
Prevalence of rifampicin-resistant Mycobacterium tuberculosis among human-immunodeficiency-virus-seropositive patients and their treatment outcomes
- DOI
- 10.1016/j.jegh.2017.09.002How to use a DOI?
- Abstract
Multidrug resistant (MDR) and extensively drug resistant tuberculosis (TB) are a threat to the TB control programs in developing countries, and the situation is worsened by the human immunodeficiency virus (HIV) pandemic. This study was performed to correlate treatment outcome with the resistance patterns in HIV-seropositive patients coinfected with pulmonary TB. Sputum specimens were collected from 1643 HIV-seropositive patients and subjected to microscopy and liquid culture for TB. The smear- and culture-positive Mycobacterium tuberculosis isolates were subjected to Genotype MTBDRplus assay version 2.0. The M. tuberculosis culture-positivity rate was 39.44% (648/1643) among the 1643 HIV-seropositive patients and the overall MDR-TB rate was 5.6% (36/648). There were 421 newly diagnosed and 227 previously treated patients, among whom, MDR-TB was associated with 2.9% and 10.57% cases, respectively. The rate of rifampicin monoresistant TB among the cases of MDR-TB was 2.31% (15/648) and the rate of combined rifampicin and isoniazid resistance was 3.24% (21/648). The cure and death rates among the 20 registered cases were 30% (6/20) and 35% (7/20), respectively. Five cases were on treatment and two cases were defaulters among the 20 registered cases. High death rate (13, 36.1%, 95% confidence interval 20.8–53.8) was observed in this study among the patients who had mutations at the 530–533 codons. The present study emphasized the prerequisite to monitor the trend of drug-resistant TB in various mutant populations in order to timely implement appropriate interventions to curb the threat of MDR-TB.
- Copyright
- © 2017 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
The convoluted linkage of tuberculosis (TB) and human immunodeficiency virus (HIV) infection for nearly the past three decades poses a major threat to the international community. Globally, the numbers of HIV-infected persons estimated to have associated (usually latent) infection with Mycobacterium tuberculosis vary from 14% in Europe to 46% in Southeast Asia [1]. Nearly one of three TB-related deaths (29%) worldwide is considered to be related to HIV infection, and TB contributes to 26% of the estimated deaths due to HIV infection [2]. India has the highest burden of TB globally and the third largest number of people living with HIV; it also ranks third in the world for HIV-associated TB. An estimated 120,000 HIV-positive TB cases have occurred in 2.1 million HIV-positive cases in India [3]. The distribution of HIV-associated TB closely follows the spread of the HIV epidemic. In 2013, 44,604 patients with HIV-associated TB were detected through HIV testing of TB patients and intensified case finding at HIV care and treatment centers. However, this represents only about 35% of the estimated burden in India. Currently, the six highest HIV prevalence states contribute about 75% of the detection. Thus, a gap exists in detection of HIV-associated TB across the country, but particularly more in historically low HIV prevalence states [4–6]. While TB is endemic across India, the HIV epidemic is concentrated in six out of 35 states and union territories in the country including Andhra Pradesh, Karnataka, Maharashtra, Tamil Nadu, Manipur, and Nagaland. These states have a HIV prevalence of around 1% among pregnant women attending the antenatal clinics. The burden of HIV-associated TB closely follows the distribution of the HIV epidemic in the country, and >75% of patients with HIV-associated TB are located in just the six states mentioned above [7].
Diagnosis of active TB disease in HIV-infected persons is difficult, as the patients with HIV-associated TB have fewer bacilli in their sputum [8] than do HIV-uninfected patients with pulmonary TB. In addition, it has been observed that presence of a cough for 13 weeks is not sensitive enough on its own as a symptom of TB in HIV-infected patients [9]. Since diagnosis in most regions depends on microscopic examination of Ziehl-Neelsen-stained sputum smears, which has low sensitivity among HIV-infected persons, most HIV-infected patients are not tested with the standard diagnostic methodology. The specific impact of methods that optimize the use of smear microscopy, such as sputum processing (liquefaction or concentration through sedimentation) and the use of fluorescence microscopy is not well understood for HIV-infected persons. Mycobacterial culture is the gold standard for TB diagnosis and is now routinely recommended to assist the diagnosis of TB in HIV-infected patients [10], although it is slow.
