
Investigation of the Risk Awareness of Wearing Masks by the Public during COVID-19 According to the Health Belief Questionnaires of Shanxi Province Residents
- DOI
- 10.2991/jracr.k.210111.001How to use a DOI?
- Keywords
- Risk; COVID-19; mask wearing behavior; health belief model; diffusion of innovation theory; structural equation model; influencing factors
- Abstract
When some parts of the world are still debating whether the public wearing masks will help prevent and control the COVID-19. We have used questionnaires to investigate the wearing of masks and its influencing factors among residents in 11 cities in Shanxi Province. The questionnaire was designed based on the health belief model. We processed the collected data using the structural equation method. The results we got are as follows: (1) the average score of perceived severity is 3.14, indicating that the respondents had a strong sense of risk; (2) The average score of perceived benefits was 4.00, indicating that respondents thought that wearing masks can prevent COVID-19; (3) The average score of perceived barriers was 2.42, indicating that the respondents believed that there were fewer barriers against wearing masks during the epidemic; (4) The average score of perceived susceptibility was 3.23, indicating that respondents believed that they had a strong risk awareness of COVID-19 infection; (5) The average score of self-efficacy was 4.00, indicating that respondents had a strong belief in wearing masks correctly. The structural equation model shows that self-efficacy (λ = 0.40) and perceived susceptibility (λ = −0.15) had direct effects on the behavior of wearing masks. A wide range of mediating effects exists in the model. Perceived severity has an effect on the behavior of wearing masks through perceived susceptibility (λ = 0.41), perceived benefits through self-efficacy (λ = 0.68) and perceived susceptibility (λ = −0.35), and perceived barriers through self-efficacy (λ = −0.28). People are in the early adopter phase. Each dimension has a direct or indirect impact on the wearing of masks during the COVID-19 epidemic.
- Copyright
- © 2021 The Authors. Published by Atlantis Press B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. LITERATURE REVIEW
Novel Coronavirus (COVID-19), which appeared in 2019 and spread around the world, is a newly discovered coronavirus strain. The pneumonia caused by it was confirmed to be an acute respiratory infectious disease [1]. As a newly discovered acute respiratory infectious disease. It poses a great threat to public health. COVID-19 prevention is necessary due to its high speed of transmission and the lack of therapeutic means. According to “COVID-19 Diagnosis and Treatment Plan (trial version 7)” [2], respiratory droplets and close contact are the main transmission routes of COVID-19, and aerosol transmission may exist when exposed to high concentration of COVID-19 contained aerosol in a relatively closed environment for a long time. In today’s epidemic, wearing masks can effectively prevent the spread of the virus. Based on the current situation, on May 26, 2020, Disease prevention and control bureau issued notice on the issuance of guidelines for the public to wear masks scientifically, it divides the population into the general public, people in specific places, key people, and occupationally exposed people, etc., and put forward scientific advice to wear masks under different places.
Although a great deal of research has been conducted on risk perception, there is still no consensus on the dimensions and measures of risk perception: Is risk strictly cognitive or emotional; Risk may differ before and after preventive actions (such as wearing a mask) [3]. This study believes that risk is a strict cognitive process, which is measured in two dimensions: perceived susceptibility, or the probability of the outcome, and perceived severity, or the size of the outcome. Studies on wearing masks during the epidemic also include the protection of masks against COVID-19 susceptibility and severity. In order to make the model more complete, based on the health belief model, this study supplemented the perceived benefit, perceived barriers and self-efficacy.
The behavior of wearing masks is a kind of health behavior, which is generally studied through health belief model. The model has been relatively mature. Health belief model can change people’s behavior by interfering with people’s attitude and other psychological activities. The structural equation model can deal with the relationship between multiple causes and multiple results at the same time. In this study, it can effectively deal with the relationship between multiple independent variables on the public behavior of wearing masks, and analyze the correlation and quantitative relationship between potential variables. In the context of COVID-19, structural equation model plays an important role in studying the behavior of the public wearing masks. Based on the structural equation model and the health belief model, the results and the conclusion can improve the public’s cognition of wearing masks, so as to promote the change of public behavior. Due to the lack of relevant studies on the behavior of wearing masks during COVID-19, this study is based on these two models to conduct investigation on the behavior of the public wearing masks, hoping to promote the change of the behavior of the public wearing masks.
2. RESEARCH OBJECTS AND METHODS
2.1. Research Objects
The residents of Shanxi Province were taken as the research object. The inclusion criteria are as follows: long-term residence in Shanxi; Have a certain ability to take care of themselves; Can complete the network questionnaire or complete the questionnaire with the help of the investigator; Understand each item in the questionnaire; Volunteer to participate in this study. Exclusion criteria are as follows: questionnaires with repeated IP addresses; With inconsistent logic. Incomplete questionnaires.
