
Establishing a field epidemiology elective for medical students in Kenya: A strategy for increasing public health awareness and workforce capacity
- DOI
- 10.1016/j.jegh.2014.10.002How to use a DOI?
- Keywords
- Field epidemiology; Medical elective; Workforce development; Africa
- Abstract
Medical students have limited exposure to field epidemiology, even though will assume public health roles after graduation. We established a 10-week elective in field epidemiology during medical school. Students attended one-week didactic sessions on epidemiology, and nine weeks in field placement sites. We administered pre- and post-tests to evaluate the training. We enrolled 34 students in 2011 and 2012. In 2011, we enrolled five of 24 applicants from a class of 280 medical students. In 2012, we enrolled 18 of 81 applicants from a class of 360 students; plus 11 who participated in the didactic sessions only. Among the 34 students who completed the didactic sessions, 74% were male, and their median age was 24 years (range: 22–26). The median pre-test score was 64% (range: 47–88%) and the median post-test score was 82% (range: 72–100%). Successful completion of the field projects was 100%. Six (30%) students were not aware of public health as a career option before this elective, 56% rated the field experience as outstanding, and 100% reported it increased their understanding of epidemiology. Implementing an elective in field epidemiology within the medical training is a highly acceptable strategy to increase awareness for public health among medical students.
- Copyright
- © 2014 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Developing countries face a growing spectrum of public health challenges arising from emerging infectious diseases, HIV/AIDS and sexually transmitted diseases, unintentional injuries, neglected diseases, and non-communicable diseases [1–3]. Addressing these complex and diverse health events require a workforce skilled in epidemiology, surveillance and response. Many countries have implemented field epidemiology training programs to train public health professionals in epidemiology [4–8]. Nonetheless, there are continued challenges to assure adequate epidemiologic capacity at all levels of the public health system. In Central America, a pyramidal training model was established to provide training at the basic, intermediate, and advanced levels for various professionals within the public health system [9]. Despite the value of this model, replication of this concept may not be possible in countries with a limited substrate of public health professionals with higher education.
Despite a longstanding recognition for the importance of the inclusion of public health and field epidemiology within the overall training of medical students, limited progress has been achieved in this area [10,11]. This deficit results from the ongoing competition for time within the medical school curriculum as an increasing number of disciplines contend with each other to justify their time within the medical curriculum. A survey among medical students in sub-Saharan Africa to identify interventions to improve retention in their country of origin found that 2.6% intended to pursue a career in public health. This suggests that career intentions of medical students graduating from universities in Africa are not aligned with the workforce needs of the continent [12]. Moreover, several studies have shown that formal exposure to public health during medical school results in health professionals choosing careers in public health, or devoting more time to non-clinical activities [13–15]. Medical school students are a critical target in developing a robust national strategy to increase epidemiology and public health workforce development in Africa.
The Kenya Field Epidemiology and Laboratory Training Program (FELTP) was established in 2004 and is a division within the Directorate for Preventive and Promotive Health Services of the Ministry of Health. The core mandate of the Kenya FELTP is to increase epidemiologic capacity within the Ministry of Health. The Kenya FELTP focuses on a two-year Masters degree awarding training. In this two-year training applied epidemiological principles are learned mostly through assessing incoming surveillance and similar data, applying epidemiology to respond to disease outbreaks, developing and assessing outcomes of interventions, and implementing prevention programs [16]. This training-through-service approach ensures that the activities of the trainees help strengthen the public health systems. The program enrolls approximately 20 Ministry officers each year. Additional efforts led by the Kenya FELTP to increase epidemiologic capacity within the Ministry of Health include short-course trainings on basic field epidemiology, surveillance and outbreak investigations. This short-course training is offered to district and county surveillance and medical officers. The training consists of one-week didactic module after which participants are mentored for approximately four to six months as they work on field projects relevant to their districts. During the last week of the training, participants present their work to their peers and other relevant senior officials within the Ministry of Health. Recently, through the support from the U.S. President’s Emergency Plan for AIDS Relief Plan and the Medical Education Partnership Initiative, Kenya FELTP began to integrate medical school students into the national strategy for developing a public health epidemiologic workforce [17,18].