People with HIV are increasingly infected with TB because HIV weakens their immune system [11]. HIV/AIDS fuels the TB epidemics in many ways, such as promoting progression to active TB, increasing the risk of reactivation of latent TB infection, as well as increasing the chance of TB once exposed to M. tuberculosis [12,13]. The emergence of multi-drug resistant (MDR)-TB further complicates the situation and threatens to jeopardize all the prior gains by global TB control programs in recent years. The situation of TB is further threatened by the devastating effect of HIV on TB susceptibility, and the rapid expansion of MDR-TB threatens to undermine the advances made by TB management programs [14]. The prevalence of MDR-TB in HIV patients in care and receiving treatment in Puducherry is not known. In the setting of an intensive TB screening program using molecular assays, mycobacterial culture, and drug susceptibility testing for all patients, our objectives were to assess the prevalence of antibiotic-resistant TB, and to describe the resistance patterns in TB patients commencing antiretroviral therapy in attending care and treatment clinic in Puducherry, South India.
2. Materials and methods
The study was retrospectively carried out from October 2012 to December 2015 for a span of 39 months. Sputum samples of HIV-seropositive patients were received through a cold chain mechanism from eight medical colleges, government hospitals, and primary health centers in Puducherry State and were assigned laboratory numbers to process the samples in the Intermediate Reference Laboratory at the Government Hospital for Chest Diseases. The study was done in a blinded manner in which the clinical diagnosis was not available to the laboratory personnel. Approximately 1643 sputum samples from various age groups included 59 ≤ 15 years, 1158 > 15 years to ≤45 years, 378 > 45 years to ≤60 years, and 48 > 60 years (Table 1). The smear-positive samples in fluorescence microscopy were directly processed by GenoType MTBDRplus assay version 2.0 (Hain Lifescience, Nehren, German [15]) and all the samples were processed in the BACTEC MGIT 960 system. The culture-positive tubes of smear negative samples were also processed for the by GenoType MTBDRplus assay version 2.0.
| Name of state and Referring Center | Patient age | |||
|---|---|---|---|---|
| ≤15 y | >15 y to ≤ 45 y | > 45 y to ≤ 60 y | > 60 y | |
| Puducherry | 22 | 128 | 45 | 3 |
| Tamil Nadu | 37 | 1002 | 322 | 45 |
| Referral of Medical Colleges | – | 28 | 11 | – |
| Total | 59 | 1158 | 378 | 48 |
Details of multidrug-resistant suspect samples among the human-immunodeficiency-virus-seropositive cases in different geographical areas.
2.1. Sputum smear microscopy
As soon as the sputum samples were received at the Intermediate Reference Laboratory, they were decontaminated and concentrated by the standard N-acetyl-l-cysteine-NaOH method [16]. The deposits were used for smear preparation and air-dried slides were subjected to fluorescent staining. The stained slides were scanned by fluorescence microscopy at 40× magnification [17].
2.2. Primary culture inoculation and identification of mycobacterial species
All sputum specimens were digested and decontaminated by the standard N-acetyl-l-cysteine-NaOH method [16]. The sediment was suspended in 1 mL sterile phosphate-buffered saline (pH 6.8) and 0.5 mL of the processed specimen was inoculated into MGIT 960 vials supplemented as described by the manufacturer [18]. All inoculated MGIT tubes were incubated in the MGIT 960 instrument either until they were flagged positive by the instrument or for a maximum of 6 weeks. All positive MGIT vials were confirmed for acid-fast bacilli by Ziehl-Neelsen staining and further subjected to identification of M. tuberculosis complex by the para-nitrobenzoic acid assay. Some of the processed specimens was refrigerated for further use and to rule out discrepant results. Species identification was based on observation of cultural characteristics and biochemical tests. Procedures were adopted to differentiate mycobacteria at species level only [19].