2.2. Research Methods
2.2.1. Taking samples
This study adopts the questionnaire through stratified cluster random sampling, draws a certain number of Shanxi residents for investigation Shanxi Province was divided into 11 prefecture-level cities, Taiyuan city, Datong City, Yangquan City, Changzhi City, Jincheng City, Shuozhou City, Jinzhong City, Yuncheng City, Xinzhou City, Linfen City and Luliang City, and 1–2 communities were selected for random sampling in each prefecture-level city.
2.2.2. Questionnaire design
The first part of the questionnaire is the general demographic characteristics of the sample population, including gender, age, current city, whether the permanent residence is an urban or rural area, highest educational level, ethnic group, religious belief, marital status, monthly income, occupation, etc.
The second part of the questionnaire is the investigation of the behavioral influence factors based on the health belief model, and set questions on the influence factors of the behavior of wearing masks during the epidemic: a total of 21 items, include five dimensions: severity (three items), perceived benefits (five items), perceived barriers (four items), self-efficacy (five items) and perceived susceptibility (four items). Each item is scored by Likert 5-level scoring method, which were 1–5 points from low to high.
The third part of the questionnaire is based on the diffusion of innovation theory, Through this part, we divide the behavior of the public to wear masks during the epidemic into five behavioral stages: innovators (the first to adopt the behavior and to spread and persuade others), early adopters (the earlier group to adopt the behavior and to spread one’s subjective view), early public (adopt the behavior after careful consideration), late public (adopt the behavior later and easily changed by external influence), laggards (resistance or late adoption).
2.2.3. Survey methods
Due to the epidemic, the questionnaires were mainly distributed online. Questionnaires were distributed one-on-one through Wechat, QQ and other social platforms to residents of 11 prefecture-level cities in Shanxi Province. In order to ensure the validity of the questionnaire, the investigator answered the questions raised by the respondents, and a total of 1603 valid questionnaires were recovered in the end.
2.2.4. Statistical analysis
IBM SPSS21.0 software (Armonk, NY, USA) was used for statistical analysis. The mean value and standard deviation were used to study the central trend 95% of the sample statistics were taken as the confidence interval. The structural equation model was established by using IBM SPSS AMOS24.0 for latent variable analysis. Chi-square/DF, Goodness-of-Fit Index (GFI), Adjusted Goodnessof-Fit Index (AGFI), Comparative Fit Indexes (CFI) and Root Mean Square of Approximate Error (RMSEA) are used in the structural equation model, take α = 0.05 as the standard of statistical test significance.
2.2.5. Quality control
Before the questionnaires were distributed, we conducted a unified training for the investigators to ensure the standardization of the survey process and improve the reliability and validity of the questionnaire survey. All questionnaires are filled in anonymously, which can reduce the concerns of respondents. After the questionnaires were collected, we checked the logical relationship of the questionnaires, and eliminated questionnaires with inconsistent logic before and after the options and incomplete questionnaires. The survey was reviewed and approved by the Ethics Committee of Changzhi Medical College RT2020018, and all the respondents understood the project content and signed the informed consent form.
3. RESULTS
3.1. Basic Information and Descriptive Statistics
A total of 1635 questionnaires were collected, and 1603 were finally confirmed to be the valid questionnaires, with an effective rate of 98.04%. Among the valid 1603 questionnaires, the basic information of 10 respondents was randomly selected, as shown in Table 1. There are 625 innovators (39.0%), 570 early adopters (35.6%), 249 early public (15.5%), 110 late public (6.9%), and 49 laggards (3.1%) of mask wearing. The scores of innovator, early adopter, early public, late public and laggards are 5 points, 4 points, 3 points, 2 points and 1 point respectively. According to the survey, the mean of the overall score is 4.01 points (3.95, 4.06), which is in the transition stage from early adopter to innovator. Univariate factors showed that there were significant statistical differences among different age groups, cities, education level, marital status, smoking status, infection of relatives and friends, etc., in the behavior of wearing masks during the epidemic period (see Figure 1 for details).
