
Sickle cell disease in Saudi Arabia: A challenge or not
- DOI
- 10.1016/j.jegh.2016.12.006How to use a DOI?
- Copyright
- © 2017 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Sickle cell disease (SCD) is an autosomal recessive disorder that is common in Sub-Saharan Africa, the Mediterranean basin, and Saudi Arabia [1]. However, this condition also threatens the health of many people globally. According to the World Health Organization, Africa has the highest prevalence of SCD, which ranges from 10% to 40%. Moreover, in countries where the trait prevalence is >20%, the disease affects approximately 2% of the population [1]. However, 7% of the population of the world are carriers of hemoglobinopathies, which are carried by approximately 2,000,000 Americans, and are clinically diagnosed in approximately 72,000 Americans [2].
Patients with SCD usually exhibit multiple organ damage because of repeated vascular occlusion, which is superimposed on a background of poor development and failure to thrive. Many patients have frequent hospital admissions for their condition, and may experience episodes of chronic pain, fatigue, hand-foot syndrome, frequent infections, delayed growth, and vision problems [3]. Furthermore, many patients with SCD face a shortened life expectancy, and a number of recurring, debilitating, and expensive health conditions. Thus, the demands for health services are increasing because of the increasing incidence of SCD, which is related to limitations in the number of trained health professionals, effective vaccines