2.3. GenoType MTBDRplus assay version 2.0
The GenoType MTBDRplus version 2.0 assay testing was accomplished in accordance with the manufacturer's recommendations and the manufacturer-trained laboratory staff members. The test is based on DNA strip technology and has three steps: DNA extraction, multiplex PCR amplification, and reverse hybridization [20,21]. All three steps were performed as per the World Health Organization recommendations [22,23].
3. Results
Sputum specimens were obtained from a total of 1643 patients clinically suspected of pulmonary TB prospectively enrolled in this study. There were 1099 (66.89%) men and 544 (33.11%) women. Patients of all age groups were enrolled, and most patients (1158; 70.48%) were aged 15–45 years, however, there was no significant preponderance of TB in any specific age group (Table 1).
The sputum smear positivity rate was 39.81% (654 of 1643 samples) and culture positivity by liquid culture was 40.9% (672 of 1643 samples). Among the positive cultures, there were 648 (39.44%) isolates of M. tuberculosis and 24 (1.46%) isolates of nontuberculous mycobacteria (Fig. 1). The 648 isolates of M. tuberculosis were subjected to Genotype MTBDRplus assay version 2.0. Among the 648 culture-positive M. tuberculosis isolates there were 421 newly diagnosed cases that had never received treatment for TB or had taken anti-TB treatment for <1 month, while 227 patients gave a history of previous anti-TB treatment for >1 month, of which 59 were treatment failures, 31 relapses after treatment, 18 defaulters during treatment, and 119 patients who did not provide sufficient history to be categorized into any group.
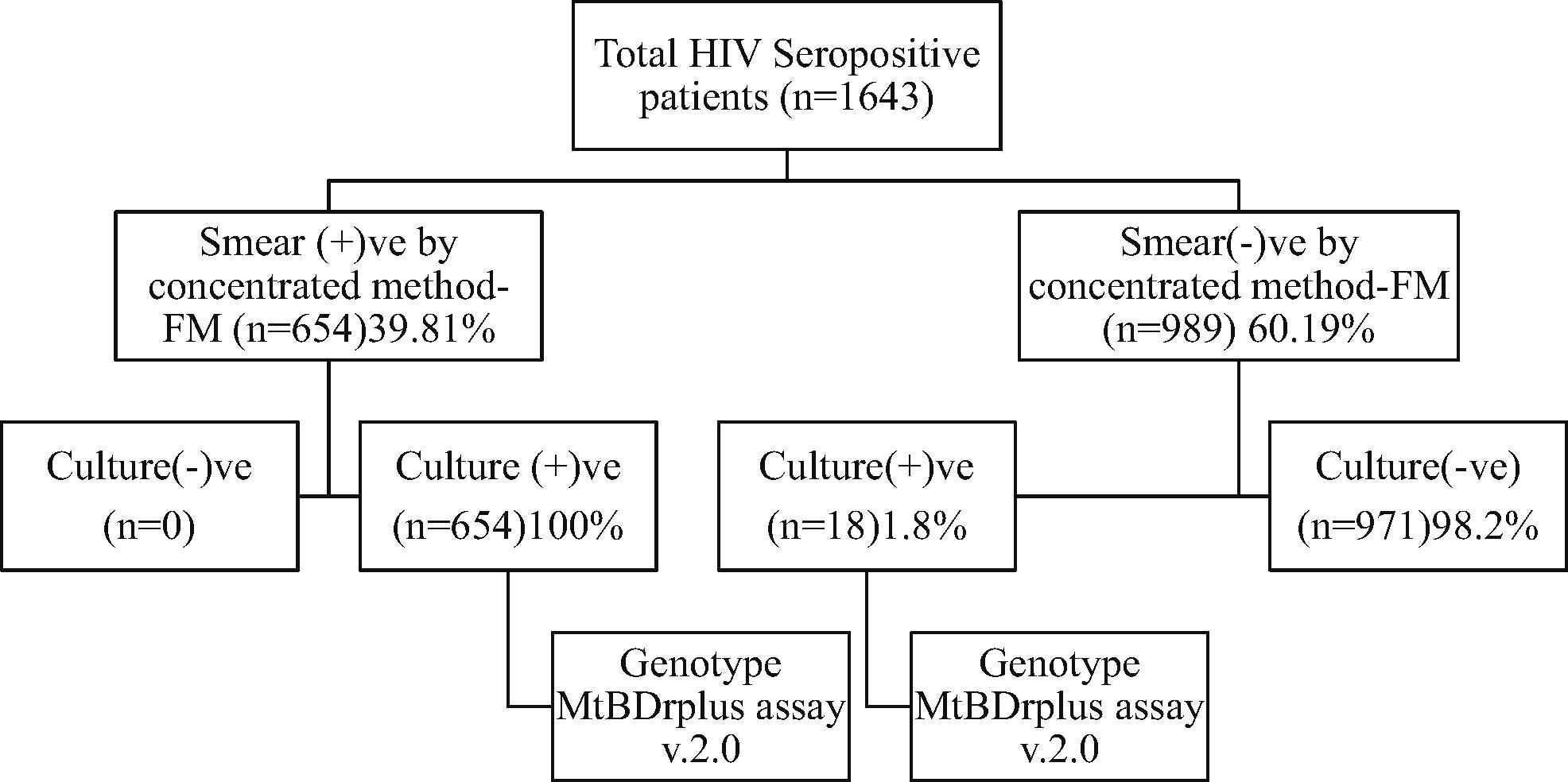
Schematic workflow for the study patients. Note. @@FM=; HIV = human immunodeficiency virus.
The patients in all age groups of culture positives were enrolled for Genotype MTBDR assay version 2.0 and most of the rifampicin-resistant TB patients 72.22% (26/36) were aged 15–45 years. The resistant pattern of 81-bp regions of rpoB gene by Genotype MTBDRplus assay was illutrated in Fig. 2. The total resistance to rifampicin was 5.55% (n = 36) and Table 2 shows the resistance profile of M. tuberculosis isolates. Of the 648 M. tuberculosis isolates, 74.54% (483) and 25.46% (175) were from male and female patients, respectively. The rate of rifampicin-resistant TB in HIV-seropositive and culture-positive men was 88.89% (32/36), compared with 