
Suicide rate in relation to the Human Development Index and other health related factors: A global ecological study from 91 countries
- DOI
- 10.1016/j.jegh.2016.12.002How to use a DOI?
- Keywords
- Ecological study; Human Development Index; Suicide
- Abstract
There has been no worldwide ecological study on suicide as a global major public health problem. This study aimed to identify the variations in suicide specific rates using the Human Development Index (HDI) and some health related variables among countries around the world. In this ecological study, we obtained the data from the World Bank Report 2013. The analysis was restricted to 91 countries for which both the epidemiologic data from the suicide rates and HDI were available. Overall, the global prevalence of suicide rate was 10.5 (95% confidence intervals: 8.8, 12.2) per 100,000 individuals, which significantly varied according to gender (16.3 in males vs. 4.6 in females, p < 0.001) and different levels of human development (11.64/100,000 individuals in very high development countries, 7.93/100,000 individuals in medium development countries, and 13.94/100,000 individuals in high development countries, p = 0.004). In conclusion, the suicide rate varies greatly between countries with different development levels. Our findings also suggest that male gender and HDI components are associated with an increased risk of suicide behaviors. Hence, detecting population subgroups with a high suicide risk and reducing the inequality of socioeconomic determinants are necessary to prevent this disorder around the world.
- Copyright
- © 2017 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Suicide is a major public health problem with considerable variation within and between countries [1]. It accounted for 0.5–1.4% of all deaths worldwide [2]. By contrast, in 2013, suicide resulted in 842,000 deaths [3]. Globally, suicide is the 15th leading cause of death in all ages [4] and the fourth in ages of 15–44 years [5]. In addition, for each successful suicide attempt, there are 10–40 failed suicide attempts as well [6]. Reports of the World Health Organization (WHO) showed that 85% of the world’s suicide rates occur in low- and middle-income countries [7], while this is increasing especially in developing countries.
Many studies have shown that several factors such as hopelessness, mental disorders, alcoholism, or drug abuse, as well as stressful events such as financial problems and interpersonal communication difficulties are associated with suicide behavior [5,8,7,9]. In addition, some socioeconomic conditions such as unemployment, poverty, and homelessness may increase the risk of suicide [10,11].
In high-income countries, social factors such as socioeconomic position (SEP) have an important role in suicide risk [12]. Knowledge of effective SEP factors on the risk of suicide and suicide attempt is important to improve public health policy notifications and plan for effective prevention programs. By contrast, inequality in the socioeconomic determinants can reflect regional imbalances in human development [13]. However, there has been no ecological study on the matter across the world. Unequal distribution of the Human Development Index (HDI) as a proxy for SEP in the countries has not been investigated yet and there have been widely conflicting findings regarding the direction of association between socioeconomic status and suicide rates. This study aimed to identify the variations in suicide specific rates by HDI and some health-related variables among different countries around the world.
2. Materials and methods
2.1. Study design
This ecological study was performed on the relationship of suicide rate with the HDI and other health-related variables in 2015. We obtained the data from the World Bank Report 2013 [14] including: the HDI, urbanization (% of population), total fertility rate (births per woman), unemployment rate (% aged ⩾ 15 years), age-standardized obesity rate among adults, and also suicide rate within different countries. Suicide rate was considered as the main outcome.
2.2. Measures
HDI has several main components that include: life expectancy at birth, mean years of schooling, expected years of schooling, and gross national income (GNI) per capita (20011 US dollars at purchasing power parity – 2011 PPP$).
The analysis was restricted to countries for which both the epidemiologic data from the suicide rate and HDI were available (91 countries). Because data about suicide rate for low HDI countries were not available, we categorized countries into three predefined categories: medium (0.5 ⩽ HDI < 0.8), high (0.8 ⩽ HDI < 0.9), and very high (HDI ⩾ 0.9). Therefore, the categorization resulted in very high human development (10), high human development (33), and medium human development (48) countries.
2.3. Data analysis
Comparison of suicide rates by gender and HDI components between various HDI categories (very high, high, and medium) were done using a one-way analysis of variance. Also, we used the Pearson correlation coefficient for assessment of the correlation between the suicide rate among men and women and some health-related variables. All analyses were conducted at 95% significant level using Stata software version 12 (StataCorp, College Station, TX, USA).
3. Results
Overall, the global prevalence of suicide rate was 10.5 (95% confidence intervals: 8.8, 12.2) per 100,000 individuals, while it significantly varied according to gender (16.3 in males vs. 4.6 in females, p < 0.001) and different categories of human development (p = 0.004). Additional information about suicide rates is shown in Table 1.
| Region | SR | p | HDI component | Total suicide rate | ||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||
| Females | Males | LEB | MYS | GNI | EYS | |||
| Very high human development | 6.25 | 16.94 | <0.001 | 81.2 | 12.25 | 86,665 | 17.15 | 11.65 |
| High human development | 6.22 | 21.52 | <0.001 | 79.1 | 10.85 | 32,141 | 15.87 | 13.94 |
| Medium human development | 3.12 | 12.66 | <0.001 | 72.3 | 8.78 | 11,846 | 12.92 | 7.93 |
| p (F-test) | <0.001 | 0.010 | – | <0.001 | <0.001 | <0.001 | <0.001 | 0.004 |
EYS = expected years of schooling; GNI = gross national income per capita; LEB = life expectancy at birth; MYS = mean years of schooling; SR = suicide rate (per 100,000 populations).