In Kenya, pre-service medical training is conducted in four universities, with the largest number of medical doctors graduating from the University of Nairobi. In these universities, the medical curriculum offers very limited exposure to field epidemiology and surveillance. Upon graduation from medical school, many graduates work as district medical officers. In this capacity they may expect to conduct surveillance and field epidemiology functions. This manuscript describes the implementation of basic training in field epidemiology and surveillance during the elective term for fourth year medical students at the University of Nairobi. The main objective of this elective was to develop competency among medical students in core aspects of surveillance and the use of epidemiologic data. A secondary objective was to expose medical students to epidemiology and public health as a career option.
2. Methods
2.1. Elective structure
The current medical curriculum at the University of Nairobi includes a 12-week elective block during the fourth year, usually from October to December. The students must arrange a placement site that serves their learning objectives. Within this elective block, the elective in Field Epidemiology and Public Health Surveillance was implemented. During this elective, students fulfill their competencies through course work, a practicum field placement, and written and oral presentations. During the first week students attended didactic sessions covering topics of basic field epidemiology and surveillance. The following 10 weeks, students were placed in one of various field sites at the national and sub-national level. During these field placements students were paired with a Kenya FELTP resident or graduate, who supervised their activities. While at their field site, students performed a project that included drafting a short protocol, collecting and analyzing data, and describing a surveillance system. Additionally, students participated with their supervisor in other public health activities being conducted at the placement site, such as immunization campaigns, community education, and district health management meetings. During the last week of the elective, students returned to Nairobi, where they drafted a report and gave a formal presentation describing the rationale, methods, findings, and recommendations derived from their data analysis.
2.2. Didactic curriculum
