
Trend of application of World Health Organization control strategy of tuberculosis in Egypt
- DOI
- 10.1016/j.jegh.2014.01.003How to use a DOI?
- Keywords
- Egypt; BCG vaccination; Coverage rate; Mortality rate; TB Morbidity rates; Tuberculosis control
- Abstract
World Health Organization (WHO) control policy for tuberculosis (TB) includes Bacillus Calmette-Guérin (BCG) vaccine at birth, case detection, and treatment of cases with directly observed therapy short-course (DOTS). This policy has been applied through the Ministry of Health and Population in Egypt for more than 30 years. The controversies about the efficacy of the BCG vaccination against TB in adults initiate some suggestions for its discontinuation from compulsory vaccinations in countries with low incidence of TB. The present work aimed to study the trend of applying the WHO control policy for TB in Egypt among the Egyptian population throughout the last 20 years (1992–2011). The documented database of the country, bibliographic review on MEDLINE, published studies and reports, WHO and EMRO databases that covered the period from 1992 to 2011 were used in this study. The incidence rate of all forms of TB (pulmonary and extrapulmonary) dropped by 50% from 34 cases to 17 cases per 100,000 population, as well as the prevalence rate declined by 60.6% from 71 cases per 100,000 population throughout the last 20 years. Case detection and treatment success rates have increased throughout the studied period while it flat-lined over the past 6 years which may need attention. The results of this study introduce an evidence-based recommendation for continuation of the WHO TB control policy in Egypt towards elimination of the disease.
- Copyright
- © 2014 Ministry of Health, Saudi Arabia. Published by Elsevier Ltd.
- Open Access
- This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Tuberculosis (TB) remains a major global health problem. It ranks as the second leading cause of death from an infectious disease worldwide, after the human immunodeficiency virus (HIV). The latest estimates by the World Health Organization (WHO) reported that there were 9 million new cases in 2011 and 1.4 million TB deaths [1]. Moreover, it is one of the top 10 causes of global mortality and affects low-income countries in particular. About half a million children (0–14 years old) are ill with TB, and 64,000 children died from the disease in 2011 [2]. In Egypt, TB is considered the third most important public health problem after schistosomiasis and hepatitis C [3,23]. The objectives of WHO in TB control policy are to reduce mortality, prevalence and incidence of TB. The basis of this policy for TB control depends on early case detection, proper treatment of cases with directly observed therapy short-course (DOTS), in addition to the compulsory BCG vaccination [4,5]. In 1996, the National TB program of Egypt took action to tackle low adherence of patients to TB treatment and began implementation of the DOTS program [6]. This action improved the average rate of defaulting in Egypt in 2008 to 4% [7]. Clinical trials have demonstrated conflicting results regarding BCG vaccine efficacy. Meta-analytic reviews have estimated the vaccine efficacy in preventing any type of TB at approximately 51% [8]. The protective effect of BCG vaccine against disseminated TB in the newborn is estimated to be 78%. Although generally the duration of the BCG vaccine protection is not well-established, one follow-up study demonstrated a protective effect for up to 60 years [9]. The International Union against Tuberculosis and Lung Disease suggested that routine BCG vaccination should be discontinued when the notification rate of pulmonary TB reaches less than 5 per 100,000 population per year [10]. One of the targets of the United Nations millennium development goals, by 2015, is to halt the mortality and morbidity indicators of TB, improving the case detection rate to reach 70% and treatment success rate to reach 85%. The present study aimed to present the trend of the application of the WHO TB control policy in Egypt throughout the last 20 years (1992–2011).
2. Methodology
2.1. Collection of data
- 1.
Data about immunization coverage rates of the compulsory BCG vaccination for Egyptian children, under 5 years old mortality rates due to TB, morbidity and mortality rates of TB of all forms in all age groups, case detection and treatment success rates of TB were used in the present study.
- 2.
- 3.
The data were revised and filtered according to documentation; all non-documented data were excluded from the final statistical analysis.
2.2. Statistical analysis of the collected data
Statistical models are used to identify the time trend of the above-mentioned predictor variables of TB. Pearson correlation coefficient and linear regression models were used to study the relationships between the predictor variables (e.g., the BCG immunization coverage, case detection rate and treatment success rate) and the outcome of interest (e.g., morbidity and mortality rates of TB) using SPSS version 18.0. The significance level was considered at P-value <0.05.
3. Results
Statistical analysis of the collected data revealed that there was a high statistically significant increase in the coverage rate of compulsory BCG vaccination during the last 20 years (r = 0.7, P = 0.001). This increase was in two steps from 92% to 95% between the years 1992 and 1993, and the second step was between the years 1996 and 1997 from 95% to 98% with few exceptions as shown in Fig. 1. In 1998 and in 2006, there was an increase in the coverage rate reaching 99%.
