
Covid-19 Effects on ARTErial StIffness and Vascular AgeiNg: CARTESIAN Study Rationale and Protocol
 , Bart Spronck2, 3, , Bernhard Hametner4, , Alun Hughes5, , Patrick Lacolley6, , Christopher C. Mayer4, , Maria Lorenza Muiesan7, , Chakravarthi Rajkumar8, , Dimitrios Terentes-Printzios9, , Thomas Weber10, , Tine Willum Hansen11, , Pierre Boutouyrie1, , on behalf of the ARTERY Society
, Bart Spronck2, 3, , Bernhard Hametner4, , Alun Hughes5, , Patrick Lacolley6, , Christopher C. Mayer4, , Maria Lorenza Muiesan7, , Chakravarthi Rajkumar8, , Dimitrios Terentes-Printzios9, , Thomas Weber10, , Tine Willum Hansen11, , Pierre Boutouyrie1, , on behalf of the ARTERY Society- DOI
- 10.2991/artres.k.201124.001How to use a DOI?
- Keywords
- COVID-19; coronavirus; inflammation; vascular ageing; arterial stiffness
- Abstract
In December 2019, an outbreak of pneumonia caused by a novel Coronavirus (COVID-19) spread rapidly worldwide. Although the clinical manifestations of COVID-19 are dominated by respiratory symptoms, the cardiovascular system is extensively affected at multiple levels. Due to the unprecedented consequences of the COVID-19 pandemic, the ARTERY society decided to launch the Covid-19 effects on ARTErial StIffness and vascular AgeiNg (CARTESIAN) study — the first international multicentre study into the effects of COVID-19 on non-invasive biomarkers of vascular ageing. The main study objective is to evaluate the presence of Early Vascular Ageing (EVA) 6 and 12 months after COVID-19 infection. Secondary objectives are to study the effect of COVID-19 disease severity on EVA, to investigate the role of psychosocial factors in COVID-19 induced EVA, and to investigate the potential modifying effect of comorbidities and chronic treatments. In the CARTESIAN study, a broad array of cardiovascular measurements, including carotid-femoral pulse wave velocity, central blood pressure, carotid ultrasound, brachial flow-mediated dilatation, will be performed. To date, 43 centres from 21 countries have agreed to participate, with an expected study population of >2500 individuals. To our knowledge, CARTESIAN will be the first study to provide insight into the relationship between COVID-19, its severity, and early vascular ageing in a large cohort, potentially enabling future care and diagnostics to be more focused on the most vulnerable.
- Copyright
- © 2020 The Authors. Publishing services by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Vascular ageing, an age-related deterioration in vascular structure and function, is an integrated marker of overall Cardiovascular (CV) risk burden on the vasculature over time. While age-dependent arterial damage typically appears in the fifth decade of life, there is strong variability between individuals with some displaying Early Vascular Ageing (EVA). Vascular ageing, driven by chronological ageing and accelerated by risk factors such as hypertension and diabetes, occurs both in the micro- and macro-vasculature: the cross-talk between the two perpetuates a vicious cycle further aggravating diabetes and hypertension, ultimately leading to CV events [1]. Life-time exposure to risk factors promotes the development and accumulation of subclinical vascular changes that directs an individual towards a trajectory of EVA [2]. This has led to the notion that vascular age may better relate to CV outcomes than chronological age [3].
In December 2019, an outbreak of pneumonia caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), occurred in Wuhan (Hubei province, China), and spread rapidly throughout China and worldwide, representing an unprecedented challenge for humanity. Although the clinical manifestations of the disease caused by SARS-CoV-2 (coronavirus disease 2019, COVID-19) are dominated by respiratory symptoms, the CV system is also extensively affected [4,5]. For this reason, the Association for Research into Arterial Structure and Physiology (ARTERY) Society, launched an initiative to study the effects of COVID-19 infection on non-invasive biomarkers of early vascular ageing. This activity is supported by the European Cooperation in Science and Technology (COST) Action CA18216 VascAgeNet [6].
2. SCIENTIFIC BACKGROUND
Severe acute respiratory syndrome coronavirus 2 infection affects the CV system at multiple levels. First, SARS-CoV-2 is able to directly infect endothelial cells, inducing marked endothelial damage and inflammation [7]. In autopsies from COVID-19 patients, cardiac infection was demonstrated [8]; endothelial injury and endothelialitis (with infiltration of inflammatory cells into vessel walls) was consistently present in multiple vascular beds [9]. In addition, an increase of a Kawasaki-like inflammatory syndrome, the most common primary vasculitis in children (known to be associated with aortic stiffness [10]), has also been observed [11]. These vascular changes may result from a complex process involving either disturbed cell metabolism as a result of cell infection or immune impairment mediated by cellular immunity and cytokine actions. SARS-CoV-2 is able to infect endothelial cells through Angiotensin-converting Enzyme 2 (ACE2), and downregulates ACE2 expression such that the enzyme is unable to exert protective effects, thus resulting in organ injury [12]. Impaired ACE2 activity enhances vascular inflammation and plaque formation, and increases vascular stiffness in experimental animals [13,14]. In people with diabetes and hypertension low ACE2 activity is associated with endothelial dysfunction and arterial stiffening [15], thus suggesting that accelerated vascular ageing might occur by this pathway after SARS-CoV-2 infection.