The didactic curriculum included lectures, case studies, and small group exercises. The curriculum was spread over five days, with six hours of training each day. The topics covered during these didactic sessions included epidemiology, surveillance, response, and basic data analysis (Fig. 1). The instructors for these sessions included staff from Kenya FELTP and from the US Centers for Disease Control and Prevention (CDC). Second year Kenya FELTP residents and graduates also provided support during the case studies and group exercises.
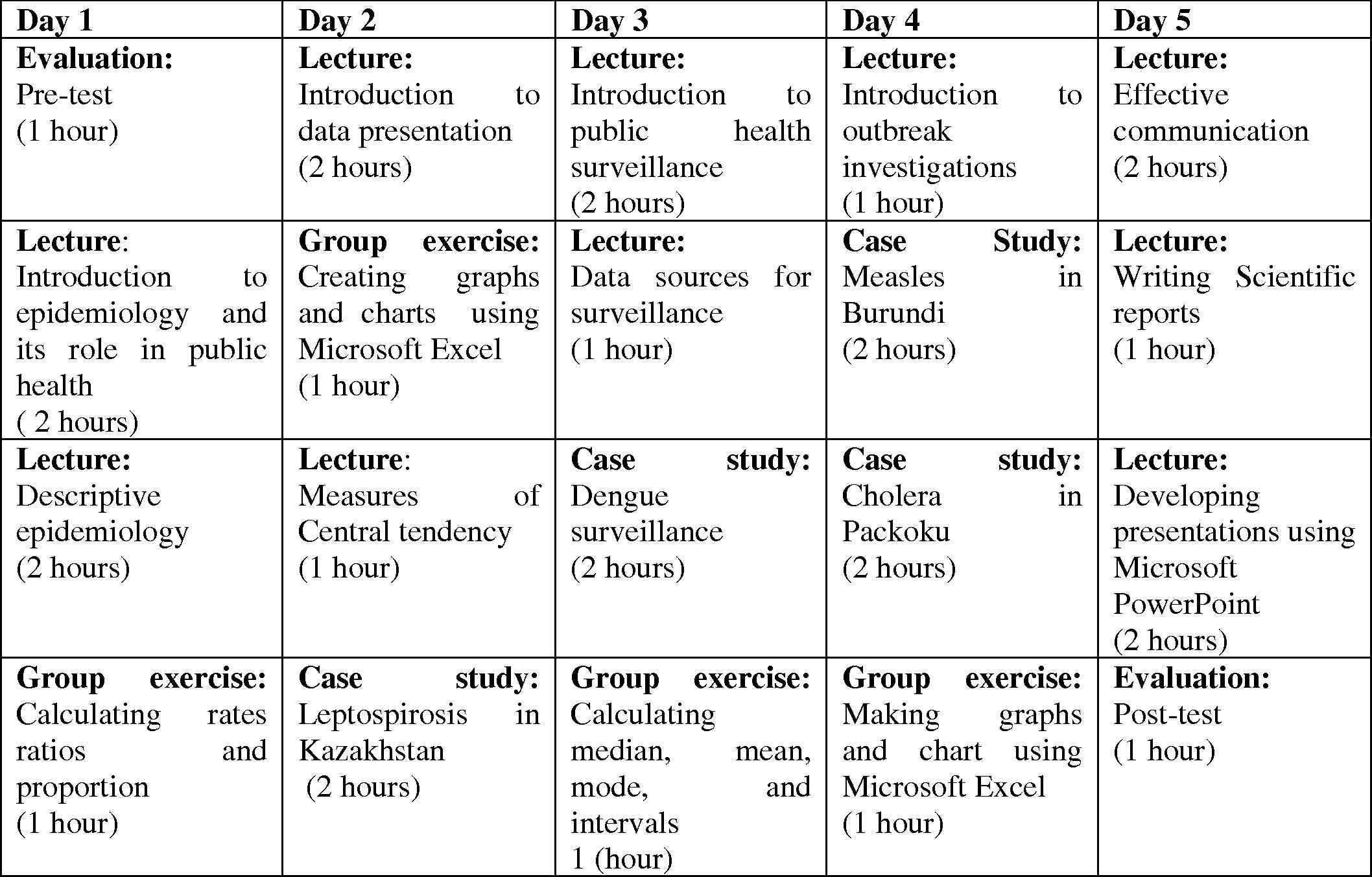
Sample course schedule for the one week didactic session during the Field Epidemiology and Public Health Elective for medical students in Kenya.
2.3. Evaluation
A one-hour pre- and post-test evaluation with 25 paper-based multiple choice questions covering all topics was conducted. The pre-test was given immediately before the beginning of the first didactic session, while the post-test was administered after the last didactic session. After the field placement, a satisfaction survey was conducted with all students who participated in the field placement component of the elective using an anonymous paper-based questionnaire. The questionnaire contained information regarding satisfaction on the didactic and practicum components, post-graduate career and training choices. The satisfaction questions were multiple choice-type using a five-level Likert format with choices ranging from “strongly agree” to “strongly dis-agree”. Students were given a “pass” or “fail” after completion of the elective. To “pass” the elective, students had to achieve a post-test score of ⩾70%, satisfactorily present their data analysis report, and receive a satisfactory appraisal from their field supervisors.
3. Results
To date this elective in Field Epidemiology and Public Health Surveillance has been offered twice–once in 2011 and again in 2012. The 2011 elective was implemented as a pilot. After advertising the elective throughout the medical school, 25 (9%) out of a class of 280 students applied. Five (21%) of the 24 applicants were enrolled. For the 2012 elective 83 (23%) out of a class of 360 students applied and 29 (36%) of the applicants were enrolled. Given human and financial resource limitations, 18 students enrolled in the 2012 didactic course and participated in the supervised field placement experience. All students who participated in the one-week didactic course received a certificate of course participation, but only students who also participated in the field elective received credit toward graduation.