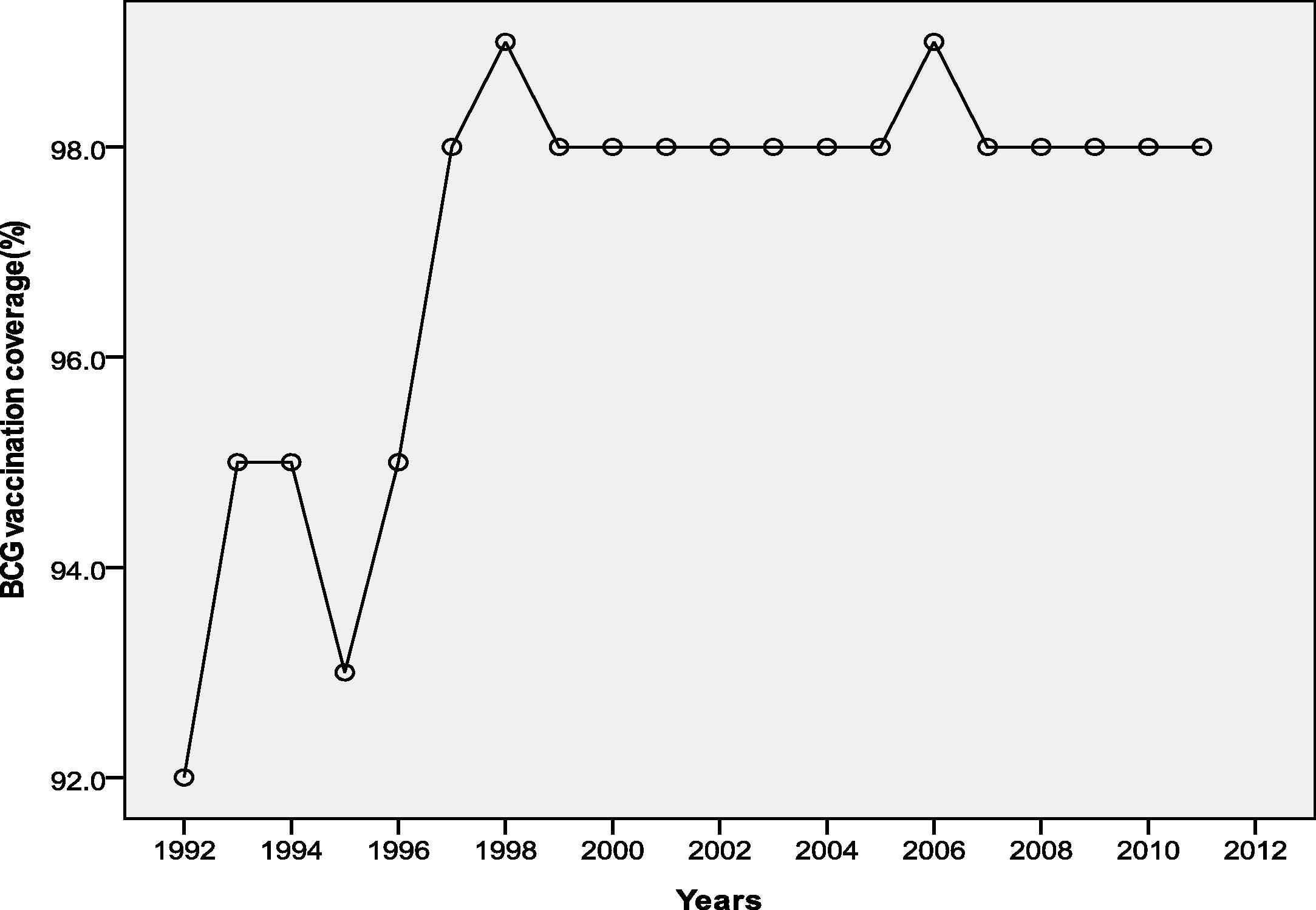
Trend of BCG immunization coverage in Egypt during the period 1992–2011.
The TB case detection and treatment success rates were increasing throughout the duration (1992–2011) with a fluctuating trend from progression to regression and so on with a plateau over the past 5 years (Figs. 2 and 3, respectively).