| Serial number | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 1 | 3 | 2 | 5 | 5 | 1 | 1 | 1 | 4 | 2 | 3 | 3 | 3 |
| 2 | 2 | 4 | 1 | 1 | 5 | 4 | 2 | 2 | 3 | 5 | 2 | 2 | 3 | 3 |
| 3 | 2 | 6 | 6 | 1 | 1 | 7 | 1 | 4 | 1 | 5 | 1 | 1 | 1 | 1 |
| 4 | 1 | 5 | 11 | 1 | 4 | 2 | 1 | 2 | 4 | 6 | 1 | 2 | 2 | 1 |
| 5 | 2 | 7 | 5 | 2 | 6 | 6 | 1 | 2 | 5 | 4 | 2 | 1 | 3 | 3 |
| 6 | 1 | 5 | 9 | 1 | 6 | 3 | 2 | 2 | 3 | 3 | 2 | 2 | 3 | 1 |
| 7 | 1 | 2 | 4 | 2 | 7 | 1 | 2 | 1 | 3 | 8 | 1 | 2 | 3 | 1 |
| 8 | 1 | 3 | 8 | 2 | 5 | 1 | 2 | 2 | 4 | 6 | 1 | 2 | 3 | 3 |
| 9 | 2 | 2 | 2 | 1 | 7 | 1 | 2 | 1 | 4 | 8 | 1 | 2 | 3 | 3 |
| 10 | 1 | 1 | 7 | 1 | 4 | 1 | 2 | 1 | 3 | 7 | 1 | 2 | 3 | 3 |
Note: Q1 Your gender: 1 = male, 2 = female; Q2 Your age: 1 = under 18 years old, 2 =18–25 years old, 3 = 26–30 years old, 4 = 31–40 years old, 5 = 41–50 years old, 6 = 51–60 years old, 7 = over 60 years old; Q3 Your city: 1: Taiyuan, 2: Datong, 3: Shuozhou, 4: Xinzhou, 5: Yangquan, 6: Lvliang, 7: Jinzhong, 8: Changzhi, 9: Jincheng, 10: Linfen, 11: Yuncheng; Q4 Your usual place of residence: 1: urban, 2: rural; Q5 Your highest education: 1: No formal education, 2: Primary school, 3: Junior high school, 4: Senior High school, 5: Technical secondary school, 6: Junior College, 7: University undergraduate, 8: Master’s degree, 9: Doctoral degree; Q6 Your nationalities: 1: Han nationality, 2: Hui nationality, 3: Zhuang nationality, 4: Tibetan nationality, 5: Miao nationality, 6: Manchu nationality, 7: Others. Q7: Religious belief: 1: have, 2: have nothing; Q8 Your marital status: 1: unmarried, 2: married, 3: divorced, 4: widowed; Q9 Per capita monthly income of your family: 1: No income: less than 2.00 yuan, 3: 1000-2999 yuan, 4: 3000-4999 yuan, 5: 5000 and above; Q10 What is your current or retired career: 1: office/business unit personnel, 2: professional and technical personnel, 3: business unit personnel, 4: business, service personnel, 5: agriculture, forestry, animal husbandry and fishery, water conservation, production personnel, 6: manufacturing, transportation equipment operators and related personnel, 7: soldiers, 8: student: 9 other employed and unemployed; Q11 So far, are there any confirmed cases in your current city?: 1: There are 2: there are no 3: It is not clear; Q12 Have any of your family or friends infected with novel Coronavirus in this epidemic?: 1: There are 2: there are no 3: It is not clear; Q13 Do you smoke?: 1: Smoking 2: have quit smoking 3: Never smoking; Q14 Do you drink alcohol?: 1: drinking 2: abstaining from alcohol 3; Never drink.
Basic information of 10 randomly selected respondents
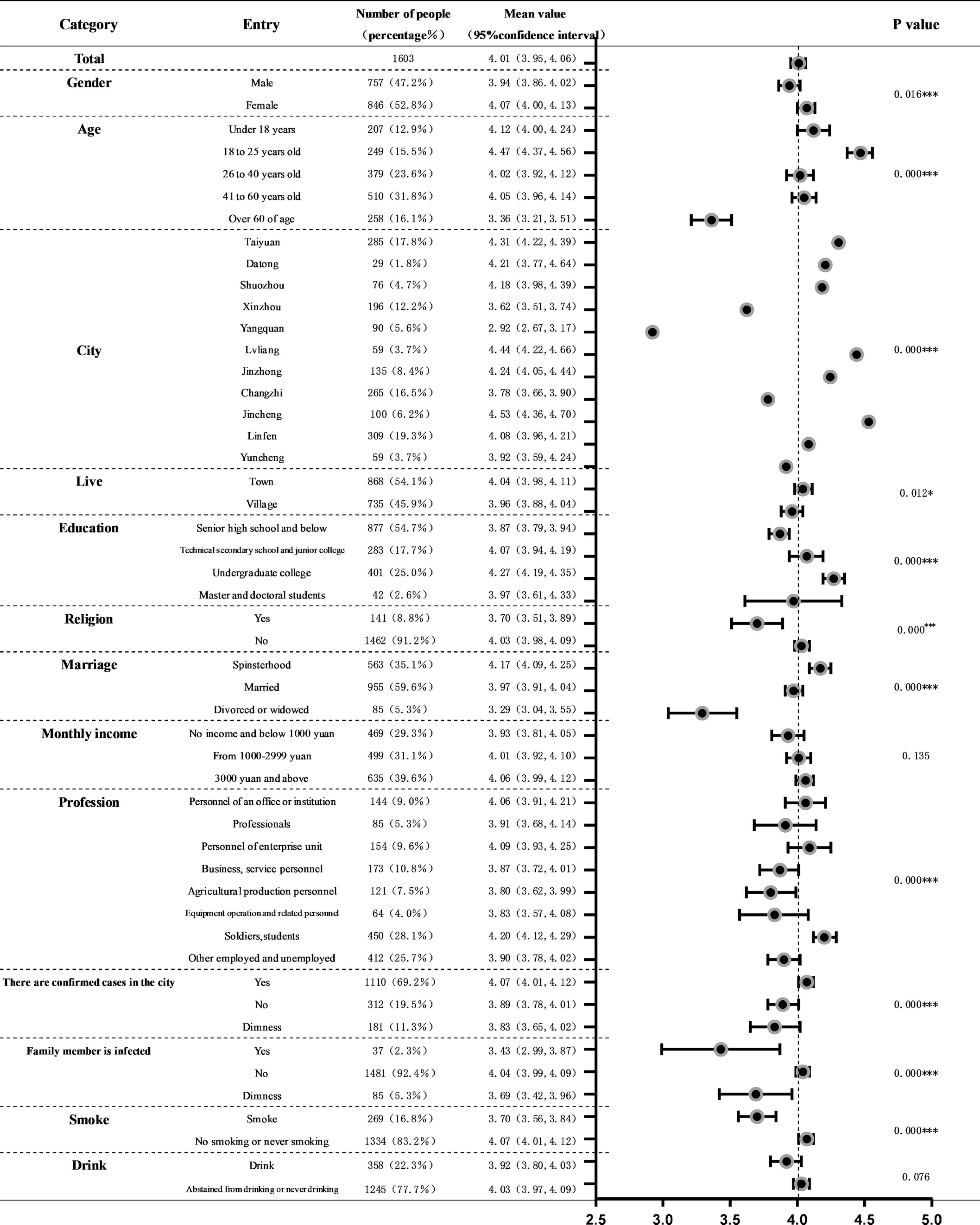
Comparison of individual characteristics with behaviors of wearing masks during the epidemic.