and medicines, specialized healthcare facilities, and safe blood transfusions [4]. Therefore, it is important to consider whether Saudi Arabia is equipped to address the significant burden of SCD in our country, and to make efforts to reduce the morbidity and mortality that is associated with this disease.
2. Current burden in Saudi Arabia
Genetic disorders, such as SCD, are very common in Saudi Arabia [2,5]. Unfortunately, although the prevalence of SCD has been decreasing in every region of Saudi Arabia, the prevalence remains higher than that in other countries (Figs. 1 and 2). Moreover, SCD is endemic in southern and eastern Saudi Arabia, which indicates that current Saudi efforts to address this disease remain insufficient. The first reported case of SCD in the eastern province was reported in the 1960 s [2,4], and the prevalence in this province is 145 cases/10,000 population, which is much higher than the prevalence in the southern region (24 cases/10,000 population), western region (12 cases/10,000 population), and central region (6 cases/10,000 population) [6]. Moreover, approximately 2–27% of the population are SCD trait carriers [2], and the Saudi Premarital Screening Program estimates that 0.26% of the adult population are trait carriers, and that 4.2% of the population is affected by SCD [2].
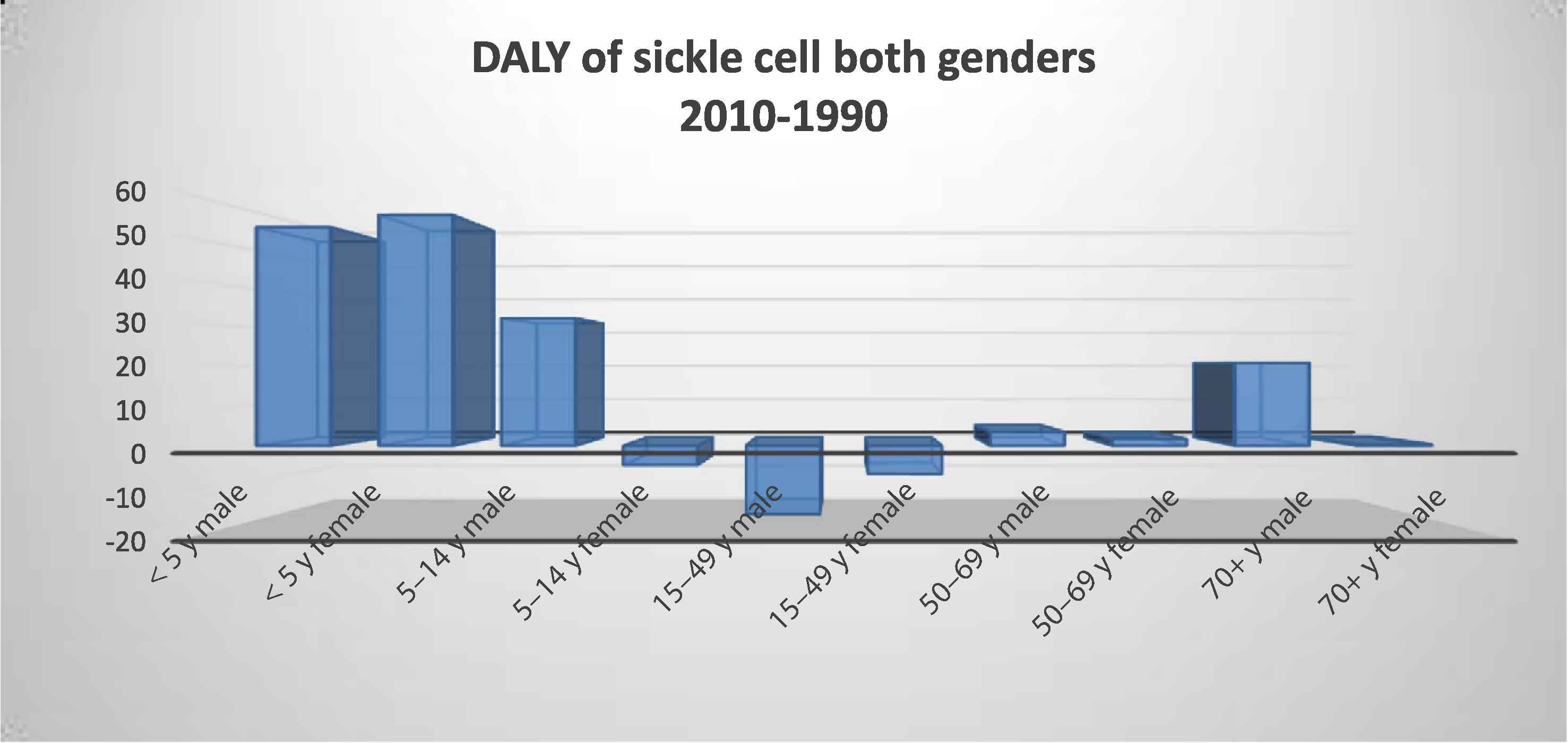
Saudi Arabia sickle cell percent of total disability-adjusted life year (both genders).
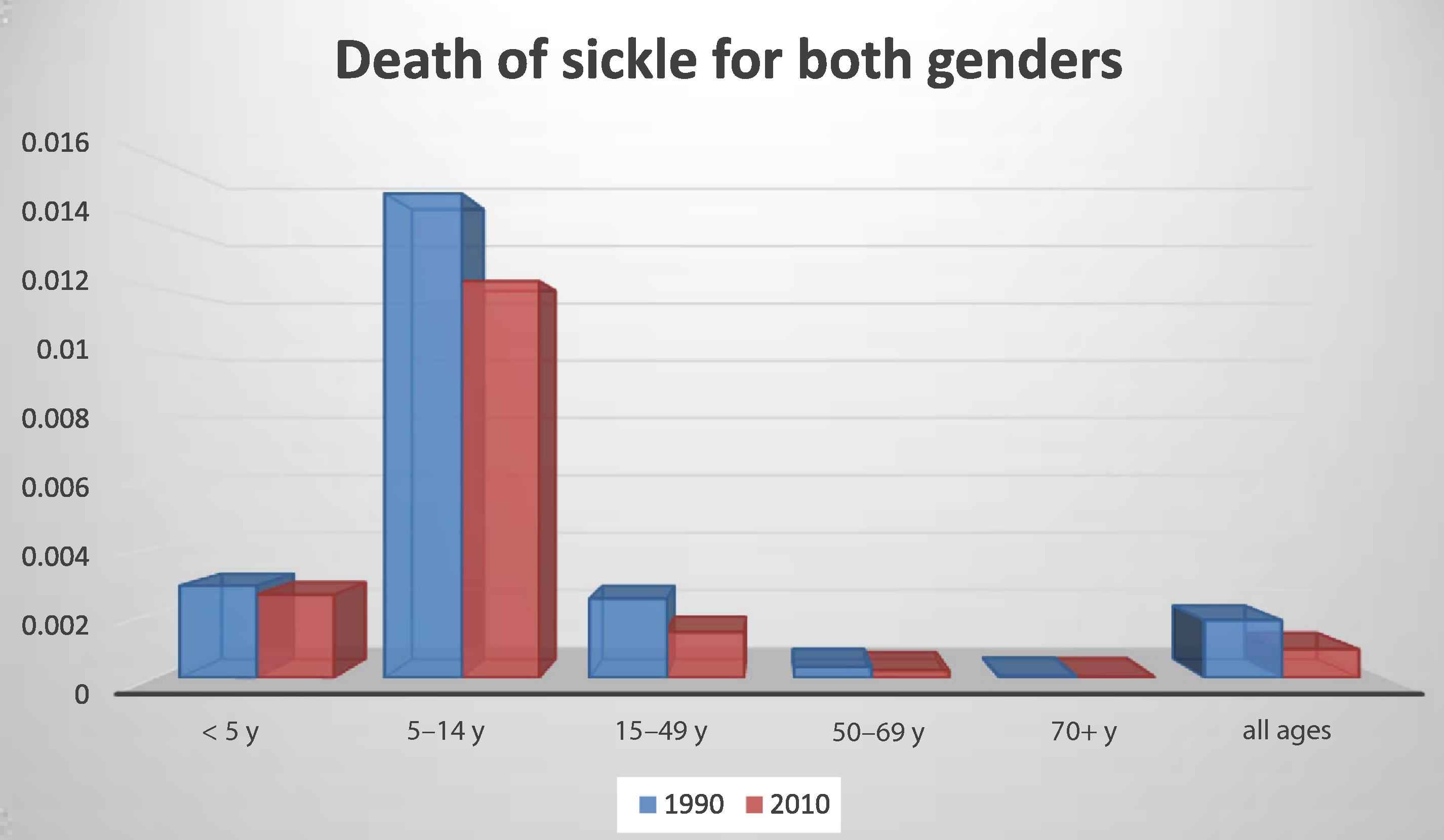
Saudi Arabia sickle cell percent of total death (both genders).