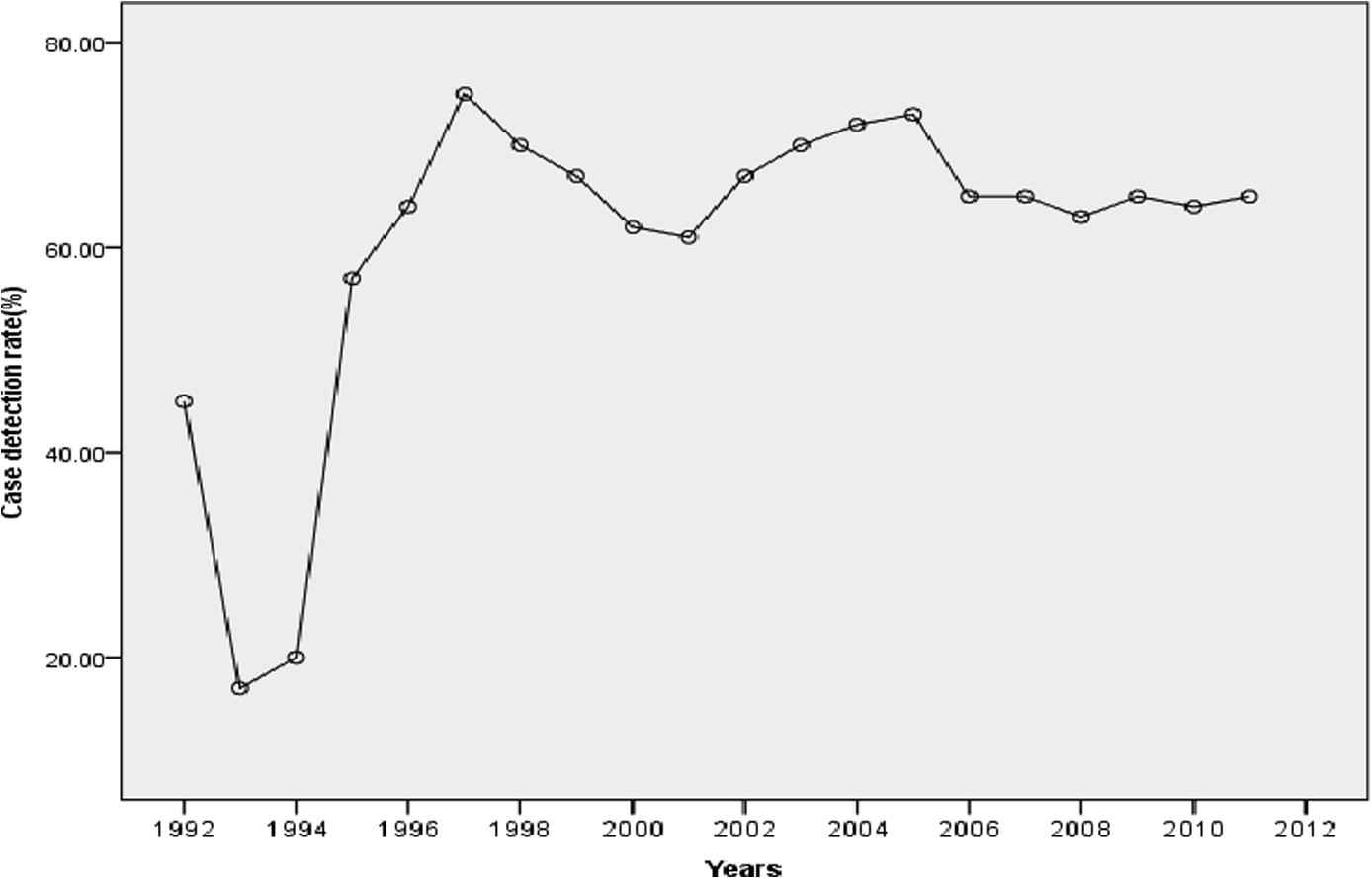
The trend of TB case detection rate in Egypt during the period 1992–2011.
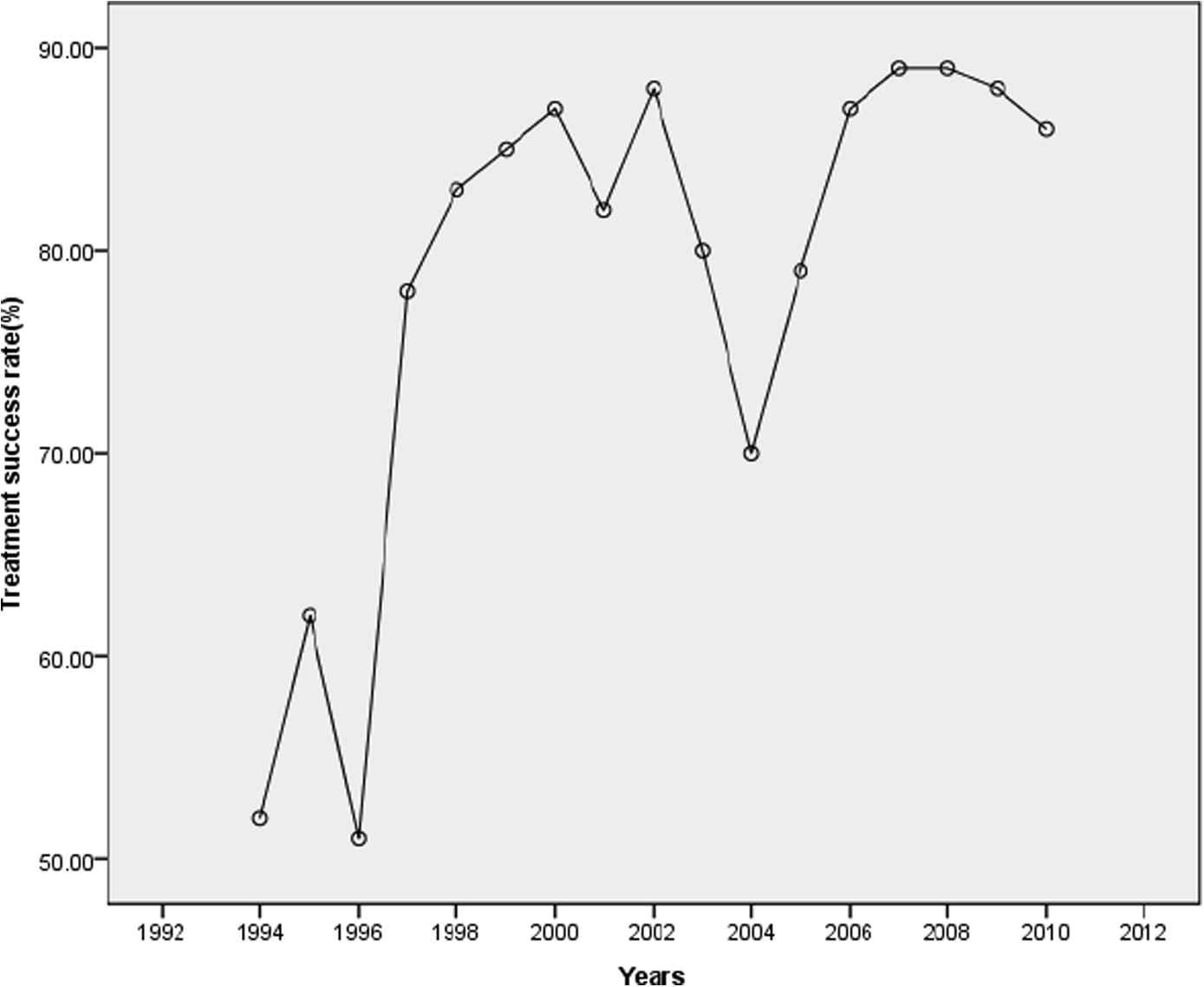
The trend of treatment success rate in Egypt during the period 1992–2011.
Moreover, severe declines were observed in the trend of the TB mortality