3.2. Health Belief Theory of the Public’s Behavior of Wearing Masks during the Epidemic
The average score of perceived severity was 3.14 (3.10, 3.18); perceived benefits 4.00 (3.96, 4.03); perceived barriers 2.42 (2.37, 2.46); self-efficacy 4.00 (3.96, 4.04); perceived susceptibility 3.23 (2.42, 4.04). The responses of the above 10 respondents to each item are shown in Table 2. Table 3 shows the correlation between the factors.
| Serial number | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| The COVID-19 epidemic will last a long time. | 5 | 5 | 4 | 4 | 4 | 3 | 3 | 3 | 3 | 2 |
| Covid-19 affects my relationship with my family or friends. | 4 | 4 | 3 | 4 | 4 | 2 | 4 | 1 | 2 | 1 |
| If I have COVID-19, I will probably lose my life. | 3 | 4 | 4 | 4 | 4 | 2 | 3 | 3 | 2 | 1 |
| Wearing masks can reduce my chance of suffering from COVID-19. | 5 | 5 | 4 | 4 | 5 | 5 | 4 | 4 | 4 | 5 |
| Wearing masks can protect my family and reduce their risk of infection. | 5 | 4 | 4 | 4 | 5 | 4 | 4 | 1 | 4 | 4 |
| Wearing masks is an expression of responsibility to my family. | 5 | 5 | 4 | 4 | 4 | 5 | 4 | 1 | 4 | 4 |
| Wearing masks can make me at ease about my health. | 4 | 4 | 3 | 4 | 4 | 4 | 4 | 4 | 4 | 4 |
| I can take advantage of wearing masks. | 3 | 4 | 3 | 4 | 4 | 5 | 4 | 4 | 3 | 4 |
| I think the cost of buying masks is high. | 3 | 4 | 4 | 3 | 3 | 1 | 2 | 2 | 3 | 2 |
| It is uncertain whether the mask wearing behavior is effective to avoid the infection. | 2 | 3 | 3 | 2 | 1 | 1 | 2 | 3 | 2 | 1 |
| I often forget to wear a mask. | 3 | 4 | 2 | 2 | 3 | 1 | 2 | 1 | 2 | 1 |
| The process of wearing a mask will make me feel uncomfortable. | 4 | 5 | 4 | 2 | 4 | 1 | 2 | 3 | 4 | 1 |
| I can pay attention and frequently check information on how to prevent COVID-19. | 4 | 5 | 2 | 4 | 5 | 5 | 4 | 1 | 4 | 4 |
| I’m sure I can wear a mask actively. | 3 | 4 | 3 | 4 | 4 | 5 | 4 | 3 | 4 | 4 |
| I am sure I can wear a mask every time I go out. | 4 | 5 | 4 | 4 | 5 | 5 | 4 | 4 | 4 | 4 |
| If I feel uncomfortable, I will go to the hospital in time. | 5 | 4 | 4 | 4 | 4 | 5 | 4 | 5 | 4 | 4 |
| Even I am not sick, I still stick to wearing a mask. | 4 | 5 | 3 | 4 | 4 | 5 | 3 | 1 | 4 | 4 |
| I have high-risk factors for contracting COVID-19 | 5 | 4 | 3 | 2 | 5 | 3 | 1 | 3 | 3 | 2 |
| Maybe one day I will be infected with novel Coronavirus. | 4 | 4 | 3 | 2 | 4 | 2 | 5 | 2 | 3 | 1 |
| I have a high probability of contracting COVID-19. | 4 | 5 | 3 | 2 | 5 | 3 | 1 | 3 | 3 | 1 |
| Before the outbreak is over, I am at high risk of getting COVID-19. | 4 | 4 | 3 | 2 | 4 | 1 | 1 | 2 | 3 | 2 |
Note: 1 = strongly disagree, 2 = disagree, 3 = not sure, 4 = agree, 5 = strongly agree.