Among the 34 students who completed the one-week didactic portion of the elective during both years, all were fourth year medical students, 71% of the 34 students were male, and their median age was 24 years (range: 22–26 years). The median pre-test score was 64% (range: 47–88%). The median post-test score was 82% (range: 72–100%) and the average score was 83%. The average percent improvement for the participants from the pre-test to the post-test was 24%. Of the 23 students who completed the field placement portion of the elective, 65% were male, and their median age was 24 years (range: 22–26 years). Four (17%) students were placed at a national level field placement site, and the rest at a sub-national placement site. During the field elective, students conducted surveillance evaluations and data analysis on the topics of vaccine preventable diseases, malaria, infectious diseases (diarrhea, typhoid, and flu), child health, and non-communicable diseases. Students were involved in a variety of other activities, such as vaccination campaigns, educational campaigns for diabetes, hand washing, helmet usage, and outbreak investigations. All students satisfactorily completed the field elective.
In the exit survey, 30% of the 18 students reported not being aware of public health as a career option before the elective, 56% rated the field experience as outstanding, and 100% reported that the elective increased their understanding of epidemiology. Five (31%) students reported having received inadequate supervision in their field sites, and 50% of students recommended that supervision in the field sites should be improved for future electives. All students indicated that they would consider public health as a career in the future. All students also recommended inclusion of the contents of the elective in the medical school curriculum, and that an increased number of students be enrolled in following years.
4. Discussion
It was found that implementing an elective in field epidemiology and public health surveillance within a medical school elective rotation is a highly acceptable and effective strategy to increase awareness and interest of medical students in considering public health and epidemiology in their professional careers. Field placements not only reinforced theoretical training, but the outputs of the field experience provided a valuable service to the Ministry of Health, particularly at the sub-national level where staff with this level of skills is limited. The elective addresses a critical gap, as after completion of the elective and graduating from medical school, these professionals are better trained to serve as district medical officers. The elective may also stimulate students to pursue more non-clinical duties and even inspire them to consider careers in public health. Though the extent to which medical students view a career choice can be modified by their medical school training needs further investigation, most researchers agree that exposure to a discipline during medical training may influence continued practice of these disciplines after graduation [19].
It was also found during the exit survey that a third of the students reported inadequate field supervision during the elective. Supervision during field placements is a critical challenge to any field and competency-based training program. Selection of field sites for the elective must consider the availability of adequate supervisors. In future cohorts, students will only be placed in field sites that include a current second year FELTP resident who can serve as a field supervisor for the medical students. A short training for the field supervisors will be provided to assure their awareness of the elective competencies and to adequately support the students.
Medical graduates who have taken the elective and are deployed to serve as district medical officers will be better skilled to improve surveillance, conduct outbreak investigations, monitor immunization campaigns, target vector control strategies, and use data to make evidence-based decisions. These graduates will become prime candidates for joining the Kenya FELTP advanced two-year degree-awarding program. Therefore, medical students can be targeted as the base for a pyramidal approach to training, where medical graduates who have taken the elective in field epidemiology and public health surveillance can be further skilled in more advanced epidemiological methods in their roles as district medical officers and subsequently as FELTP residents. Since Kenya FELTP residents are required to teach medical students during the elective in field epidemiology and public surveillance, this approach promotes a sustainable model for developing an epidemiologic workforce capacity in Kenya (Fig. 2 ).