rate per 100,000 population as well as in the under 5 years old TB mortality rate per 1000 live births during the period 1992–2011 (Figs. 4 and 5, respectively), as there were significant inverse correlations between the time in years and the rates of TB mortality and under 5 years old mortality (r = −0.85, P < 0.0001 and r = −0.99, P < 0.0001, respectively).
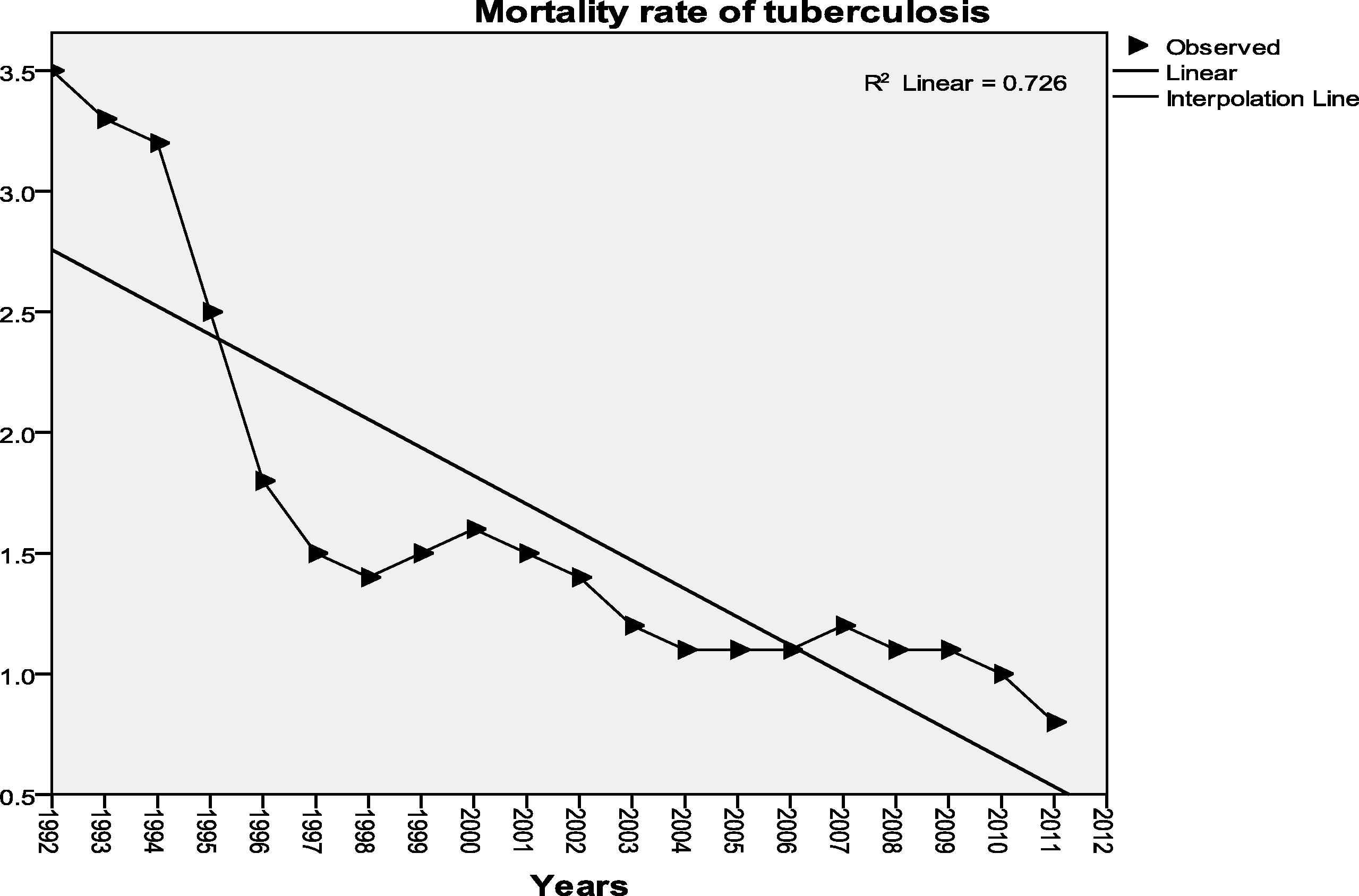
Trend of mortality rate of TB in Egypt during the period 1992–2011.
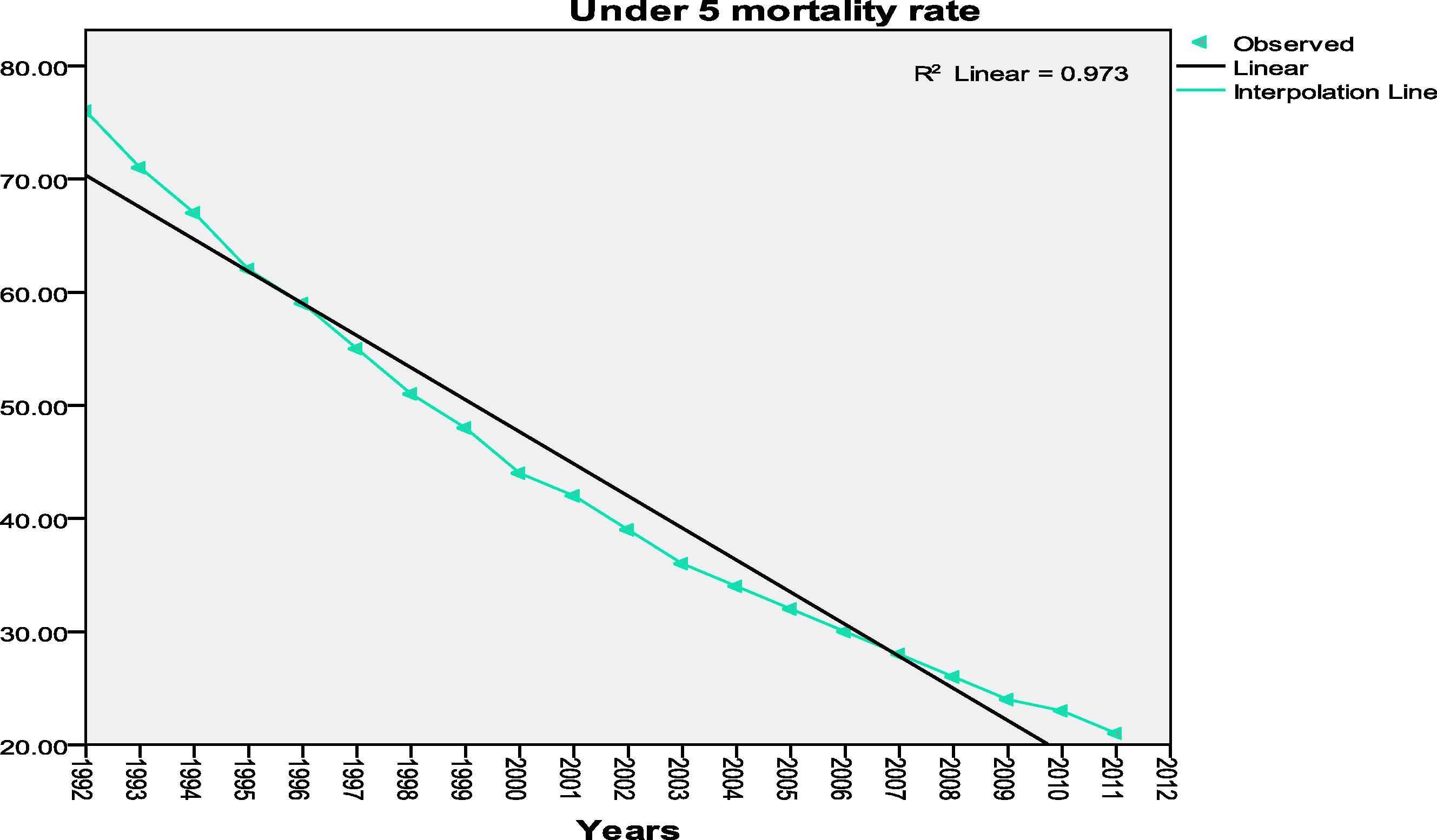
Trend of under 5 mortality rate of TB among the Egyptian children during the period 1992–2011.