The responses of the 10 respondents to each item
| Correlation | Perceived severity | Perceived benefit | Perceived barriers | Self-efficacy | Perceived susceptibility |
|---|---|---|---|---|---|
| Perceived severity | 1 | ||||
| Perceived benefits | −0.087** | 1 | |||
| Perceived barriers | 0.359** | −0.513** | 1 | ||
| Self-efficacy | −0.178** | 0.763** | −0.589** | 1 | |
| Perceived susceptibility | 0.377** | −0.328** | 0.541** | −0.415** | 1 |
Significantly correlated at 0.01 level (bilateral).
Correlation among factors
3.3. Structural Equation Model of Public Behavior When Wearing Masks during the Epidemic
Structural equation model includes measurement model and structural model. Perceived severity, perceived benefits, perceived barriers, self-efficacy and perceived susceptibility were included in the model. The factor load of 21 items in the scale was all higher than 0.5, the combined reliability of the five dimensions of the scale was all higher than 0.6, and the average variance extract of the five dimensions was all higher than 0.5. Therefore, the scale had good validity. The fitting index of measurement model is as follows: Chi-Square/DF = 4.755 < 5, GFI = 0.947 & GT; 0.9, AGFI = 0.933 & GT; 0.9, CFI = 0.966 > 0.9, RMSEA = 0.048 < 0.08, all within the acceptable range, indicating that the model and the survey data are compatible as a whole and the model is relatively scientific and effective. In the structural equation model, self-efficacy and perceived susceptibility have a direct impact on behavior, with path coefficients of 0.40 and −0.15 respectively, indicating that self-efficacy positively affects behavior, while perceived susceptibility negatively affects behavior. In other words, the stronger self-efficacy is, the more compliance is with the behavior of wearing masks during the epidemic. The lower the susceptibility, the stronger the compliance with wearing masks during the epidemic. Perceived severity, perceived benefits and perceived barriers play a mediating role in the public