Second, COVID-19-associated inflammation may induce immune-mediated vascular damage, as already shown in a wide range of primarily inflammatory diseases [16]. Dysregulated immune response and cytokine-release syndrome, due to overactivation of innate immunity characterizing severe COVID-19, may result in indirect, immune-mediated damage to the systemic vasculature and to increased risk of CV events [17]. For example, survivors of hospitalised pneumonia have an increased risk of CV disease during up to 10-years follow-up and it is likely that cases infected via respiratory virus outbreaks will experience similar adverse outcomes [18], which could be prevented by timely vaccination [19]. COVID-19-associated severe systemic inflammation may induce immune-mediated damage to the vasculature, thus increasing long-term risk of CV events. A large body of evidence shows that accelerated vascular ageing (with arterial stiffening and increased risk of CV events) occurs in chronic inflammatory diseases [16,20,21]. Preliminary studies suggest that arterial stiffening may also occur after sepsis [16,22].
Third, COVID-19 alters metabolic and cardiac markers. Survivors of SARS-CoV infection had a markedly increased prevalence of metabolic complications, including impaired glucose metabolism and dyslipidaemia, 12 years after infection [23], possibly related to marked release of inflammatory mediators, especially interleukin (IL)-1β and tumor necrosis factor α(TNF-α), which promote systemic insulin resistance and β-cell damage [24]. Alternatively, these consequences could be related to treatments administered during the acute phase of infection, such as corticosteroids, antiviral drugs, or immunomodulator drugs [23]. The metabolic consequences of COVID-19 are still unknown, but may be similar and further accelerate vascular ageing and increase long-term CV risk. In addition, one study has reported diastolic dysfunction in 16% of patients with COVID-19 [25], consistent with previous findings in SARS-CoV patients [26]; this is compatible with our current hypotheses that SARS-CoV-2 seems to particularly affect small vessels and capillaries and that cardiac diastolic dysfunction may relate to abnormalities in the micro-circulation. Alternatively, the observed diastolic dysfunction could be attributable to myocarditis [27,28]. A significant proportion of patients have shown increased cardiac troponin-I levels, associated with worse prognosis [29,30].
Fourth, psychosocial factors may play a role in COVID-19-associated vascular ageing. These factors are increasingly recognised as a relevant risk factor to take into account in CV disease prevention [31]. A significant proportion of patients having survived COVID-19 show Post-traumatic Stress Disorder (PTSD), anxiety, depression, and insomnia [32]; this phenomenon might be amplified if the patient needed intensive care [33]. Indeed, survivors of intensive care hospitalisation have impaired quality of life [34], and roughly half of them have symptoms of depression, anxiety and PTSD, associated with increased mortality during follow-up [35]. A direct correlation between PTSD symptoms and arterial stiffness has been demonstrated in Polish survivors from deportation to Siberia in their childhood [36], suggesting that PTSD may contribute to the increased CV risk also in COVID-19 survivors. Social inequalities also play a crucial role in accelerating vascular ageing [37], and foster health disparities in COVID-19 severity and mortality [38].
Fifth, chronic or acute treatments and comorbidities may play a role in COVID-19-associated vascular ageing. Previous chronic treatments (e.g., renin–angiotensin system blockers) or treatments administered in the acute phase (such as corticosteroids, immunomodulators, antiviral drugs, and invasive respiration) may have direct consequences on vascular ageing in COVID-19 patients, being either protective or deleterious. For example, corticosteroid use is associated with better survival outcome in COVID-19 patients [39], but its chronic use has been associated with increased risk of CV events in the general population [40]. Some authors suggest that chronic use of drugs protecting the endothelium might attenuate COVID-19 severity [7,41]. Studies exploring the effect of blockers of the renin-angiotensin system on COVID-19 outcome found either a beneficial [42] or neutral impact [43,44]. Moreover, these drugs may be protective on long-term CV consequences of SARS-CoV-2 infection. CV comorbidities, including ischemic heart disease, hypertension, obesity and diabetes are the most important contributors to the severity of COVID-19 [45–47]. Impaired vascular function in these patients may play a role in worsening COVID-19 prognosis. Diabetic patients in particular, due to a compromised innate immune response, exhibit increased susceptibility and enhanced disease severity following SARS-CoV-2 infection [48].