Saudi Arabia faces numerous challenges in controlling SCD. One of the major challenges is the prevalence of consanguineous marriages (57.7%), and this prevalence can increase to >80% in certain rural areas [7]. As these marriages increase the risk of genetic diseases, the Saudi government is trying to educate people regarding the effects of consanguineous marriages through awareness programs. The most successful programs that have been implemented by the government are the Premarital Screening Program and the Genetic Counseling Program. The Premarital Screening Program is mandatory for all couples, and is provided free at all government facilities. This program appears to be successful, as it has significantly reduced the number of voluntary cancelations of at-risk marriage proposals by 60%, which has increased by 5-fold over 6 years [5].
3. Opportunities for control and intervention
Early intervention at the newborn stage, and the Saudi Premarital Screening Program, may be useful for controlling and preventing SCD. Furthermore, primary and secondary prevention can be improved through the training of health professionals, development of genetic counseling and testing protocols, and increasing the geographical and financial accessibility of healthcare services. Moreover, developing countries (such as Saudi Arabia, which has a high burden of SCD) should be encouraged to increase public awareness in schools, communities, health institutions, the media, and medical associations; and to establish patient support groups, advocacy, and policies regarding employment for patients with SCD [1].
Although the Premarital Screening Program and free genetic counseling have been very effective in the Saudi population, Saudi Arabia must also implement other effective programs for identifying new cases of SCD (e.g., through newborn screening). For example, parental counseling and follow-up care for affected cases have reduced SCD-related morbidity and mortality in other countries [3]. However, Saudi patients experience several barriers to genetic counseling and screening, such as limited access to health services, few trained healthcare professionals, social and cultural stigmas, and religious beliefs. Therefore, Saudi Arabia must implement awareness programs at a very early age to help the population overcome these barriers.
There is also very little genetic research regarding SCD in Saudi Arabia, and interventional studies are needed to evaluate the effectiveness of population-based strategies and interventions. Based on the success of the Premarital Screening Program and free genetic counseling, the Saudi government should focus on promoting newborn screening at the national level, which may help reduce the primary and secondary burdens of SCD. Moreover, it would be useful to maintain an up-to-date registry for estimating the actual burden of SCD.
4. Conclusion
In conclusion, the burden of SCD is high in Saudi Arabia, which is likely related to the high prevalence of consanguineous marriages. Although genetic screening and counseling services (e.g., the Premarital Screening Program) are effective in the Saudi population, the long-term benefits will be observed only over time. Therefore, national preventative strategies are needed, such as promoting newborn screening, improving access to health services, training health professionals, increasing awareness at a very early age, and the development of population-based research and an up-to-date SCD registry. These steps may help reduce the burden of SCD at the primary and secondary levels.
Conflicts of interest
The author declares no conflicts of interest.
References
Cite this article
TY - JOUR AU - Maha Mohammed Alotaibi PY - 2017 DA - 2017/02/28 TI - Sickle cell disease in Saudi Arabia: A challenge or not JO - Journal of Epidemiology and Global Health SP - 99 EP - 101 VL - 7 IS - 2 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2016.12.006 DO - 10.1016/j.jegh.2016.12.006 ID - Alotaibi2017 ER -