11.11% (4/36) in women (Table 3). Most mutations (almost 94.44%) occurred in codons 516 (5/36, 13.88%), 526 (4/36, 5.56%), and 531 (26/36, 72.22%) of an 81-bp region of rpoB gene that encodes β-subunit of RNA polymerase, and 2.77% (1/36) mutations occurred in the 511 codon region (Table 4).
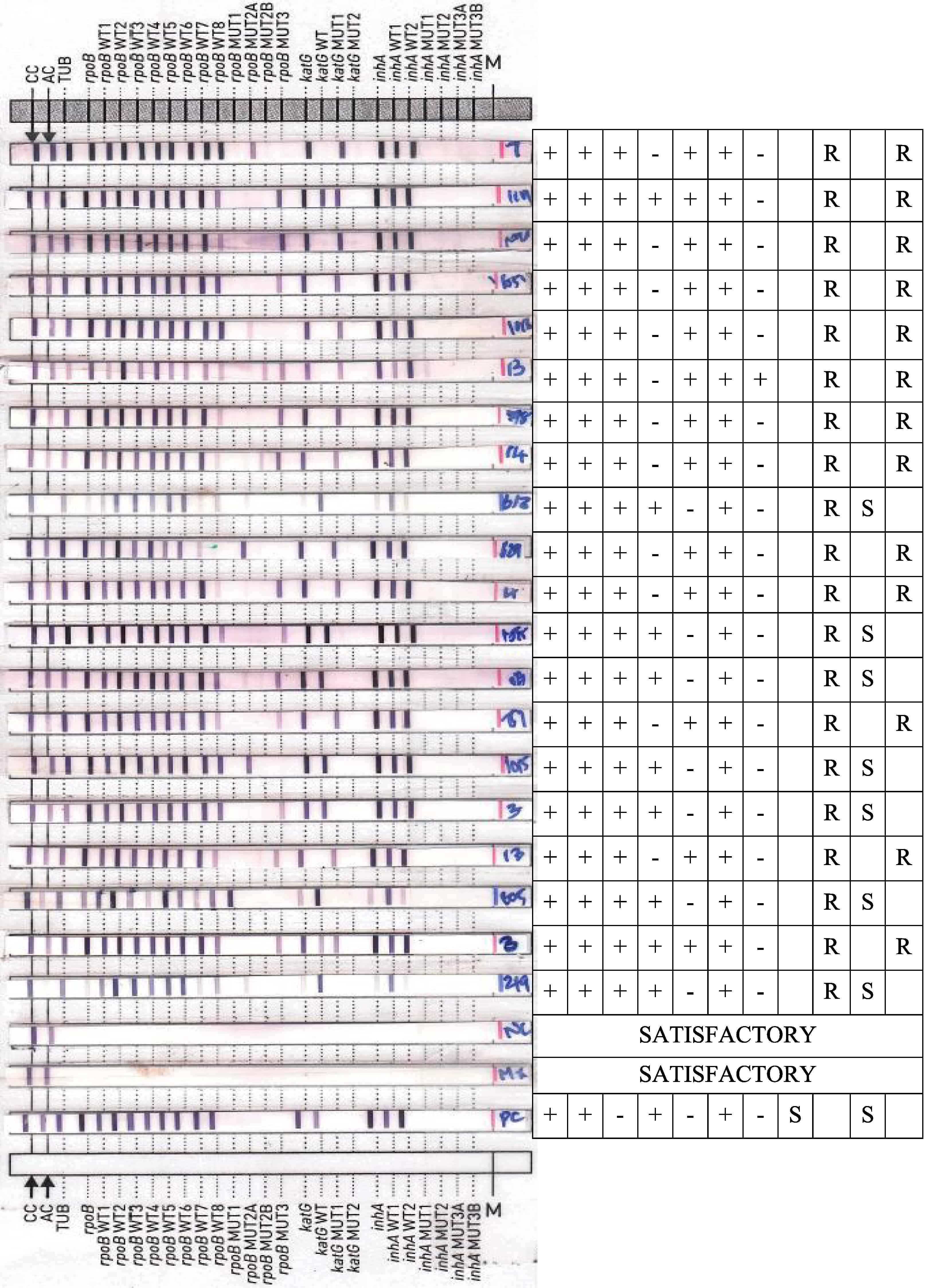
Band pattern of 81-bp regions in Genotype MTBDRplus assay version 2.0.
| Age group (y) | Total HIV seropositive | Total culture positive | Resistance pattern | |
|---|---|---|---|---|
| RI | R | |||
| ≥15 | 59 (3.59) | 10 (16.95) | 2 (20.0) | 1 (10.0) |
| CI (2.7–4.6) | CI (8.4–29.0) | CI (2.5–55.6) | CI (0.03–44.5) | |
| 16–45 | 1158 (70.48%) | 481 (41.54%) | 15 (3.12%) | 11 (2.29%) |
| CI (68.2–72.7) | CI (38.7–44.4) | CI (1.8–5.1) | CI (1.1–4.1) | |
| 46–60 | 378 (23.01) | 141 (37.30) | 3 (2.13) | 3 (2.13) |
| CI (21.0–25.1) | CI (32.4–42.4) | CI (0.4–6.0) | CI (0.4–6.0) | |
| >60 | 48 (2.92) | 16 (33.33) | 1 (6.25) | 0 |
| CI (2.2–3.9) | CI (20.4–48.4) | CI (0.2–30.2) | ||
| 1643 (100.00%) | 648 (39.44) | 21 (3.24) | 15 (2.31) | |
Note. Data are presented as n (%) or range. CI = 95% confidence interval; HIV = human immunodeficiency virus; R = rifampicin; RI = rifampicin and isoniazid.