Female and male suicide rates and Human Development Index (HDI) component by different HDI regions in 2012.
Table 2 and Fig. 1 show the correlations between female and male suicide rates and health-related variables. There was a negative significant correlation between total suicide rate with total fertility rate (r = −0.462, p < 0.001) and age-standardized obesity rate among adults (r = −0.240, p = 0.024). After stratifying by sex, there was a positive correlation between female suicide rate and urbanization (r = 0.23, p = 0.030), GNI (r = 0.31, p = 0.003), and life expectancy at birth (r = 0.21, p = 0.040), while a negative significant correlation was shown with total fertility rate (r = −0.42, p < 0.001), unemployment rate (r = −0.23, p = 0.030), and age-standardized obesity rate among adults (r = −0.41, p < 0.001). More specifically, the male suicide rate was inversely correlated with total fertility rate (r = −0.46, p < 0.001).
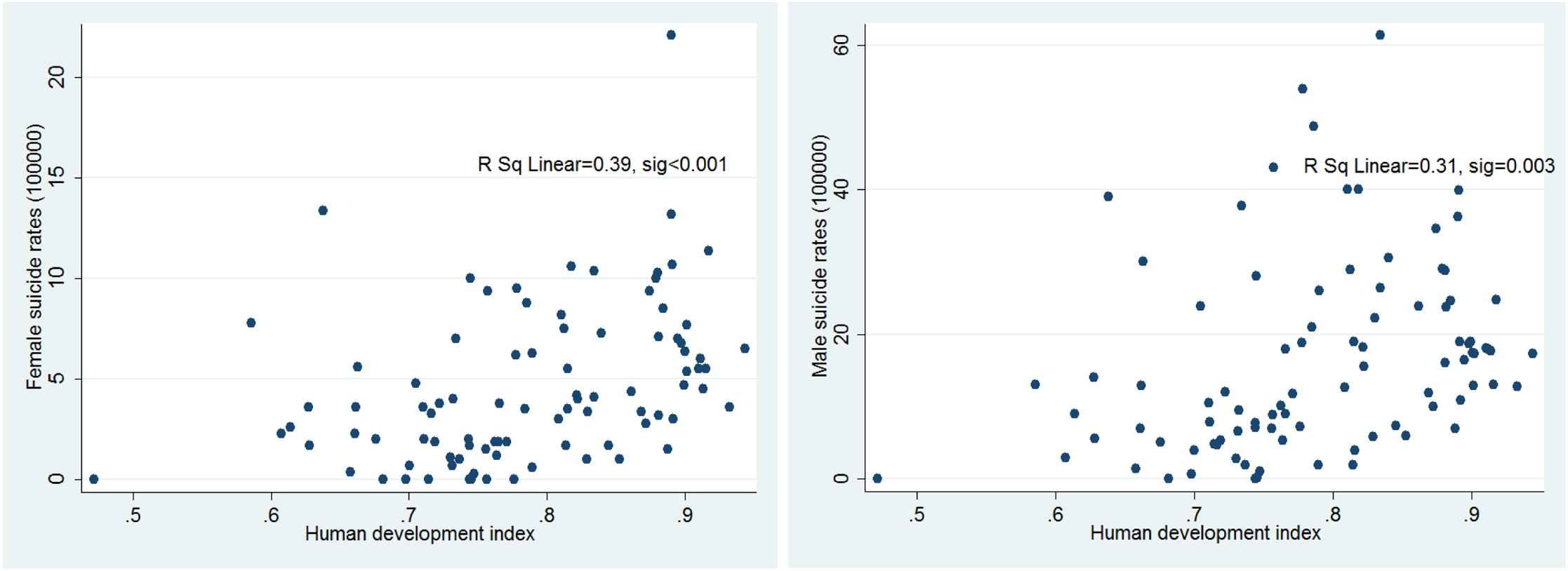
Correlation between the Human Development Index and female and male suicide rates per 100,000.
| Urbanization level (%) | Total fertility rate | Gross national income | Life expectancy at birth | Un employment rate | Obesity rate among adults | |
|---|---|---|---|---|---|---|
| Female suicide rate | 0.23 | −0.42 | 0.31 | 0.21 | −0.23 | −0.41 |
| p | 0.030 | <0.001 | 0.002 | 0.040 | 0.030 | <0.001 |
| Male suicide rate | 0.11 | −0.46 | 0.16 | 0.007 | −0.16 | −0.18 |
| p | 0.310 | <0.001 | 0.140 | 0.947 | 0.130 | 0.094 |
| Total suicide rate | 0.139 | −0.462 | 0.200 | 0.055 | −0.190 | −0.240 |
| p | 0.188 | <0.001 | 0.057 | 0.606 | 0.085 | 0.024 |
Correlations between female and male suicide rates and health related variables.