Taken together, accurate CV phenotyping associating arterial and cardiac measurements of stiffness, and structure and function tests (endothelial function), assessing both the micro- and the macro-vasculature and their cross-talk, is needed to ascertain whether COVID-19 infection is associated with EVA and to establish which mechanisms are involved in COVID-19 related accelerated vascular ageing. It is therefore that we are presenting the Covid-19 effects on ARTErial StIffness and vascular AgeiNg (CARTESIAN) study (Figure 1).
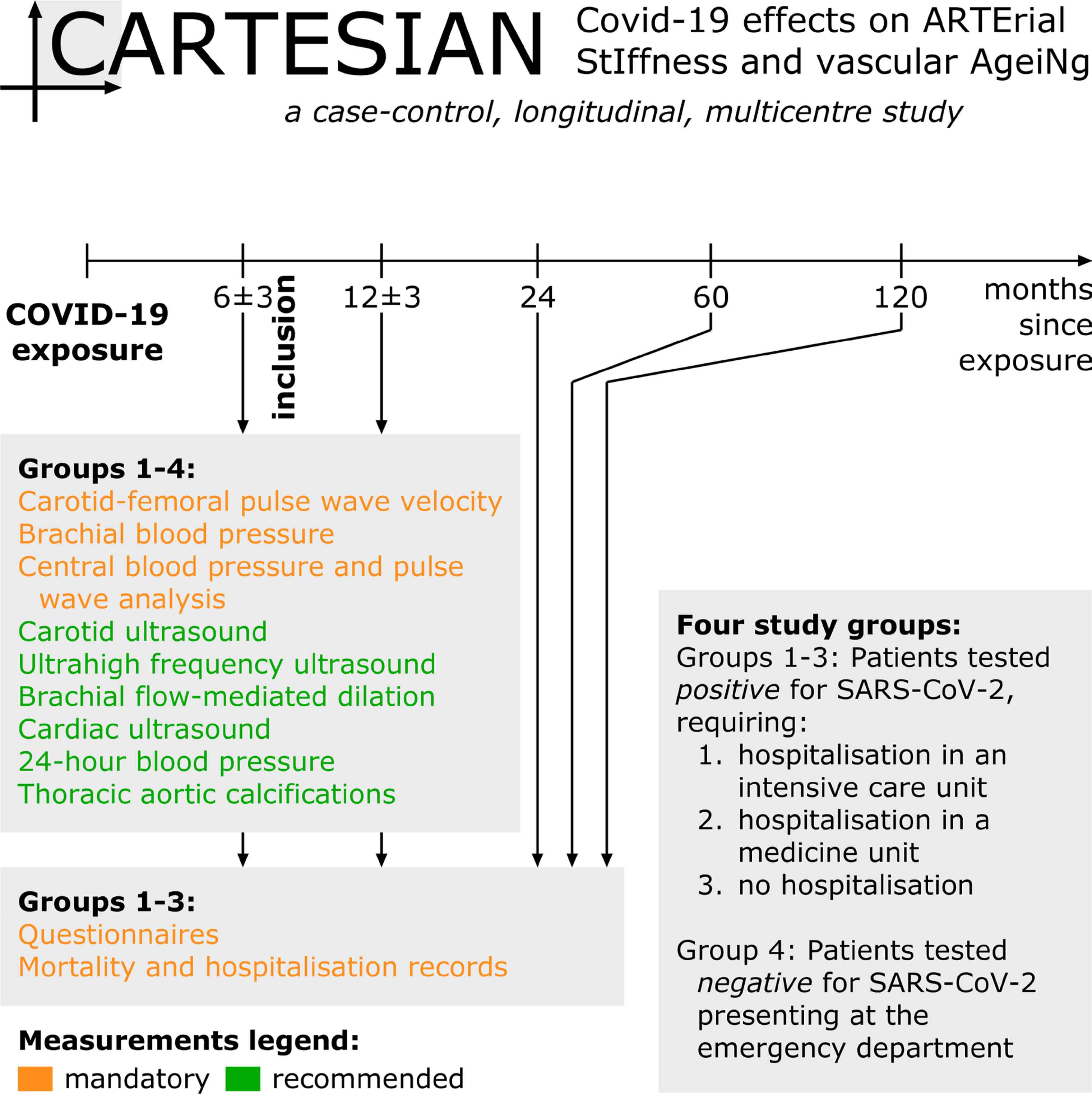
CARTESIAN study overview.
3. HYPOTHESES AND OBJECTIVES
We hypothesise that accurate CV phenotyping by structural and functional tests, assessing both the micro- and the macro-vasculature and their cross-talk, will demonstrate the presence of accelerated vascular ageing in COVID-19 survivors. We further hypothesise that COVID-19-related vascular ageing will correlate with COVID-19 severity and with pre-existing cardiometabolic disease. We will also explore the role of pre-existing cardiometabolic disease; including metabolic alterations, residual chronic inflammation and psychosocial factors and the possible influence of chronic and/or acute treatments in COVID-19-associated accelerated vascular ageing.