Prevalence of rifampicin-resistant tuberculosis among 1643 HIV-seropositive patients.
| Age group (y) | Total HIV seropositive | Total culture positive | Resistance pattern | |||||
|---|---|---|---|---|---|---|---|---|
| RI | R | |||||||
| Male | Female | Male | Female | Male | Female | Male | Female | |
| ≥15 | 36 | 23 | 10 | 0 | 2 | 0 | 1 | 0 |
| >15 to ≤45 | 748 | 410 | 355 | 126 | 12 | 3 | 10 | 1 |
| >45 to ≤60 | 277 | 101 | 104 | 37 | 3 | 0 | 3 | 0 |
| >60 | 38 | 10 | 14 | 2 | 1 | 0 | 0 | 0 |
| Total | 1099 | 544 | 483 | 165 | 18 | 3 | 14 | 1 |
Note. HIV = human immunodeficiency virus; R = rifampicin; RI = rifampicin and isoniazid.
Multidrug-resistant tuberculosis stratified by sex of 1643 HIV-seropositive patients.
| Codon region | Resistance pattern | Treatment outcome, n (%) | ||||
|---|---|---|---|---|---|---|
| NR | Death | Defaulter | Cured | On Rx | ||
| 510–513 | L511P | – | – | 1 (2.77) | – | – |
| CI (0.1–14.5) | ||||||
| 513–519 | D516Y | 3 (8.33) | – | – | 1 (2.77) – | |
| CI (1.8–22.5) | CI (0.1–14.5) | |||||
| 513–519 | D516V | – | 1 (2.77) | – | – | – |
| CI (0.1–14.5) | ||||||
| 526–529 | H526Y | 2 (5.55) | – | – | – | – |
| CI (0.7–18.7) | ||||||
| 526–529 | H526R | – | – | – | – | 1 (2.77) |
| CI (0.1–14.5) | ||||||
| 526–529 | H526D | 1 (2.77) | – | – | – | |
| CI (0.1–14.5) | ||||||
| 530–533 | S531P | 3 (8.33) | 4 (11.11) | – | 5 (13.88) | 3 (8.33) |
| CI (1.8–22.5) | CI (3.1–26.1) | – | CI (4.7–29.5) | CI (1.8–22.5) | ||
| 530–533 | S531L | 1 (2.77) | 8 (22.22) | 1 (2.77) | – | 1 (2.77) |
| CI (0.1–14.5) | CI (10.1–39.2) | CI (0.1–14.5) | CI (0.1–14.5) | |||
| N (36) | 10 (27.7) | 13 (36.1) | 2 (5.55) | 6 (16.6) | 5 (13.88) | |
Note. Data are presented as n (%) or range. CI = 95% confidence interval; HIV = human immunodeficiency virus; NR = not registered; Rx = treatment.
Treatment outcome against mutations at codons of 81-bp region in ropb gene in HIV-seropositive patients.
Twenty rifampicin-resistant TB patients coinfected with HIV were registered for CAT IV treatment among the 36 diagnosed cases. Nine patients were not registered because they could not be traced; one patient was not willing to take any medication; and six patients died before starting TB treatment. The cure rate and death rate among the 20 registered cases were 30% (6/20) and 35% (7/20), respectively. Five cases were on treatment and two cases were defaulters among the 20 registered cases.
4. Discussion
The present study demonstrated high prevalence of TB among HIV/AIDS patients attending care and treatment in this setting. A study done in Dares Salaam found a TB prevalence of 15% in patients attending an HIV care and treatment clinic [24]. Another study done in rural Northern Tanzania found a prevalence of 8.5% among people living with HIV/AIDS attending care and treatment [11]. The prevalence in the present study of 39.44% among HIV-seropositive patients is high when compared with the studies in Dares Salaam and Northern Tanzania. The difference between these two previous studies can be explained by the fact that Dares Salaam is urban and contributes about 24% of all TB cases in Tanzania, while the rural area in Northern Tanzania contributes <2% of cases. Patients with low immunity due to HIV are more likely to acquire TB in an area with high TB prevalence [10]. The World Health Organization currently recommends that all HIV-infected persons need to be screened for TB, and HIV-infected persons without active TB disease should be evaluated for treatment of latent TB infection [22,23].