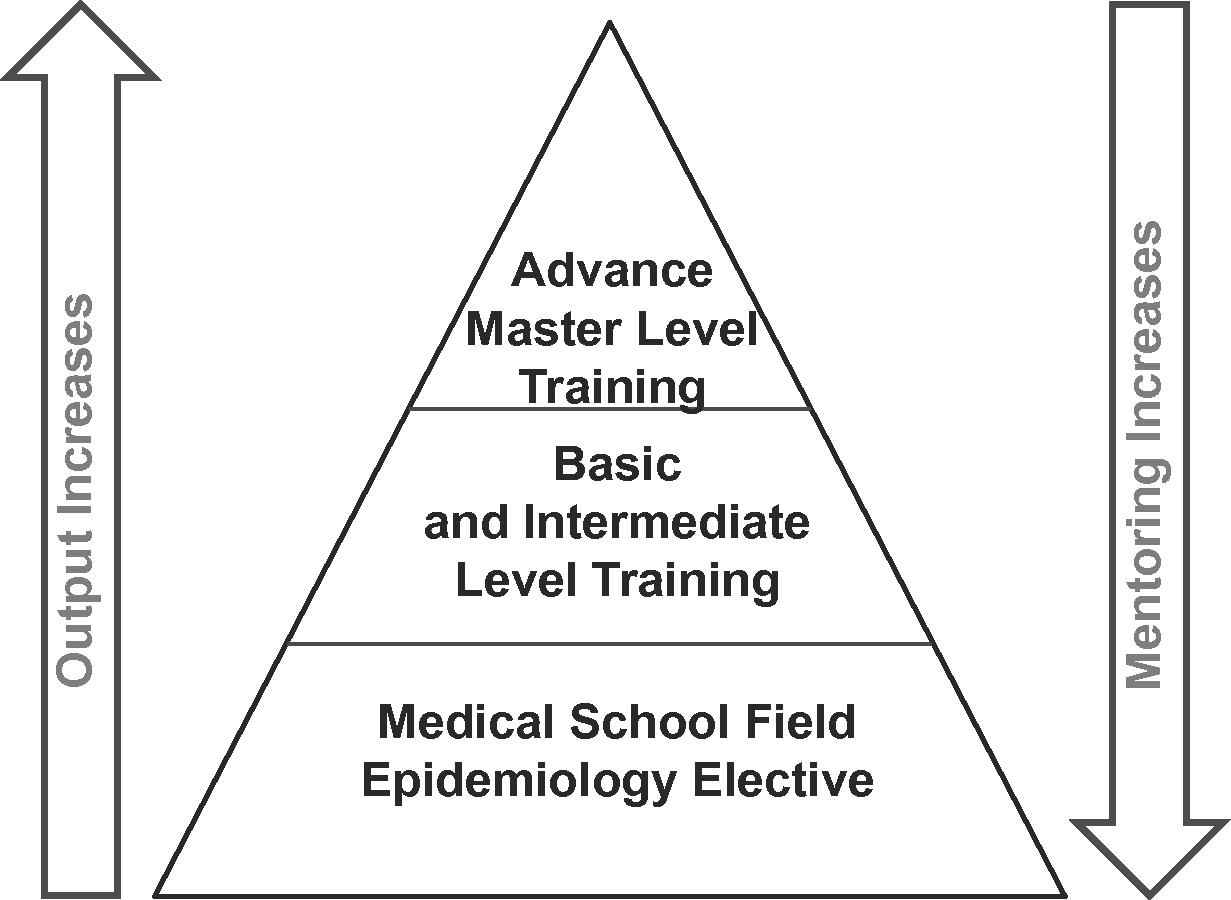
Diagrammatic representation of the pyramidal training structure for developing a sustainable epidemiologic and public health workforce in Kenya.
These findings are subject to several limitations. First, the medical student elective was introduced during a block of unstructured elective time, when students have limited elective choices and many seek mentors individually to develop their own electives. This situation may have reflected a higher interest in the elective than if multiple structured opportunities were available to students during this block. Second, the post-test was conducted immediately after the completion of the didactic week, and it remained unclear if there would be long-term retention of the material taught during the elective. In future electives an additional post-test following the field placement was suggested to evaluate learning in the longer term and to assess the impact of the field placement in individual learning. Finally, results from the survey conducted on career paths at the end of the elective could reflect some interviewer bias leading to an overestimation of the potential impact of the elective on future career paths. Though attempts were made to maintain anonymity of this survey, it is unclear of the extent of this bias.