behavior of wearing masks. Perceived severity has an effect on the public’s behavior of wearing masks through perceived susceptibility, with a path coefficient of 0.41. Perceived benefits has an effect on the public behavior of wearing masks through self-efficacy and perceived susceptibility, and the path coefficient is 0.68 and −0.35 respectively. Perceived barriers has an effect on the behavior of the public wearing masks through self-efficacy, with a path coefficient of −0.28 (see Table 4 and Figure 2 for details).
| Latent variables | Independent variable | β | Unstd. | S.E. | t-value | p |
|---|---|---|---|---|---|---|
| Perceived severity | v1 | 0.77 | 1.00 | |||
| v2 | 0.69 | 1.07 | 0.05 | 23.84 | <0.01 | |
| v3 | 0.81 | 1.13 | 0.05 | 24.84 | <0.01 | |
| Perceived benefits | v4 | 0.76 | 1.00 | |||
| v5 | 0.84 | 1.25 | 0.04 | 34.33 | <0.01 | |
| v6 | 0.78 | 1.05 | 0.03 | 31.38 | <0.01 | |
| v7 | 0.81 | 1.31 | 0.04 | 32.73 | <0.01 | |
| v8 | 0.68 | 1.24 | 0.05 | 26.86 | <0.01 | |
| Perceived barriers | v9 | 0.79 | 1.00 | |||
| v10 | 0.81 | 1.07 | 0.03 | 32.69 | <0.01 | |
| v11 | 0.84 | 1.15 | 0.03 | 34.45 | <0.01 | |
| v12 | 0.61 | 0.85 | 0.03 | 24.83 | <0.01 | |
| Self-efficacy | v13 | 0.78 | 1.00 | |||
| v14 | 0.86 | 1.30 | 0.04 | 37.29 | <0.01 | |
| v15 | 0.87 | 1.36 | 0.04 | 38.43 | <0.01 | |
| v16 | 0.78 | 1.10 | 0.03 | 33.17 | <0.01 | |
| v17 | 0.83 | 1.34 | 0.04 | 35.79 | <0.01 | |
| Perceived susceptibility | v18 | 0.84 | 1.00 | |||
| v19 | 0.84 | 0.99 | 0.02 | 40.69 | <0.01 | |
| v20 | 0.89 | 1.06 | 0.02 | 45.15 | <0.01 | |
| v21 | 0.83 | 0.96 | 0.02 | 40.58 | <0.01 |
Parameter estimation in the structural equation model
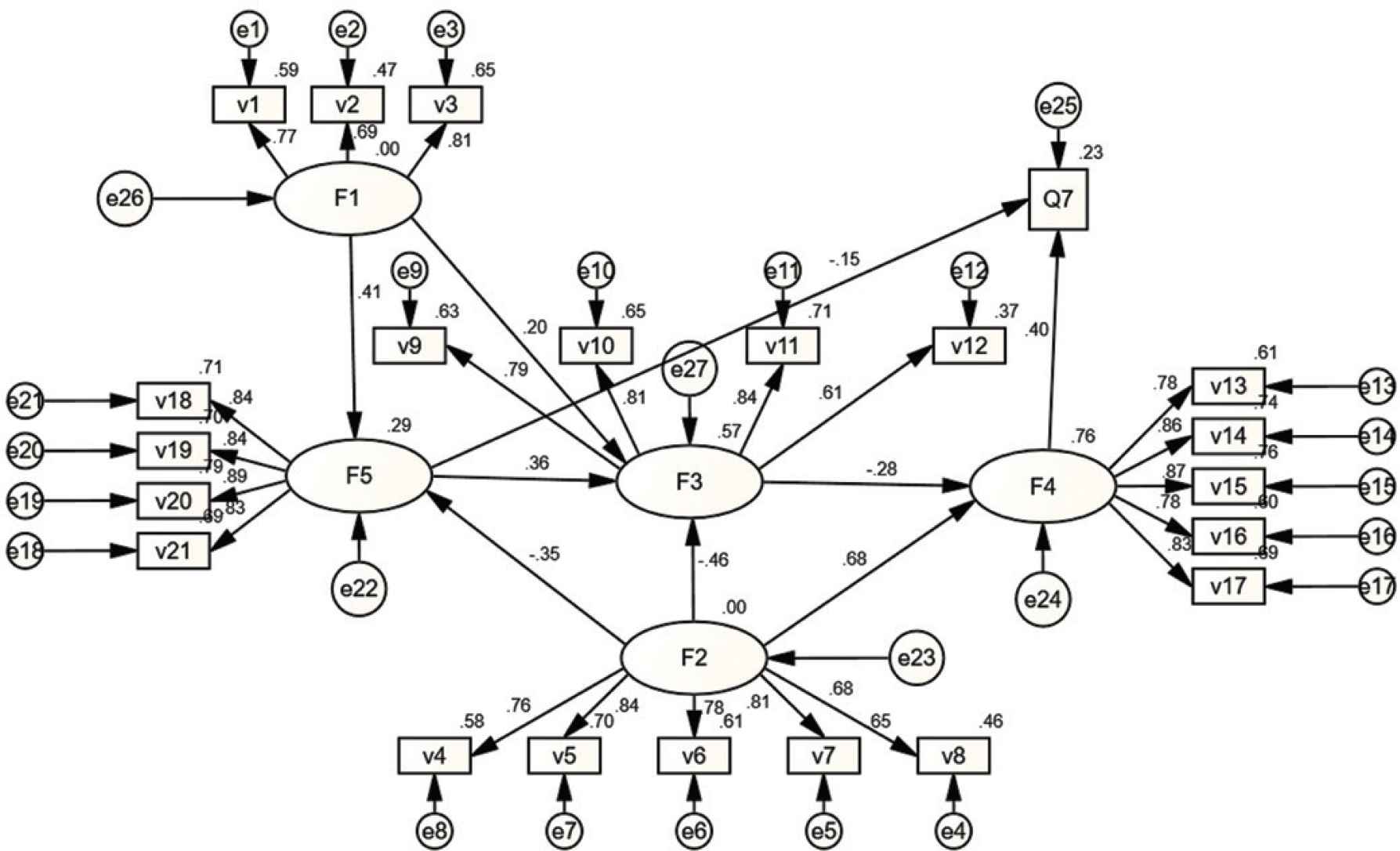
Structural equation Model. Note: F1: perceived severity, F2: perceived benefits, F3: perceived barriers, F4: self-efficacy, F5: perceived susceptibility, Q7: behavior stage; The path coefficient in the figure is the standardized coefficient, and the path coefficient in the figure is statistically different (p ≤ 0.05). v1–v21: Entry.
