. However, both of them had mild symptoms, did not require supplemental oxygen, and were hospitalized only for observation. On the other hand, 78 among those not on HCQ prophylaxis (n = 221) were symptomatic, SARS-CoV-2 infection was confirmed in 13 (5.9%) by RT-PCR, and 9/13 required hospitalization. All that hospitalized required low molecular weight heparin and steroids in addition to the standard treatment, and supplemental oxygen was required by two among those admitted.
A total of 71 (14.2%) participants reported a prior SARS-CoV-2 RT-PCR test. All participants who had a prior nucleic acid SARS-CoV-2 test were either symptomatic at the time of testing or among contacts of confirmed cases, which is consistent with the local practice. Of the 71 participants, 25 tested positive; however, only 14/25 participants were seropositive for SARS-CoV-2 IgG antibodies, and 11/25 were seronegative.
Of 200 participants who provided information on affected family members, 11 a reported an affected family member.
4. DISCUSSION
The overall seroprevalence of SARS-CoV-2 in the study population was 11%. Only about two-fifths of the HCWs who had detectable anti-SARS-CoV-2 antibodies reported symptoms consistent with a prior viral illness. This reiterates that testing only symptomatic may miss a substantial number of infected HCWs. This may have implications on nosocomial transmission. Also, 99/189 HCWs from both seropositive and seronegative groups who had experienced symptoms of a viral illness did not undergo RT-PCR testing due to the presence of mild or non-specific symptoms. However, 12 (12.1%) of these had detectable antibodies. As such, HCWs being a high-risk group should not ignore even mild symptoms and should undergo testing.
Comparing the results with sero-prevalence studies from other countries, our study reveals a higher seroprevalence compared to studies from Wuhan, Germany, and Italy [12–14]. This might be indicative of complacence in observing strict precautions at all times, especially in non-COVID-19 wards and non-testing despite the presence of symptoms.
Four of the 11 HCWs who were seronegative despite SARS-CoV-2 infection confirmed by RT-PCR testing had less than 3 weeks’ duration between symptom onset and testing which might be responsible for a negative result. Three participants were asymptomatic and detected RT-PCR positive on contact screening, and one participant had reported mild symptoms, as such they might have titres below detectable levels. This has been observed in a recent study which reported low neutralizing antibody titre in as many as 30% individuals recovering from mild SARS-CoV-2 infection. Three participants had borderline OD values; and a repeat testing might be required in these participants.
Direct care to COVID-19 patients for long hours was associated with an increased incidence of seropositivity; this might be attributed to overcrowding in the OPD and emergency areas, exposure to aerosol-generating procedures, and suboptimal use of PPE. Optimizing working conditions by adjusting shift schedules, following strict precautionary measures like hand hygiene practices, and regular use of PPE may help reduce the risk of infection [22]. Strict adherence to strategies for RT-PCR testing in case of symptoms and quarantine of confirmed SARS-CoV-2 infected HCWs may also help in limiting the risk of nosocomial transmission.
Prophylaxis with HCQ may have a role in reducing the vulnerability to infection [7,23] as depicted by univariate and multivariate analysis. It was also noted that those not on HCQ prophylaxis were threefold more prone to infection as confirmed by RT-PCR as compared to those on HCQ prophylaxis. Thus, HCQ may even have a role in mitigating the severity of the disease among those infected.
Hydroxychloroquine inhibits endosomal acidification thereby elevating the pH of endosomes and prevents replication of SARS-CoV-2. Also, the drug appears to interfere with terminal glycosylation of the cellular receptor, Angiotensin converting enzyme (ACE-2) thereby affecting the virus-receptor binding and entry of virus into the cell. The immunomodulatory effect may also help in preventing cytokine storm associated with COVID-19 disease [24]. The universal availability, low cost, long half-life and weekly dosing schedule are other benefits that make HCQ an appropriate choice as a prophylactic agent. Although several trials are underway to assess the efficacy of HCQ prophylaxis for SARS-CoV-2 infection, conclusive evidence to support or refute the use of this drug is awaited [16,23]. Our observational study supports the evidence in favour of HCQ prophylaxis which is also reported by three other Indian studies by Chatterjee et al. [7], Goenka et al. [25] and Khurana et al. [26]. Our manuscript shows that there is both a benefit of HCQ ever-use and a dose–response in weeks of use which has also been reported by the other Indian studies mentioned above. A recent review of HCQ PrEP by Stickler and Fesler [27] mentions the decreased rate of COVID-19 mortality in patients with autoimmune diseases taking HCQ. All these observational studies including ours enrolled a total of 2660 patients and provide corroborative evidence of the effectiveness of HCQ prophylaxis for frontline HCWs. None of these studies were RCTs which might be considered a limitation of the study. However, RCTs require a longer time for completion and an average cost of millions of dollars thereby taking a long time to generate any conclusive results.
The effectiveness of the regular use of PPE and HCQ prophylaxis can also be emphasized by comparing seroprevalence among HCWs and the city-wide seroprevalence which was reported in early July to be about 33% in the city of Mumbai [28]. The results with PPE usage and HCQ pre-exposure prophylaxis can be considered useful in face the second wave of COVID-19. Although vaccination is the most robust strategy to safeguard against COVID-19, it will be months before vaccination percolates to the masses. The use of HCQ prophylaxis in combination with use of face-masks regularly may be considered as a cost-effective measure for population dense areas like urban slums where social distancing is not possible.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
AP contributed in conceptualization, investigation. RMY contributed in methodology, project administration, investigation, data curation and analysis, visualization, writing and editing the manuscript. AS and SA contributed in investigation, validation. SS, Mangesh P, HP, Meena P, and MG contributed in investigation. UAB contributed in designing the data collection tool, resources. MRM contributed in supervision, funding acquisition, resources, validation, review of manuscript and approval of final version for submission.
FUNDING
The work was supported by the
ACKNOWLEDGMENTS
- 1.
Dr Vijay Suryavanshi, Commissioner Kalyan Dombivli Municipal Corporation for Administrative approval to conduct the study in Dombivli area.
- 2.
Dr Suresh Kadam, MOH, KDMC for facilitating the study.
- 3.
Technical Officer Mrs. Vaishali Pujari, Technical assistants – Mr. Ganeshmoorthy, Mrs. Shreya Chavan and Mr. Ramesh Kawle for support in antibody testing and data entry in excel and Mr. Shailesh Shinde for assistance in sample collection.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Reetika Malik Yadav AU - Archana Pate AU - Aruna Shankarkumar AU - Shreyasi Athalye AU - Shweta Shinde AU - Umair Ahmed Bargir AU - Mangesh Pate AU - Makarand Ganpule AU - Meena Pruthi AU - Hemant Patil AU - Manisha Rajan Madkaikar PY - 2021 DA - 2021/05/23 TI - Serosurvey for Health-Care Workers Provides Supportive Evidence for the Effectiveness of Hydroxychloroquine Prophylaxis against SARS-CoV-2 Infection JO - Journal of Epidemiology and Global Health SP - 283 EP - 288 VL - 11 IS - 3 SN - 2210-6014 UR - https://doi.org/10.2991/jegh.k.210518.001 DO - 10.2991/jegh.k.210518.001 ID - Yadav2021 ER -