Coinfection with TB has been a major concern in HIV/AIDS patients. TB remains an important public health problem and has been worsened by the HIV epidemic, resulting in increased morbidity and mortality worldwide. HIV/AIDS leads to immunosuppression and is the strongest of all known risk factors for the development of TB. Thus, in the present study, the prevalence of pulmonary TB was 39.44%, which was higher than 23% reported by Dhungana et al. [25]. Sudha and Atul. [26] reported the prevalence to be 23.48%. The prevalence of coinfection with HIV varies widely across regions, as shown in different studies mentioned above, within and outside India, mainly due to the variation in the distribution of risk factors, geographic location, awareness levels, and other factors. Among the Indian studies, a prevalence similar to that in our study of 42% and 39.5% was reported by Maniar et al. [27] and Chakraborty et al. [28], respectively, whereas Mahajan et al. [29] reported a lower prevalence as 7.39%. The lower prevalence of pulmonary TB can be ascribed to the early diagnosis, increasing awareness, and high index of suspicion about the presence of TB and timely prophylaxis.
The emergence of MDR-TB in developing countries preceded the HIV epidemic and was considered to have been acquired. MDR-TB levels are higher in areas with poor TB control and the proportion of retreatment cases is high. MDR-TB detection rate among the 1643 HIV seropositive cases in this study was 5.55% (95% confidence interval 0.7–18.7). A high prevalence of MDR-TB strains was reported in tertiary health facilities as early as 1991, followed by further documentation in 2006 [30,31], including information on the magnitude of the epidemic in children [32]. A study by D’souza et al. [30] in 2009 documented high levels of multiple drug resistance (both MDR and poly-drug resistance) among previously untreated cases in urban parts of Mumbai. Hom et al. [33] reported a high prevalence of rifampicin resistance and MDR-TB, with a prevalence of 10.3% in patients previously treated for TB. MDR-TB has been associated with poor short-term outcomes among HIV-infected people in South Africa [34]. Hom et al. [33] have reported a substantial proportion of patients (52.42%) with no prior history of TB with evidence of drug resistance.
The GenoType MTBDRplus assay version 2.0 correctly identified mutations with a high concordance rate. Genotypic analysis of the 81-bp region of rpoB for rifampicin resistance is thought to be sufficient for evaluating the public health threat of MDR-TB. We observed 36 (5.55%) cases of MDR-TB in HIV-seropositive patients. Culture-positive patients of all age groups were enrolled in our study, and most of the MDR-TB patients (26/36; 72.22%) were aged 15–45 years. Among the 36 MDR-TB cases, three (8.3%) were pediatric (8.3%) and four (11.11%) were female. The total mono-resistance to rifampicin was found to be 2.31% (15/648) and 7.56% (49/648), respectively. The mutations at the 81-bp region of the rpoB gene were distinct, implying that they were acquired through separate mutagenesis events, whereas most of the strains had the same mutation (S531L) belonging to a potentially more transmissible strain. The high death rate (13, 36.1%, 95% confidence interval 20.8–53.8) was observed in patients who had a mutation at the 530–533 codon region of rpoB gene, which has not been reported in any other study.
In summary, our study demonstrated high rates of rifampicin-resistant TB in HIV-seropositive patients. Although our sample size was small, this is believed to be the first multisite study of drug-resistant TB in HIV-seropositive individuals in Puducherry, Southern India. The present study highlighted that there is a need to monitor the trend of antibiotic-resistant TB in various mutant populations in order to timely implement appropriate interventions to curb the threat of MDR-TB.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
Cite this article
TY - JOUR AU - C.K. Vidyaraj AU - A. Chitra AU - S. Smita AU - M. Muthuraj AU - S. Govindarajan AU - B. Usharani AU - S. Anbazhagi PY - 2017 DA - 2017/09/21 TI - Prevalence of rifampicin-resistant Mycobacterium tuberculosis among human-immunodeficiency-virus-seropositive patients and their treatment outcomes JO - Journal of Epidemiology and Global Health SP - 289 EP - 294 VL - 7 IS - 4 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2017.09.002 DO - 10.1016/j.jegh.2017.09.002 ID - Vidyaraj2017 ER -