The main objective of the CARTESIAN study is to evaluate the presence of EVA after COVID-19 infection. The primary endpoint will be carotid-femoral Pulse Wave Velocity (PWV), an established biomarker of EVA. PWV will be evaluated at 6 ± 3 and 12 ± 3 months after infection. PWV-derived vascular age and difference between chronological and vascular age will also be calculated according to comparison to reference values [49] as well as according to a more recent approach, validated for cardiovascular event prediction [50].
Secondary objectives are:
- (1)
To investigate the presence of altered arterial properties in the carotid, radial and digital arteries by standard and ultrahigh-frequency ultrasound; endothelial dysfunction in the brachial artery by flow mediated dilation; micro-macrovasculature crosstalk alterations by wave separation/intensity analysis of aortic pressure and flow curves; 24 h-central blood pressure (in equipped centers);
- (2)
To investigate the presence of: cardiac dysfunction by cardiac ultrasound (in equipped centers);
- (3)
To investigate temporal evolution of vascular ageing biomarkers between 6 and 12 months in the four groups;
- (4)
To investigate the role of psychosocial factors (including PTSD) in COVID-19-related EVA; and
- (5)
To investigate the association with EVA of previous chronic treatments or treatments administered in the acute phase, as well as of pre-existing cardiometabolic disease.
As a pre-planned study extension, in COVID-positive patients, mortality causes and hospitalization data from electronic medical records will be collected 2, 5, and 10 years after the beginning of the study. Questionnaires to evaluate health status and psychometric tests will be also sent by email/mail.
The resulting findings have the potential to improve CV risk assessment and patient management in the long term.
4. MATERIALS AND METHODS
The CARTESIAN study is a prospective, multicentre, cohort study.
4.1. Study Population
The study will include three groups of individuals with recent (6 ± 3 months) documented exposure to SARS-CoV-2 and one control group (Figure 1):
- (1)
Patients with confirmed infection by SARS-CoV-2, requiring hospitalisation in an intensive care unit.
- (2)
Patients with confirmed infection by SARS-CoV-2, requiring hospitalisation in a medicine unit.
- (3)
Patients with confirmed infection by SARS-CoV-2, not requiring hospitalisation.
- (4)
Individuals tested for SARS-CoV-2 infection, but who tested negative.
Written informed consent will be obtained from all included individuals. COVID-19 status will be assessed through Reverse Transcriptase-Polymerase Chain Reaction (RT-PCR). A positive serology for COVID-19 will be also considered. Participants enrolled in groups 1 and 2 will be recruited during their planned follow-up visits. Group 3 will be recruited from individuals who tested positive for COVID-19 but did not need hospitalization. This may include individuals who were asymptomatic or minimally symptomatic but were picked up through routine testing. The comparison between these three groups will provide insight into the role of disease severity in COVID-19-associated vascular damage, and to assess whether milder forms of COVID-19 are associated with evidence of vascular damage. Group 4, constituted by individuals who underwent testing for SARS-CoV-2 infection (RT-PCR testing or serology) but tested negative, represents the negative control group for this study. A negative control group is crucial in this study in order to confirm the study hypothesis, i.e., the presence of accelerated vascular ageing in COVID-19 survivors. Exclusion criteria are inability to provide written consent, pregnancy or breastfeeding, diseases carrying out a life expectancy of <1 year according to clinical judgment, or any other circumstance that would preclude full participation in the study.
Comparison with data from historical cohorts has been also planned, to consolidate acquired results against an unexposed group and to permit exploration of the effects of social measures to control spread of COVID-19 on EVA.
4.2. Schedule and Study Duration
Patients will attend for their first visit 6 ± 3 months after COVID-19 exposure, and a second one 12 ± 3 months thereafter. At both visits, CV measurements will be taken for all four groups (Figure 1). Questionnaires will be completed and outcomes and hospitalisations recorded at these visits, as well as 24, 48, and 120 months after recruitment. The duration of participation for each participant is thus 6 months for the main study and 10 years for the pre-planned study extension.