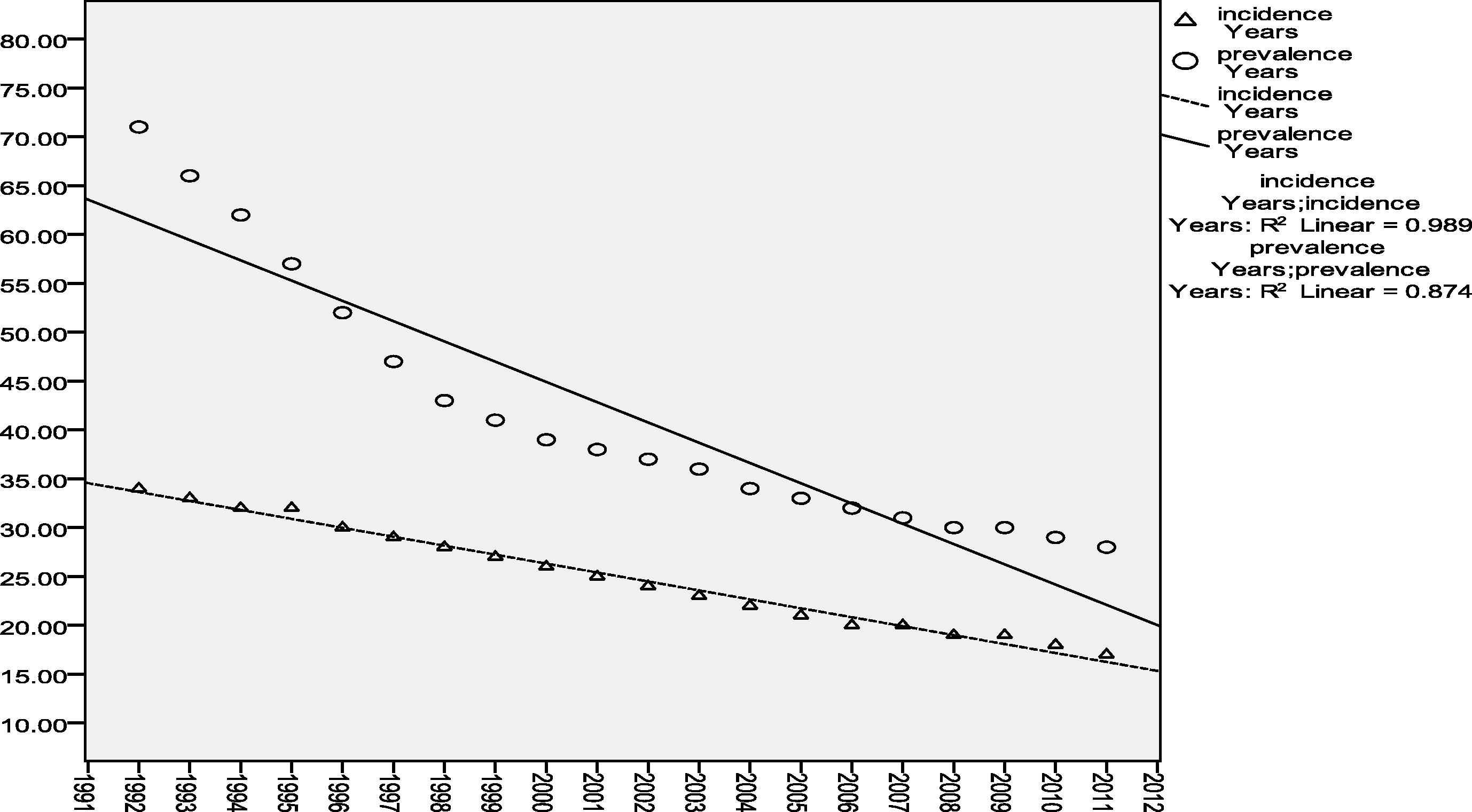
Statistically significant inverse correlations were also detected between the time in years and the TB morbidity rates per 100,000 population (incidence and prevalence rates; r = −0.99, P < 0.0001, and r = −0.94, P < 0.0001, respectively) (Fig. 6).