5. Conclusions
Establishment of an elective in field epidemiology and public health surveillance for medical students was found to be highly acceptable. The elective also serves as a strategy to increase awareness in practical aspects of public health and field epidemiology, and provided a platform for creating interest in careers in public health among medical students in Kenya. Training in epidemiology and surveillance during the pre-service stage allows for the development of a pyramidal training approach where more advanced skills can be provided during the in-service stages as district medical officers and FELTP residents. Based on this experience, it is recommended that any country interested in developing similar platforms should first establish a partnership between the Ministry of Health and a school of public health from the university training the targeted medical students. A direct partnership between the Ministry of Health and an academic institution was crucial for this elective to be successful. An ideal collaboration should consider the Ministry of Health staff as adjunct professors for the university, such as Ministry staff can directly supervise and grade the medical students. For a broader implementation of this platform the didactic sessions of the elective could be offered to a wide number of students. The number of students who participate in the field experience will be limited by the availability of adequate placement sites with available data and experienced and willing supervisors. Cost is an additional consideration in the implementation of the field epidemiology elective; different from other medical student electives, placement of students in the field epidemiology elective required additional financial support. Supervisors are usually Ministry of Health personnel outside the medical school system and may require some remuneration. Since field placements were usually far from the students’ home, a small stipend was also provided to partially support living arrangements during the elective. In some circumstances, additional funds were made available to support specific field work activities when these were of high priority to the Ministry of Health and available support for the student from the field placement was limited.
This elective is expected to continue to be offered at the University of Nairobi, and in coming years include more students. This elective in field epidemiology and surveillance will also be expanded to include other medical schools and veterinary schools in Kenya. Though including field epidemiology concepts and experiences within existing elective structures is a reasonable and simple approach, additional considerations should be given to include the contents of the elective experience within the medical school curriculum. Integration of field epidemiology within the medical school curriculum will result in broader and systematic exposure of public health surveillance and epidemiology principles among medical students.
Conflict of interest statement
All the authors declare no financial or personal relationships with other people or organizations that could inappropriately influence this work.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the U.S. Centers for Disease Control and Prevention (CDC).
Ethics consideration
The manuscript describes data that did not involve human subjects. The study was approved by the Kenyan Ministry of Health.
Author contributions
WA, JO, DJ, and RD conceptualized the field epidemiology elective for medical students; WA, ZG, SA, PW, and DO implemented and supervised the elective; WA, ZG, SA, PW, JO, SB, DJ, DO, and RD participated in drafting and revising the manuscript and providing important intellectual content. The study was overseen by WA. All authors have provided approval of the final manuscript.
Role of the funding source
The Field Epidemiology and Public Health Elective was funded in part by the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) in support of the Medical Education Partnership Initiative (MEPI) to develop, expand and enhance models of medical education in Sub-Saharan African countries. The funders had no role in the study design; in the collection, analysis and interpretation of data; in the writing of the manuscript; and in the decision to submit the article for publication.
Acknowledgments
We would like to thank all the medical students who have participated in the Field Epidemiology and Public Health Elective, and wish them the very best as they continue through their medical education and career. We are also grateful for the logistical and administrative support of the Kenya FELTP Program Support Unit, in particular Alex Jones, Marion Mwangi, and Gabriel Oluoch. Additionally, we are thankful for the administrative support of the African Field Epidemiology Network (AFENET).
References
Cite this article
TY - JOUR AU - Wences Arvelo AU - Zeinab Gura AU - Samuel Amwayi AU - Petra Wiersma AU - Jared Omolo AU - Steven Becknell AU - Donna Jones AU - Dismas Ongore AU - Richard Dicker PY - 2014 DA - 2014/11/16 TI - Establishing a field epidemiology elective for medical students in Kenya: A strategy for increasing public health awareness and workforce capacity JO - Journal of Epidemiology and Global Health SP - 33 EP - 39 VL - 5 IS - 1 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2014.10.002 DO - 10.1016/j.jegh.2014.10.002 ID - Arvelo2014 ER -