4.3. Measurements
To ensure a broad inclusion of centres, only a core set of measurements (carotid-femoral PWV, brachial and central blood pressure) is considered mandatory, whereas the majority of the measurements described below are optional but recommended (Figure 1). An overview of all measurements and parameters is given in Table 1.
| Measurement | Location | Derived parameters | Mandatory? |
|---|---|---|---|
| Applanation tonometry | Carotid, femoral | PWV; carotid PP* | Yes |
| Peripheral blood pressure | Brachial | SBP/DBP/MAP | Yes |
| Central blood pressure | Radial (recording site) | SBP/DBP; AP; AIx, AIx@75; RM; Pf; Pb | Yes |
| Ultrasound | Carotid | IMT; As; Ad; DC; PWVcar | No |
| Ultrasound | Brachial | FMD: Δd/d0; ΔQ/Q0 | No |
| Ultrasound | Cardiac | LVMI; E/e’; LAVI; TR; SV; CO; CI; proximal aortic As/Ad/DC | |
| Ultrahigh frequency ultrasound | Carotid, radial, digital | IMT; As/Ad/DC | No |
| 24-h blood pressure | Brachial, central | Brachial SBP/DBP/MAP; central SBP/DBP; AP; AIx, AIx@75; RM; Pf; Pb | No |
| Computed tomography | Thorax | Aortic calcification score; CAC | No |
| Questionnaires | – | SF-12; ISI; HADS; DSM-5; EPICES; CBS | No |
Carotid PP measurement is optional and to be used together with carotid ultrasound measurements to compute local carotid distensibility.
PP, pulse pressure; SBP/DBP, systolic/diastolic blood pressure; MAP, mean arterial pressure; AP, augmentation pressure; AIx, augmentation index; AIx@75, AIx normalised for a heart rate of 75 beats per minute; RM, reflection magnitude; Pf and Pb, absolute amplitude of the forward and backward wave; IMT, intima-media thickness; As/Ad, systolic and diastolic cross-sectional area; DC, distensibility coefficient; PWVcar, local carotid PWV; FMD, flow-mediated dilation; Δd/d0, relative flow-mediated diameter increase; ΔQ/Q0, relative flow increase; CAC, coronary artery calcium; LVMI, left ventricular mass index; E/e’, ratio between early mitral inflow velocity and mitral annular early diastolic velocity; LAVI, left atrial volume index; TR, tricuspid regurgitation; SV, stroke volume; CO, cardiac output; CI, cardiac index; SF-12, 12-item short form survey score; ISI, insomnia severity index; HADS, hospital anxiety and depression scale; DSM-5, diagnostic and statistical manual of mental disorders scale; EPICES, evaluation de la précarité et des inégalités de santé dans les centres d’examens de santé/evaluation of deprivation and inequalities in health examination centres; CBS, caregiver burden scale.
Overview of measured parameters
4.3.1. Carotid-femoral pulse wave velocity
Large artery stiffness will be assessed by carotid-femoral PWV [51]. Waveforms will be recorded at the femoral and carotid site, using validated devices, such as SphygmoCor (AtCor Medical, Sydney, NSW, Australia), Complior (Alam Medical, Vincennes, France), PulsePen (PulsePen, DiaTecne, Milan, Italy), or Vicorder (Skidmore Medical, Bristol, UK). Briefly, a probe or cuff is placed on the selected artery while 10–15 subsequent heartbeats are recorded. PWV is calculated from the pulse Transit Time (TT) using the 80% of direct distance method, as
4.3.2. Brachial blood pressure
Brachial blood pressure will be measured using a validated device according to the Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO) protocol [53]. Three measurements should be performed in the supine position at the non-dominant arm at intervals of 2 min after 10 min of rest. Blood pressure will also be measured in the supine posture directly before starting the PWV measurement.
4.3.3. Central blood pressure and micro-macrocirculation cross-talk
Peripheral pressure waveforms will be recorded from the radial artery at the wrist, using applanation tonometry with a high-fidelity tonometer. After 20 sequential high-quality waveforms have been acquired, a validated, Federal Drug Administration (FDA)-approved generalised transfer function will be used to generate the corresponding central aortic pressures and pressure waveforms (SphygmoCor). Waveforms will be calibrated with brachial mean and diastolic blood pressure. Blood pressure will be measured with a validated, automated, oscillometric, sphygmomanometer and mean blood pressure calculated as diastolic blood pressure + 0.4 * pulse pressure.
Augmentation Pressure (AP) — the difference between the second and first systolic peak will be determined. Augmentation Index (AIx) will be calculated as the ratio of AP to Pulse Pressure (PP), expressed as a percentage. In addition, an index normalised for a heart rate of 75 beats per minute (AIx@75) will be calculated.
Micro-macrocirculation cross-talk will be assessed by wave separation analysis [54]. The absolute amplitude of the antegrade and retrograde pressure waves will be quantified using the ARCSolver method [55] from measured pressure waveforms and modelled flow waveforms. Reflection magnitude, as well as absolute amplitude of the forward and backward wave, will be calculated.