4. DISCUSSION
4.1. Analysis of the Current Situation of the Public Wearing Masks during the Epidemic
The five stages of innovators, early adopters, early public, late public, and laggards of the public wearing masks during the epidemic were scored 5 points, 4 points, 3 points, 2 points, and 1 point. The overall average score of 4.01 (3.95, 4.06). During the epidemic, the public are early adopters of wearing masks. This is consistent with the research results of Sim et al. [4], Zai et al. [5] and Zhan et al. [6] on the behavior of public wearing masks [6]. There were 625 innovators (39.0%), 570 early adopters (35.6%), 249 early public (15.5%), 110 late public (6.9%) and 49 laggards (3.1%). Therefore, during the epidemic, the innovative act of wearing masks by the public was carried out in depth, during which the government played an important role with the high frequency and multi-form publicity of personal protection measures.
Demographic characteristics can influence the behavior of the public to wear masks during the epidemic. Through one-way analysis of variance, eight factors were obtained, including age, education level, religion, marital status, occupation, whether there were confirmed cases in the city of the resident, whether any of the family or friends infected with COVID-19 and whether they smoked. These factors had a significant impact on the behavior of the public wearing masks during the epidemic period.
In terms of age distribution, residents aged 18–25 have an earlier stage of innovation behavior on the whole, and young people can get information faster and more easily to be exposed to information related to COVID-19 prevention, so they adopt healthy behaviors to prevent diseases earlier. The overall stage of innovation behavior of residents over 60 years old is relatively backward, which is related to the elderly’s weak ability to accept new information and stubborn and backward thinking. It is inconsistent with the results of a telephone survey conducted by Taylor et al. [7]. This may be due to the fact that the survey was conducted in the early stage of the prevalence of COVID-19, and that the elderly were slower to obtain protective measures and lower in the level of healthy behavior than the young. However, once the elderly accept this health behavior, it will last for a long time and will not be easily changed. In terms of educational background, residents with the highest educational background in high school and below have a low level of cognition of disease-related knowledge and a weak ability to acquire the latest knowledge, so they have a weak behavioral ability to take proper preventive measures. People with a bachelor’s degree or above have a higher literacy level. They have a strong ability to prevent and control diseases and can take correct measures to prevent COVID-19, which is consistent with the research results of Kuo et al.’s [8] risk awareness and prevention behavior of avian influenza and Lau et al.’s [9] prevention behavior in the H5N1 epidemic period. In terms of marital status, the married people are more obedient to wearing masks during the epidemic than unmarried, divorced or widowed residents. Due to the sense of family responsibility, married people pay more attention to their own health or the health of family members, which is consistent with the research of Tang and Wong [10]. People who believe that there are confirmed cases in their city have higher levels of wearing masks than those who do not know whether there are confirmed cases in their city. People who have quit smoking or never smoke are more compliant to wearing masks than those who smoke. Therefore, people with good health habits are more likely to take effective measures to protect themselves during the epidemic than those with bad health habits. When publicizing the knowledge and protective measures about the virus during the epidemic period, it is necessary to take into account the residents with low education level and long age, take pictures, videos and other health communication forms that do not require high level of cultural knowledge for health communication, expand the spread and coverage of health information, and make more people take health protective measures to effectively prevent diseases.
4.2. Analysis of the Public’s Behavioral Health Beliefs in Wearing Masks during the Epidemic
The scores of self-efficacy, perceived benefits, perceived severity, perceived barriers and perceived susceptibility ranged from 1 to 5 in order from low to high.
The average score of self-efficacy was 4.00 (3.96, 4.04), which was higher among five stages. Residents’ attention to the prevention of COVID-19 information, their awareness of going to the hospital voluntarily due to physical discomfort, their correct choice despite of illness and their insistence on wearing a mask have an impact on their self-efficacy. Thus, it can be seen that COVID-19 information can be effectively released during the epidemic period, and the public should be encouraged to seek medical treatment in time when they are sick. This will have an important impact on the self-efficacy of the mask wearing behavior during the epidemic.
The average score of perceived benefits was 4.00 (3.96, 4.03), which was higher among five dimensions. The satisfaction of benefiting from wearing a mask, the certainty that wearing a mask reduces the risk of being infected by COVID-19 for oneself and the family, and the sense of responsibility to one’s family and oneself positively affected the perception of benefits. Therefore, the effective prevention of infection by wearing masks by the public during the epidemic, and the publicity and popularization of the impact of wearing masks on their own health and the health of their families play a vital role in improving the public’s awareness of the benefits of wearing masks during the epidemic.