Trend of TB morbidity rates in Egypt during the period 1992–2011.
There were significant inverse correlations between the BCG vaccination coverage rate and the rates of TB morbidity and mortality, and under 5 years old mortality (Table 1). There were also significant inverse correlations between the rates of case detection and treatment success of TB, and the rates of TB morbidity and mortality, and under 5 years old mortality.
| Incidence rate | Prevalence rate | Mortality rate | Under 5 years old mortality rate | |||||
|---|---|---|---|---|---|---|---|---|
| R | P-value | R | P-value | r | P-value | R | P-value | |
| BCG coverage rate | −0.74 | <0.0001 | −0.86 | <0.0001 | −0.86 | <0.0001 | −0.77 | <0.0001 |
| Case detection rate (%) | −0.57 | 0.008 | −0.72 | <0.0001 | −0.84 | <0.0001 | −0.63 | 0.003 |
| Treatment success rate (%) | −0.7 | 0.001 | −0.82 | <0.0001 | −0.75 | <0.0001 | −0.75 | 0.001 |
Correlations between BCG vaccination coverage rate and the rates of TB (case detection, treatment success, morbidity and mortality, and under 5 years old mortality rates) in the period 1992–2011.
4. Discussion
The WHO declared TB a global public health emergency in 1993. Starting in the mid-1990s, efforts to improve TB care and control intensified at national and international levels. WHO developed the DOTS strategy, diagnosis using sputum smear microscopy, a regular supply of first-line anti-TB drugs, short-course chemotherapy and a standard system for recording and reporting the number of cases detected by national TB control programs (NTPs) and the outcomes of treatment [1]. The WHO also recommends neonatal BCG vaccination in countries with a high prevalence of TB as one of the preventive measures of TB control [2]. It is used in over 150 countries and is mainly given in the neonatal period [13]. In Egypt, BCG vaccination became compulsory in all governorates of Egypt since 1974 [14].
In the current work, the trend of application of the WHO control strategy for TB in Egypt in the form of the rates of case detection, treatment success, and mandatory coverage of BCG vaccine, and the efficacy of this strategy on the burden of TB among Egyptians in the last 20 years (1992–2011), were studied using statistical analysis of the documented data.
Marked improvement was noticed in the percentage of newly notified TB cases (case detection rate), including relapses. Moreover, the improvement was extended to reach the percentage of newly registered smear-positive (infectious) cases that were cured or in which a full course of treatment was completed (DOTS treatment success rate).
It was observed that the TB case detection rate has improved from 45% to 65% while the treatment success rate has improved from 52% to 86% with marked fluctuation between increase and decrease and so on throughout the studied period (1992–2011). The most prominent two peaks in the case detection rate were observed in 1997 and 2005, where it reached 75% and 73%, respectively. Similarly, the most prominent peak of increase in the DOTS treatment success rate was in the years 2007 and 2008 where it reached 89% (Figs. 2 and 3). It is observed that the treatment success rate has declined slowly after the second peak to reach 86%, which is still above the global target (85%).
It was also noticed that in the past six years, the case detection rates have become flat (leveled off) at 65% (Fig. 2), which is an alarming sign because it is less than the global target of 70%. However, the two statements may need more attention from the Egyptian national TB control program.
Strong inverse correlation was observed between TB case detection rates, treatment success rates and the rates of TB under 5 years mortality, and TB mortality and morbidity (incidence and prevalence rates) (Table 1). Egypt was classified as one of the 36 worldwide countries having achieved the global targets in both case detection and treatment success under DOTS [11]. However, WHO has identified five priority actions for further improvement of case detection and treatment success rates, as well as for more progression towards 2015 global targets [24]. These five actions include: better efforts to reach the missed cases through instituting mandatory notification and reporting systems in private and non-governmental health facilities. Another priority is addressing Multiple Drug Resistant (MDR-TB) cases through proper diagnosis and better supply of the effective treatment [24].
The currently recommended WHO approach to TB care and control is the Stop TB Strategy, launched in 2006. This Strategy was linked to new global targets for reductions in TB cases and deaths that were set for 2015 as part of the Millennium Development Goals (MDGs) and by the Stop TB Partnership. The targets are that TB incidence should be falling by 2015, and that prevalence and death rates should be halved compared with their levels in 1990 [1]. In the present study, statistically significant declines in the trend of TB morbidity (incidence and prevalence) and mortality rates with time were detected during the period 1992–2011. The incidence rate of all forms of TB (pulmonary and extrapulmonary) dropped by 50% from 34 cases per 100,000 population in the year 1992 to 17 cases per 100,000 population in the year 2011. The TB prevalence rate declined also throughout the last 20 years by 60.6% from 71 cases per 100,000 population in 1992 to 28 cases per 100,000 population in 2011 (Figs. 4 and 6). These results indicate that TB is regressing in Egypt, thus it was ranked by WHO as a country with intermediate incidence of TB in the Eastern Mediterranean Region (EMR).