4.3.4. Carotid ultrasound
Carotid ultrasound scans will be obtained by high-resolution B-mode ultrasound by a ≥7.5 MHz linear array transducer by a trained operator. The systolic and diastolic left and right carotid diameters will be automatically measured on the distal wall 1–2 cm proximal to the bifurcation by a real-time computerised contour tracking system “Cardiovascular Suite” (Quipu srl, Pisa, Italy). Cross-sectional Distensibility Coefficient (DC) will be estimated through the variations in arterial cross-sectional area and pulse pressure. DC will be calculated as
4.3.5. Carotid, radial, and digital ultrahigh frequency ultrasound
Carotid, radial, and digital remodelling (diameter and thickness) and distensibility will be assessed by ultrahigh frequency ultrasound by Vevo® MD (FUJIFILM VisualSonics Inc., Toronto, ON, Canada) in equipped centres. This high-frequency ultrasound machine is equipped with three probes operating at 22, 48, 70 MHz, with a spatial resolution of 100, 50, 30 μm, respectively. Edge detection and contour tracking techniques will be applied on high-resolution ultrasound images (Cardiovascular Suite, Quipu srl), in order to obtain arterial diameter, thickness and distensibility for each arterial site (as described above) [59].
4.3.6. Brachial artery flow-mediated dilation
Conduit artery endothelial function by brachial artery flow-mediated dilation and will include assessment of reactive hyperaemic response, a proxy for microvascular function, in equipped centres. This response will be assessed as increase of the artery diameter in response to increased blood flow [60]. The brachial artery will be imaged in longitudinal section, about 5 cm proximal to placement of a blood pressure cuff, just below the antecubital fossa. The probe (linear, >7.5 MHz) will be held in a stereotactic clamp to avoid movement artefacts. A Doppler flow signal will be recorded from the centre of the vessel with the range gate set at 1.5 mm. The baseline image and Doppler signal will be recorded for 1 min, following which a blood pressure cuff will be inflated to supra-systolic pressure for 5 min (300 ± 30 mmHg). The cuff will then be rapidly deflated and the artery imaged and Doppler signal recorded for 5 min post-cuff deflation. Brachial artery flow-mediated dilation is calculated as the maximum change in diameter from baseline, expressed as a percentage. On cuff deflation the resultant reactive hyperaemia is calculated as the flow change from baseline, expressed as a percentage change in blood flow using an automatic edge detection system (Cardiovascular Suite, Quipu srl).
4.3.7. Echocardiography
Participants will undergo standard echocardiograms at baseline and during follow-up, following standard recommendations [61–63] and according to each centre’s pre-specified protocol by expert sonographers. Left Ventricular (LV) Mass Index (LVMI) will calculated by Devereux’s formula and indexed to body surface area. The geometric classification will be based on the combination of LVMI and relative wall thickness. Transmitral peak E wave (pulse Doppler) and early diastolic Tissue Doppler velocity of mitral annulus (e’) will be used to assess LV diastolic function together with other parameters [E/e’, Left Atrial (LA) volume index, and peak Tricuspid Regurgitation (TR)]. Doppler echocardiography combined with two-dimensional imaging will be used to estimate Stroke Volume (SV), Cardiac Output (CO), and the cardiac index. Proximal aorta imaging (including M-mode images obtained from the parasternal long-axis view) will be used to assess the end-systolic aortic dimension and end-diastolic aortic dimension 2–3 cm above the aortic valve using the leading edge-to-leading edge technique. Using these measurements, aortic indices such aortic distensibility, strain and stiffness index will be estimated. In addition to standard echocardiography and when available in the participating centres, Global peak systolic Longitudinal Strain (GLS) will be assessed using 2D speckle tracking echocardiography.
4.3.8. 24-h brachial and central blood pressure
24-h brachial and central blood pressure will be measured using the Mobil-o-graph Pulse Wave Analysis (PWA) device (IEM GmbH, Stolberg, Germany). An appropriately sized cuff used for oscillometric reading is inflated at a pre-defined steady-state pressure level to obtain waveform signals which are analysed with proprietary methodologies. The central blood pressure measurement follows the brachial blood pressure assessment; brachial pressure waveforms are therefore auto-calibrated to brachial blood pressure values. The protocol for ambulatory blood pressure measurements will follow published recommendations [64].
4.3.9. Thoracic aortic calcifications
Assessment of presence or absence of thoracic aortic calcifications will be performed in any thoracic Computed Tomography (CT) scan available in the recruited population. The extent of aortic calcification will be assessed by a semi-qualitative method and will be defined as none, mild (1 sector [ascending, arch, descending]), moderate (>1 sector), or severe (>1 sector, concentric) [65]. Similarly, assessment of presence or absence of Coronary Artery Calcium (CAC) will be performed and the extent of CAC will be also assessed by a semi-qualitative method. CAC will be characterised as none, mild, moderate, or severe based on visual assessment that has been shown to be comparable to the Agatston score [66]. This information will be included in the baseline characteristics of the participants in the study. Further, quantitative assessment of arterial calcifications (coronary or/and thoracic) might be pursued as a post hoc analysis based on availability of baseline and follow-up scans.