The average score of perceived severity was 3.14 (3.10, 3.18), which was medium. The average score of perceived susceptibility was 3.23 (2.42, 4.04), with the lowest score. The impact of illness on one’s relationship with family and friends, the public’s perception of the long duration of the epidemic and the threat of the disease to life, in turn, have a positive impact on the perceived severity. The public’s perception of the possibility of future illness, the perception of whether they have disease influencing factors and the probability of their infection with virus will influence the public’s perceived susceptibility. Therefore, under the premise of not affecting the normal life of the public, if the government and the media strengthen publicity on the duration of the epidemic, the general susceptibility of the population, and the harm of COVID-19, it will help improve the public’s cognition for the extent of severity and susceptibility of the virus. However, it should be noted that the government and the media’s overemphasizing the severity of COVID-19 will definitely increase the psychological burden of the public and patients with COVID-19 and, subsequently, cause social panic. Meanwhile, the government and the media are suggested to achieve precise health communication and adopt different intervention measures for different groups of people.
The average score of perceived barriers was 2.42 (2.37, 2.46), which was low. The discomfort of wearing a mask, the aversion to learning to wear a mask correctly, the uncertainty about the effectiveness of wearing a mask, and forgetting to wear a mask due to negligence all have positive effects on the perception of disability. Therefore, when promoting the correct way of wearing masks, it is necessary to adopt a popular way as far as possible, so as to improve the public’s enthusiasm for learning how to wear masks correctly and develop good healthy habits. The repeated emphasis in various forms on the usefulness of wearing masks for virus prevention and the adoption of appropriate life tips will affect the public perception of the barrier of wearing masks during the epidemic.
4.3. Analysis of Influencing Factors of Public Behaviors of Wearing Masks during the Epidemic
The structural equation model showed that self-efficacy and perceived susceptibility had significant direct effects on the public wearing masks behavior during COVID-19. Self-efficacy is the most important factor influencing the public wearing masks behavior during the epidemic, and it has a positive effect on the behavior of wearing masks, which is consistent with the research results of Babatunde [11], Li [12] and others. Therefore, relevant departments should be coordinated to improve the public’s perceived susceptibility, and at the same time, the public’s self-efficacy should be improved through health education and health promotion, so as to appeal for more people to wear masks.
There is a mediating effect in the structural equation model. The perceived severity, perceived benefits and barrier perception have significant mediating effects on the public wearing masks behavior during COVID-19 epidemic. Self-efficacy and perceived susceptibility are mediating variables in this model. Self-efficacy is the most important mediating variable, which is consistent with the research results of McNeill et al. [13] and Ling et al. [14]. Self-efficacy is the mediating variable of perceived barriers and perceived benefits. The perceived benefits has the greatest influence on self-efficacy. The higher the perceived benefits, the higher the self-efficacy. The greater the risk awareness of COVID-19 infection among the public, the greater the self-efficacy of the public, and the more likely it is to promote the implementation of mask wearing. Therefore, health education practitioners should guide the public to wear masks scientifically to emphasize their preventive effect on COVID-19. Perceived susceptibility is a mediating variable of perceived severity and perceived benefits. Perceived severity has the greatest impact on perceived susceptibility. The more serious the consequences of COVID-19 are considered by the public, the stronger the awareness that they may contract COVID-19. Therefore, health education practitioners should appropriately increase the publicity of the harm caused by COVID-19.
4.4. Limitations
This study also has some limitations. First, the nature of cross-sectional data limited the analysis of causal relationships between variables. Secondly, due to the impact of the epidemic, the questionnaires for the study were mainly distributed online. And the respondents’ answers were so uneven that the validity of questionnaires could not be guaranteed. All above may easily lead to data bias and serial errors. Third, questionnaires and the collected data used for investigation are presented in the form of self-report, which may cause the difficulty of elimination of the recall bias, thus, affects the scientific nature and reliability of the results to some extent.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
HR and DT are responsible for questionnaire design, data analysis and thesis writing; SC is responsible for translating the thesis; W. Yibo is the corresponding author; WX is responsible for thesis guidance; W. Yujie and SY are responsible for distributing and collecting the questionnaire.
FUNDING
To the key research base of
ACKNOWLEDGMENTS
Thanks to Li Yunshan of Shandong University for her support in data processing. We would like to thank Hou Qiang, Wang Wenjin, Xie Yanfei, Zhang Huihui, Li Liting, Liu Xiaofeng and Zhang Lu from Changzhi Medical College for their contributions in the questionnaire.
REFERENCES
Cite this article
TY - JOUR AU - Hou Ruyi AU - Duan Tingyu AU - Sui Chunying AU - Wu Yibo AU - Wang Xiujun AU - Wang Yujie AU - Sun Yu PY - 2021 DA - 2021/01/28 TI - Investigation of the Risk Awareness of Wearing Masks by the Public during COVID-19 According to the Health Belief Questionnaires of Shanxi Province Residents JO - Journal of Risk Analysis and Crisis Response SP - 168 EP - 175 VL - 10 IS - 4 SN - 2210-8505 UR - https://doi.org/10.2991/jracr.k.210111.001 DO - 10.2991/jracr.k.210111.001 ID - Ruyi2021 ER -