4. Discussion
This study was conducted to determine the association between HDI levels and the incidence of suicide in different countries. The results of this study showed that suicide rates increased with increasing levels of HDI, and were higher in men compared to women. There was a direct and significant correlation between incidence of suicide with percentages of urbanization of countries, GNI, and life expectancy in women. There was also a significant inverse correlation between suicide and total fertility rate (both in men and women), unemployment rate, and the rate of obesity in adults only in women.
Our results demonstrated that suicide was higher in men compared to women. Other studies have reported similar results [15,16]. One explanation for the higher rate of successful suicide attempts in men could be attributed to the fact that men usually use more lethal methods for taking their lives. Furthermore, women are less likely to become alcoholic and they also tend to have stronger religious orientations. More resilience, social support, and better compliance for mental disorder treatments among women are regarded as the explanations for more failed suicide attempts [12]. In contrast, men have more responsibility for financing the family and are more likely to develop psychological stress [17].
Our results showed a significant direct correlation between HDI levels of countries and the incidence of suicide. Results of similar studies are contradictory. While some studies have shown an inverse relationship between income levels (as a component of HDI) and suicide rate [18–21], other studies have reported otherwise [22]. This paradox may be due to the effect of other confounding factors such as religion and race in different societies. The use of different scales to measure socioeconomic status, type of study design, and population size could also partly explain this contradiction.
Unemployment and the presence of women in the home are associated with lower suicide rates. Working populations usually have more access to the means for suicide attempts. Thus, the highest suicide rate has been shown in professional vocations such as veterinarians, physicians, and farmers who have easy access to drugs and toxins [23]. Job-related stress can provide an incentive to commit suicide as well [24], although a systematic review revealed that unemployment was associated with suicidal behaviors [25]. One reason could explain our result; the secondary aggregated data which were used in the study may cause the Simpson’s paradox issue [26].
The results of this study showed that increases in life expectancy were associated with increasing suicide rates. Typically, suicide rates increase with age. The elderly usually use lethal methods for suicide and consequently the rate of successful suicide among them is high [27]. Secrecy of attempting suicide, as well as retirement problems, social isolation, and increased probability of morbidities are different reasons for this elevated rate in the elderly.
A positive relationship between percentage of urbanization and incidence of suicide in this study can be argued through massive migrations of rural residents to urban areas. These people in the new environment are socially isolated and have less access to health services and welfare. Therefore, they are more likely to commit suicide. Results of a meta-analysis showed an increase in suicide rate among immigrants compared to indigenous populations [28].
Increase in the total fertility rate is due to the increase in marriages. Several studies have shown that single individuals are more susceptible to suicide attempts [29,30]. The results of a study of 12 developed countries from America, Europe, and Australia suggest a protective role of marriage in both men and women regarding suicide [31]. Another study in the USA to obtain the association between suicide mortality and family structure indicated that family extension had a protective role against the rate of suicide [32].
This study had several limitations. We performed an ecological analysis using the global data from 91 countries. Although using the global data with consistent definition facilitates the comparisons across countries, there cannot be any individual-level interpretation. Another important limitation was the lack of data about suicide rates for low HDI countries, as well as some under-reporting of suicide rates in some other countries. These issues may raise selection and information biases, respectively. Hence, further studies addressing these issues, especially in the aforementioned regions, are imperative. Despite the limitations, this study provides the first evidence on the relationship between suicide rates and HDI worldwide which may help to fill a gap in the literature.
5. Conclusion
The suicide rate varies greatly between countries with different development levels. Our findings also suggest that male gender and HDI components are associated with increased risk of suicide behaviors. Hence, detecting population subgroups with a high suicide risk and reducing the inequality of socioeconomic determinants are necessary to prevent this disorder around the world. Governors will need to focus on community-based programs and equal distribution of economic resources to reduce the suicide rates. Further longitudinal studies are warranted to assess the socioeconomic factors on reducing national and regional suicide rates.
Conflicts of interest
None declared.
References
Cite this article
TY - JOUR AU - Salman Khazaei AU - Vajihe Armanmehr AU - Shahrzad Nematollahi AU - Shahab Rezaeian AU - Somayeh Khazaei PY - 2017 DA - 2017/02/07 TI - Suicide rate in relation to the Human Development Index and other health related factors: A global ecological study from 91 countries JO - Journal of Epidemiology and Global Health SP - 131 EP - 134 VL - 7 IS - 2 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2016.12.002 DO - 10.1016/j.jegh.2016.12.002 ID - Khazaei2017 ER -