4.3.10. Questionnaires
The following psychometric tests will be included:
- •
Quality of life (12-item short form survey, SF-12)
- •
Insomnia Severity Index (ISI)
- •
Hospital Anxiety and Depression Scale (HADS)
- •
PTSD questionnaires (PTSD checklist for DSM-5, PCL-5)
- •
Socio-economic status (evaluation de la précarité et des inégalités de santé dans les centres d’examens de santé/evaluation of deprivation and inequalities in health examination centres, EPICES)
- •
Chronic burden scale (CBS)
4.3.11. Mortality and hospitalisation records
All participants will be linked to relevant health surveillance, electronic heath record and mortality data in participating countries at visit 1. Follow up of these data is planned for visit 2, and at 2, 5 and 10 years after recruitment (Figure 1). Questionnaires to evaluate health status and psychometric tests will be also sent by email/mail.
4.4. Statistical Analysis
First, we will compare the trajectories of vascular ageing variables between COVID-19 patients and controls (group 4), and between COVID-19 patients with various degrees of severity, accounting for a set of fixed and time-varying confounders. This will be performed using mixed models suited for repeated assessments. Adjustment for age, sex, and mean arterial pressure will be performed. Further adjustment for classical CV risk factors (obesity, diabetes, renal function) will be performed if deemed necessary.
Second (mid-term/long-term), we will compare the risk of CV disease between the four groups. For this purpose, Cox proportional hazards regression will be performed, accounting for differences in trajectory of vascular ageing between infected and noninfected patients will be used.
Third, we will compare among infected patients: (a) the treatment/management practices (acute treatments for COVID-19, chronic renin-angiotensin system (RAS) blocker treatment); (b) the prevalence of pre-existing cardiovascular comorbidities; (c) the psychosocial characteristics, including PTSD; and (d) their potential impact on trajectory of vascular ageing and clinical events. To minimise indication bias in objective (d), propensity score analysis will be carried out.
Since COVID-19 is a completely new condition, sample size calculation cannot be based on preliminary data. However, we estimated that the minimal detectable difference in PWV between the control group and any of the other COVID-19 positive groups in a Dunnett’s test will be 0.35 m/s for a total population of 1500 participants, 0.3 m/s for 2000 participants, and 0.28 m/s for 2500 participants, given a standard deviation of 1.2 m/s, α = 0.05, a global statistical power (1-β) of 0.80, and 10% of subjects lost to follow-up.
5. ETHICAL CONSIDERATIONS
The CARTESIAN study is a research study involving human participants with minimal risks and burden. Accordingly, it cannot be carried out on a person without his/her freely given and informed consent, obtained expressly after the person has been given the information. An adequate reflection period will be given to the individual between the time when he or she is informed and when he or she signs the consent form. A copy of the information sheet and consent form, signed and dated by the research participant and by a study investigator, will be given to the individual prior to their participation in the study. This research concerns only people physically able to give her/his written consent. Given the real-life nature of this study, no prohibition from participating in another clinical study or exclusion period after the study is foreseen.
6. DATA COLLECTION AND MANAGEMENT
Data will be held centrally in the European coordinating centre (Institut national de la santé et de la recherche médicale - INSERM U970, Paris France). An electronic Case Report Form (eCRF) is set up (RedCAP) via a web browser. The eCRF used for this research is implemented in accordance with European (General Data Protection Regulation) regulations.
INSERM will be responsible for data hosting and management. A data transfer agreement will be signed between INSERM and study promoter in order to authorise INSERM to secured data storage and management. INSERM will send to the study promoter a cleaned database version, via secured electronic transfer. Ownership of any data transferred to the eCRF and centralized database will be retained by the site that contributed it. All analysis of pooled data will be undertaken with the explicit agreement of each contributing site. Research data will be shared with public health authorities as needed.
7. CONCLUSION
There is strong reason to believe that COVID-19 has long-term consequences for arterial structure and function, and thus for CV prognosis in survivors. Therefore, in this paper, we present the protocol of a large multi-centre prospective study investigating the effects of COVID-19 on EVA. Although this protocol details many measurements, we took great care to ensure that only the core ones are mandatory, ensuring inclusiveness for as many centres as possible. At the time of writing (10 November 2020), 43 centres from 21 countries had expressed interest in participating (Figure 2) with a total expected number of >2500 included patients. A list of centres that have obtained Ethics Committee approval/started recruitment is provided in Supplemental Table S1 in Supplemental Digital Content 1.