On the other hand, the protective efficacy of BCG remains controversial, varying from 0% to 80% in different populations and geographic regions [15]. However, BCG currently remains the only vaccine available, particularly for severe forms of TB in children. Various explanations for the variability of BCG efficacy in the different trials and populations are still under study, including latitude variation, differences in vaccine strain, vaccine dose, virulence of Mycobacterium tuberculosis strains, genetic make-up of vaccinees, nutritional status of vaccinees and methodological differences [9,16]. In this work, the compulsory vaccination coverage rate of BCG was significantly increased during the last 20 years (1992–2011) among children in Egypt, with two peaks of increase in the years 1998 and 2006, where it reached 99% (Fig. 1).
The meta-analysis of data from 14 prospective trials and 12 case-control studies of BCG efficacy indicates that vaccination with BCG significantly reduces the risk of TB by an average of 50%. This level of protection persists across a number of subgroups of the studies defined by age at vaccination and study design. Age at vaccination was not a significant predictor of BCG efficacy. Vaccination with BCG was significantly associated with reduction in pulmonary and extrapulmonary TB [17].
In the present study, the coverage rate of compulsory BCG vaccination revealed a strong statistically significant inverse correlation with both TB morbidity indicators (incidence and prevalence rates) (Table 1). It was observed that the decline in the prevalence of the disease showed a rapid decline rate, from 71 to 43 cases per 100,000 population (34.4%) within the period 1992–1998, which is synchronous with the first peak of increase in BCG vaccination coverage rate at the year 1998, where it reached 99% coverage rate. After this first peak, the prevalence rate was decreased at a slower rate (Fig. 6).
The WHO global TB situation report mentioned that more than 50,000 deaths in children worldwide aged 0–4 years can be prevented by increasing the BCG coverage rate [5]. In the present study, a strong statistically significant inverse correlation was detected between the BCG vaccination coverage rate and the under-5 years old mortality rate (Table 1). In addition, a statistically significant decline was observed in the trend of under-5 years mortality rate during the period (1992–2011) by 72.3% from 76 to 21 deaths per 1000 live births. This decline showed a rapid rate from 76 to 51 (32.9%) deaths per 1000 live births within the first 7 years of the studied period (1992–1998), which is synchronous with the first peak of increase in the BCG vaccination coverage rate at the year 1998 where it reached 99%. After this first peak, the under-5 years mortality rate was decreased by a slower rate throughout the resting 13 years of the studied period (1999–2011) where it declined from 48 to 21 deaths per 1000 live births (Fig. 5). This finding may be in agreement with Garly et al. [18] and Roth et al. [19], where they found that the BCG vaccine enhances and promotes a T-helper-1 immune response and consequently it might reduce the mortality due to other causes of mortalities in this age in addition to the mortalities due to severe forms of TB as well.
Trunz et al. [20] found that the 100 million doses of BCG vaccine given to children every year globally prevent about 40,000 cases of tuberculous meningitis and miliary TB before these children reach their fifth birthdays, or roughly one case prevented for every 2500 inoculations.
Randomized controlled trials and case-control studies have shown variable efficacy of BCG against pulmonary TB in adults [20–22]. In the present work, the mortality rate due to TB in all age groups dropped in Egypt by 77.1% from 3.5 to 0.8 deaths per 100,000 population between 1992 and 2011 (Fig. 4), and the TB mortality rate was inversely correlated with the compulsory BCG coverage rate (Table 1).
5. Conclusion
Although TB control is a multidimensional problem, TB in Egypt is regressing in both mortality and morbidity indicators, despite the observed fluctuation in TB case detection rate that reached 65% in 2011 with a marked plateau throughout the past 6 years, which is less than the global target. WHO has succeeded to achieve a sustained treatment success rate exceeding the global target (85%) since 2006 until now; furthermore, it succeeded to maintain a higher level of the BCG vaccination coverage rate (98%) since 1997 until now. Application of the WHO control strategy for TB in Egypt is considered complementary to each other towards elimination of the disease. Even the compulsory BCG vaccination at birth may play a role in decreasing the burden of disease either through its non-specific effect on immune system and/or through prevention of progression of infection to disease. More attention is needed for improvement in case detection to reach its global target and to prevent further regression in the treatment success rate.
Conflict of interest
The authors have no conflict of interest to declare.
References
Cite this article
TY - JOUR AU - Amal Saad-Hussein AU - Asmaa M. Mohammed PY - 2014 DA - 2014/03/12 TI - Trend of application of World Health Organization control strategy of tuberculosis in Egypt JO - Journal of Epidemiology and Global Health SP - 195 EP - 202 VL - 4 IS - 3 SN - 2210-6014 UR - https://doi.org/10.1016/j.jegh.2014.01.003 DO - 10.1016/j.jegh.2014.01.003 ID - Saad-Hussein2014 ER -