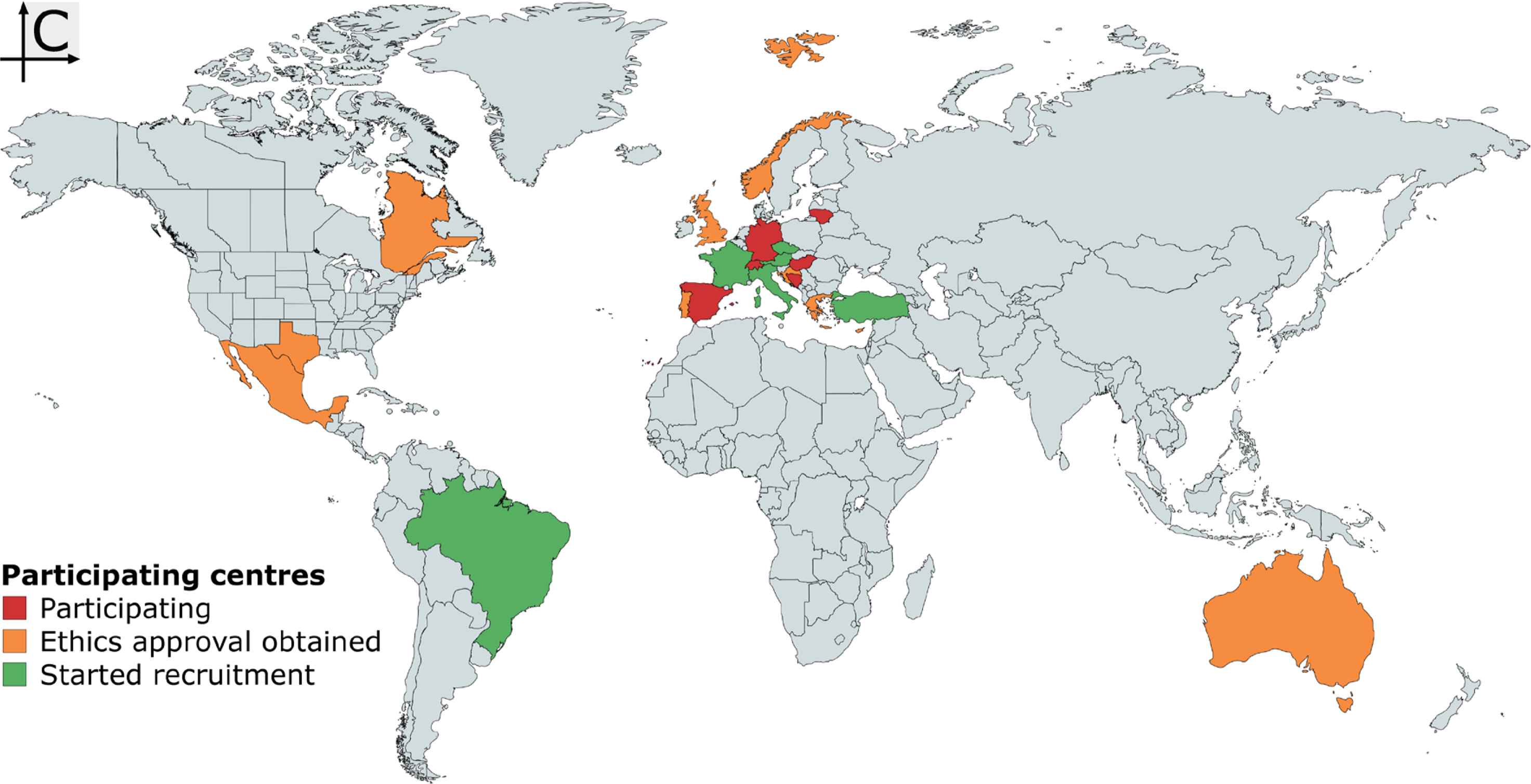
Map of participating centres as of 10 November 2020. Map created with mapchart.net.
In summary, data from the CARTESIAN study should provide insight in the relationship between COVID-19, its severity, and early vascular ageing in a large cohort. To our knowledge, this will be the first study to provide such insight, potentially enabling future care and diagnostics to be more focused on those most affected.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
RMB and BP contributed in study conceptualization and writing (original draft, review & editing) the manuscript. BH, PL, CCM, MLM, CR, DTP, TW and TWH contributed in review & editing. PB supervised the project.
FUNDING
The CARTESIAN study is supported by a grant from the
SUPPLEMENTARY MATERIAL
Supplementary data related to this article can be found at
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Rosa Maria Bruno AU - Bart Spronck AU - Bernhard Hametner AU - Alun Hughes AU - Patrick Lacolley AU - Christopher C. Mayer AU - Maria Lorenza Muiesan AU - Chakravarthi Rajkumar AU - Dimitrios Terentes-Printzios AU - Thomas Weber AU - Tine Willum Hansen AU - Pierre Boutouyrie AU - on behalf of the ARTERY Society PY - 2020 DA - 2020/12/08 TI - Covid-19 Effects on ARTErial StIffness and Vascular AgeiNg: CARTESIAN Study Rationale and Protocol JO - Artery Research SP - 59 EP - 68 VL - 27 IS - 2 SN - 1876-4401 UR - https://doi.org/10.2991/artres.k.201124.001 DO - 10.2991/artres.k.201124.001 ID - Bruno2020 ER -